
Abstract
Introduction. Propofol is a commonly used sedative medication for procedural sedation with a limited side effect profile. Although well tolerated with minimal adverse reactions, uncommon side effects have been reported. Methods. Case report of priapism in a 9-year-old male following the use of propofol for sedation in the pediatric intensive care unit (PICU) setting. The patient was admitted to the PICU for postoperative management following laryngotracheal reconstruction. On postoperative day 2, our patient was initiated on continuous infusion of propofol and he developed priapism. Propofol was then immediately discontinued, and the priapism quickly resolved without any medical or surgical interventions. Results. Priapism is a low-flow state and is considered a urological emergency requiring prompt recognition, withdrawal of suspected offending agents, and possible need for urologic consultation to alleviate complications. Although rare, priapism with propofol has been reported but never in a prepubescent male. The mechanism of propofol-associated priapism is not well understood, but it is thought that it may result from an autonomic system imbalance, leading to an increase in parasympathetic activity. In addition, propofol has been shown to affect nitric oxide–mediated smooth muscle relaxation. In our patient, we suspected propofol to be contributing factor to his priapism based on the temporal relationship between the initiation of the medication and symptoms and resolution of symptoms after propofol discontinuation. Discussion. Given the expansive use of propofol in pediatrics for sedation and anesthesia, pediatric clinicians should be cognizant of this rare adverse effect in pediatric patients with potentially disastrous complications.
Introduction
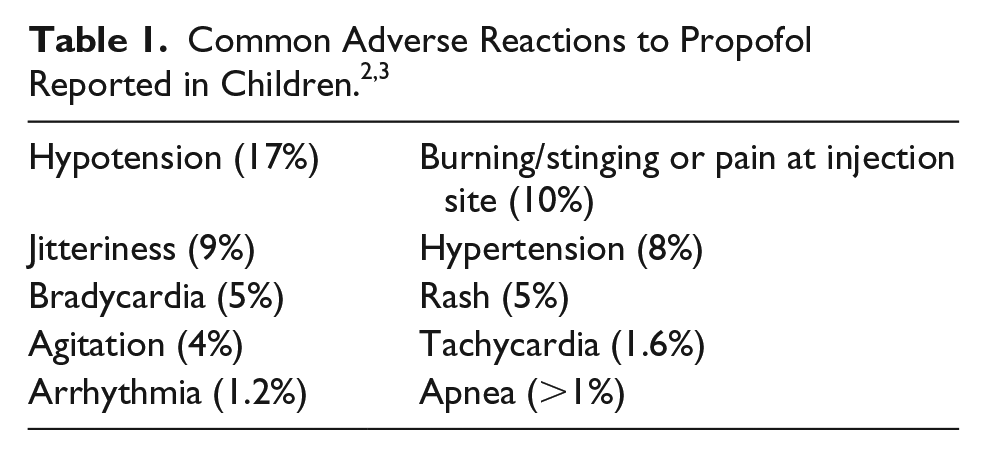
Propofol is an intravenous medication commonly used as a sedative agent in procedural and critical care situations for pediatrics. It has multiple pharmacological advantages over other agents in this population due to its rapid onset and short duration of action, as well as minimal side effects such as decreased postoperative nausea/vomiting and emergence delirium. The side effects mostly seen in the adult population such as anaphylaxis, propofol-related infusion syndrome from prolonged exposure, and metabolic decompensation are less likely to occur in the pediatric population. 1 Common adverse events in pediatric patients from the manufacturer’s prescribing information include arrhythmia, tachycardia, hypotension, hypertension, burning, stinging, rash, pruritis, and apnea (Table 1).2,3
We present a case of priapism that occurred in a pediatric patient who was on propofol for sedation in our pediatric intensive care unit (PICU), which was the youngest patient having this rare side effect among a handful of reported cases.4-7
Ethical Approval and Informed Consent
Institutional review board consent was not required since this was a case report for a single patient.
Case Report
A 9-year-old African American child (weight: 27.9 kg) with no known drug allergies and a history of premature birth (24 weeks gestational age) and severe subglottic stenosis and a chronic need for tracheostomy tube was admitted to the PICU following laryngotracheal reconstruction surgery with a right rib graft. He received rocuronium at the start of surgery and then placed on an inhalational anesthetic, continuous remifentanil infusion for analgesia, and was bolused with propofol twice during the surgery at dosages of 1 mg/kg/dose and 0.7 mg/kg/dose. The surgery was successful with no hemodynamic instability and minimal blood loss. The patient was then transferred to PICU intubated with acute respiratory failure necessitating mechanical ventilation and initiated on postoperative sedative management with versed infusion, analgesia management with fentanyl infusion, and paralytic management with cisatracurium.
Our postoperative guidelines for the care of laryngotracheal reconstruction surgery calls for prolonged intubation, typically 5 to 7 days, to allow for proper healing at the reconstruction site (Figure 1). As such, the patient will need prolonged sedation and paralytic infusions with changes to the type of medication to allow decrease tolerance and withdrawal effects. On postoperative day 1, the patient remained intubated and was continued on the medication regimen previously stated. During postoperative day 2, the patient was switched from a midazolam infusion to a propofol infusion as per our institutional guidelines. The patient was started on propofol 25 µg/kg/min and was uptitrated to 60 µg/kg/min. Approximately 4 hours after the start of the infusion, the patient had a sustained penile erection in the form of priapism lasting approximately 2 minutes. The propofol was immediately discontinued, resulting in the patient’s priapism to subside within minutes. The patient had received more than 300 mg of propofol after surgery before this adverse event.

Institution-specific guidelines for the postoperative management of laryngotracheal reconstruction surgery patients.
Discussion
Priapism is a persistent erection of the penis not otherwise associated with sexual stimulation or desire. 8 The mechanism of propofol-associated priapism is not well understood but thought that it might result from an autonomic system imbalance, leading to an increase in parasympathetic activity. 6 Also, propofol has been shown to affect nitric oxide–mediated smooth muscle relaxation. 7
Propofol-associated priapism is generally categorized into 2 states based on the penile venous blood flow. 9 Low-flow ischemic priapism, the most common form, is due to occlusion of venous outflow that can be caused by impaired relaxation and paralysis of the cavernosal smooth muscle, vascular stasis, acidosis, and tissue hypoxia. Prolonged erections in ischemic priapism can lead to structural damage of erectile tissue and even irreversible damage if a patient is identified to have priapism for over 24 hours, making this a medical emergency when it occurs. 10 High-flow, nonischemic priapism is commonly related to penile or perineal trauma. Usually, there is an injury to the cavernosal artery, which leads to increased flow through the corpora cavernosa, causing the priapism. This form of priapism does not represent an emergent situation and resolves spontaneously in up to 62% of untreated cases. 11 Both low-flow and high-flow priapism may initially be treated with watchful waiting or using ice packs and the possible need for urology consultation (Figure 2). However, aspiration, arterial embolization, or shunt therapy may be required in severe cases. 12
Priapism has also been associated with other medications, including the antihypertensive agents guanethidine, prazosin, and hydralazine. 10 A few case reports also noted antipsychotic-associated priapism with trazodone, thioridazine, and chlorpromazine due to their α-adrenergic antagonist properties. 10 However, our patient was not administered nor was previously on any of these medications. Doherty et al reported that each patient in previous cases of propofol-associated priapism was also on concomitant opioid medication. 7 Similarly, our patient was on a continuous fentanyl infusion. Opioid medications are thought to potentially decrease peripheral vascular resistance, leading to the potentiation of propofol’s effects on inducing priapism. 9
We believe that our patient experienced priapism caused by propofol because of the temporal relationship with the administration of propofol and the onset of priapism, the lack of alternative causes, and the priapism event resolving after discontinuation of the medication. Based on the probability scale developed by Naranjo et al for assessing the likelihood of an adverse drug reaction, propofol is a probable cause of the priapism in our patient (+7). 13 Questions within the tool are answered as either “yes,” “no,” or “do not know,” with points either added, subtracted, or no change depending on the answer to the specific question. Scores were determined as follows (our score; range: yes; no; do not know):
Previously published reports on this reaction (+1; range: +1; 0; 0)
Adverse event appeared after the medication was administered (+2; range: +2; −1; 0)
Adverse reaction improved after the medication was discontinued (+1; range: +1; 0; 0)
No alternative causes for the reaction (+2; range: −1; +2; 0)
Adverse reaction was confirmed by objective evidence (+1; range: +1; 0; 0)
There have been 4 other cases of propofol-associated priapism in pediatric patients documented in the literature. The first reported case was in a 17-year-old male who experienced priapism 2 hours after initiation of a propofol infusion. This case was similar to ours in the fact that the priapism occurred multiple hours after initiation of the propofol infusion. However, the patient required injections of lidocaine 0.5% with epinephrine into each corpus for management of his priapism. 4 Another pediatric case reported by Doherty et al in a 13-year-old patient who experienced priapism within minutes of receiving a propofol bolus to control movements related to underlying movement disorder. The priapism resolved within an hour after aggressive intravenous hydration. 7 Compared with the previously reported case reports, the treatment of our patient’s priapism event was the quickest and least invasive that was accomplished by prompt recognition of the priapism event and discontinuation of propofol, which led to our patient’s erection subsiding within minutes. Also, we monitored our patient very closely for recurrence of the priapism because the longer the priapism persists the higher likelihood that surgery would be necessary for treatment as was seen in the previously mentioned case reports.
One case involved a 7-year-old male who was noted to have a penile erection following surgery. The patient had received a combination of propofol, fentanyl, vecuronium, and neostigmine bromide. 14 Since the patient received all of these medications at the same time before the priapism occurring, it would be difficult to predict which medication or combination of medications resulted in priapism. Moreover, the patient’s priapism had not subsided after 12 hours lowering the probability of this priapism event being due to propofol. In contrast, there is plausible evidence that our patient’s priapism event was most likely due to propofol and not any other underlying disease state, medication, or other external factors.
Conclusion
We report a case of propofol-associated priapism in a 9-year-old patient, the youngest ever reported. With the increased use of propofol in the pediatric population, clinicians should be aware of this rare side effect that can occur in male patients of all ages as it needs to be treated promptly to avoid invasive surgical treatment or permanent penile damage.
Footnotes
Author Contributions
C.S collected the patient information, conducted literature review, and wrote the initial manuscript with significant editing and mentoring from V.R and P.K. All revisions were done by V.R and P.K.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.