
Abstract
Propofol is a commonly used sedative for the induction of clinical anesthesia and sedation maintenance in intensive care unit patients. However, in a minority of patients, prolonged infusion of propofol may cause metabolic acidosis, electrocardiographic abnormalities, arrhythmias, and rhabdomyolysis, a condition known as propofol-related infusion syndrome. If not promptly identified and managed, propofol-related infusion syndrome can be fatal. Propofol-related infusion syndrome typically occurs in critically ill patients in the intensive care unit and is less common in clinical surgical anesthesia. We herein report a case of a patient with hematospermia who developed propofol-related infusion syndrome perioperatively, receiving a large amount of propofol infusion in a short time due to agitation during anesthesia recovery. Arterial blood gas analysis indicated persistently increasing lactic acid and unresolving metabolic acidosis, leading to the patient’s transfer to the intensive care unit for further treatment. During intensive care unit treatment, the patient received continuous propofol infusion for sedation, with doses reaching up to 10 μg/kg/min, and a total infusion duration of ~8 h. We highly suspected propofol-related infusion syndrome and discontinued propofol. The patient successfully recovered after continuous renal replacement therapy. Propofol-related infusion syndrome can occur in non-critically ill patients receiving short-term propofol; hence, caution is warranted when using this drug. Early blood purification therapy is recommended for a better recovery from propofol-related infusion syndrome, and alternative sedatives should be considered as needed.
Keywords
Introduction
Propofol-related infusion syndrome (PRIS) refers to a set of specific clinical reactions that occur after prolonged high-dose (>48 h, >4–5 mg/kg/h) infusion of propofol. 1 The syndrome is commonly characterized by metabolic acidosis, electrocardiographic abnormalities, rhabdomyolysis, arrhythmias, heart failure, hyperlipidemia, hyperkalemia, hepatomegaly, among other clinical manifes-tations.2,3
Ever since PRIS was first reported in pediatric patients in Denmark in 1990, 4 numerous adult PRIS cases have also been gradually reported. 5 Due to the pharmacokinetic properties of propofol, such as its rapid onset and short half-life, it allows for quicker awakening after the infusion is stopped, 6 making it an ideal sedative for intubated patients requiring mechanical ventilation in the intensive care unit (ICU). Therefore, PRIS mostly occurs in critically ill patients treated in the ICU. 5 A multicenter prospective study assessed the incidence of PRIS in critically ill patients at 1.1%, with a mortality rate of 18%, indicating that PRIS is a rare but fatal clinical syndrome. 7 However, the occurrence of PRIS is fairly uncommon in clinical surgical anesthesia.
We herein report a suspected PRIS case of a patient who developed clinically unexplained metabolic acidosis after receiving a short-term high-dose infusion of propofol during the perioperative period, even though the patient was initially not receiving treatment in the ICU for any critical illness.
Case presentation
A 32-year-old male patient, with 175 cm height and 79 kg weight, was admitted to Xi’an Daxing Hospital on January 24, 2024, due to “hematospermia for more than half a month.”
The patient was previously healthy with no significant medical history and was not on any long-term medications. Routine preoperative examinations and laboratory test results showed no abnormalities. Physical examination was normal. The American Society of Anesthesiologists classification was Grade I. Admission diagnosis: hematospermia, seminal vesiculitis, chronic prostatitis. On January 26, 2024, at 12:40, he was admitted to the operating room with a blood pressure of 125/81 mmHg, a heart rate of 80 beats/min, and a saturation of pulse oxygen (SpO2) of 99%.
Anesthesia induction at 12:55 included propofol 50 mg, sufentanil 20 μg, midazolam 2 mg, rocuronium bromide 40 mg, and dexmedetomidine 14 mg. After successful induction, a laryngeal mask was inserted. Intraoperative anesthesia maintenance was with dexmedetomidine 0.37 μg/kg/h and remifentanil 0.10 μg/kg/min continuous infusion, along with 10 mL of sevoflurane. The surgery began at 13:10 and was uneventful, concluding at 13:50 with a seminal vesicle exploration procedure. No irrigation fluid was used during the procedure. Intraoperative blood pressure fluctuated between 100–130/55–80 mmHg and heart rate of 50–80 beats/min.
Intraoperative fluid supplementation included compound sodium chloride 1000 mL, with an intraoperative blood loss of 5 mL. At the end of the surgery, neostigmine 1 mg and atropine 0.5 mg were administered to antagonize residual muscle relaxation, and flumazenil 0.2 mg was given to promote waking. At 14:00, the laryngeal mask was removed, after which the patient showed mild agitation and hence was sent to the recovery room. The patient’s consciousness did not improve, so at 14:20, another dose of flumazenil 0.2 mg was administered with poor effect, resulting in agitation. Propofol 50 mg was intermittently injected for sedation.
The first arterial blood gas was taken at 14:50 (T1, Figure 1), showing pH 7.19, pCO2 45 mmHg, pO2 69 mmHg, Na+ 140 mmol/L, K+ 3.7 mmol/L, Cl− 105 mmol/L, Ca2+ 1.10 mmol/L, and glucose 14.7 mmol/L. At 15:50, arterial blood gas analysis showed severe lactic acidosis (T2, Figure 1), with PaO2 at 97 mmHg, PaCO2 at 30 mmHg, pH at 7.21, lactate at 11.1 mmol/L, base excess at −15.9 mmol/L, glucose at 15.1 mmol/L, and hematocrit at 44%. Consequently, 5% sodium bicarbonate 50 mL was intravenously infused. At 16:50, arterial blood gas analysis showed lactate concentration further increased to 14.9 mmol/L (T3, Figure 1). During this period, the patient exhibited progressive agitation and metabolic acidosis. Endocrinology consultation was obtained, which considered the possibility of diabetic ketoacidosis. The patient received fluid resuscitation (2500 mL over 2 h, with urine output of 2400 mL), insulin with glucose infusion, and intermittent sodium bicarbonate to correct acidosis. The anion gap was found to be 25 mmol/L. Despite these interventions, the patient’s condition did not improve. As the progressive worsening of acidosis continued, a laryngeal mask was reinserted at 17:45. During this period, the patient’s circulation remained stable, with blood pressure 95–124/63–75 mmHg and heart rate 64–94 beats/min. The patient’s body temperature remained normal throughout this period (36.7 °C), and there were no signs of conduction abnormalities or cardiac arrest. At 18:40, the patient was transferred out of the recovery room, with a total infusion of 2500 mL and urine output of 2400 mL. Propofol was used to suppress patient agitation, with a total dose of 150 mg. A computed tomography (CT) scan of the head showed no abnormalities, and the patient was transferred to the ICU at 18:55 due to unexplained lactic acidosis during the waking period, which continued to worsen.
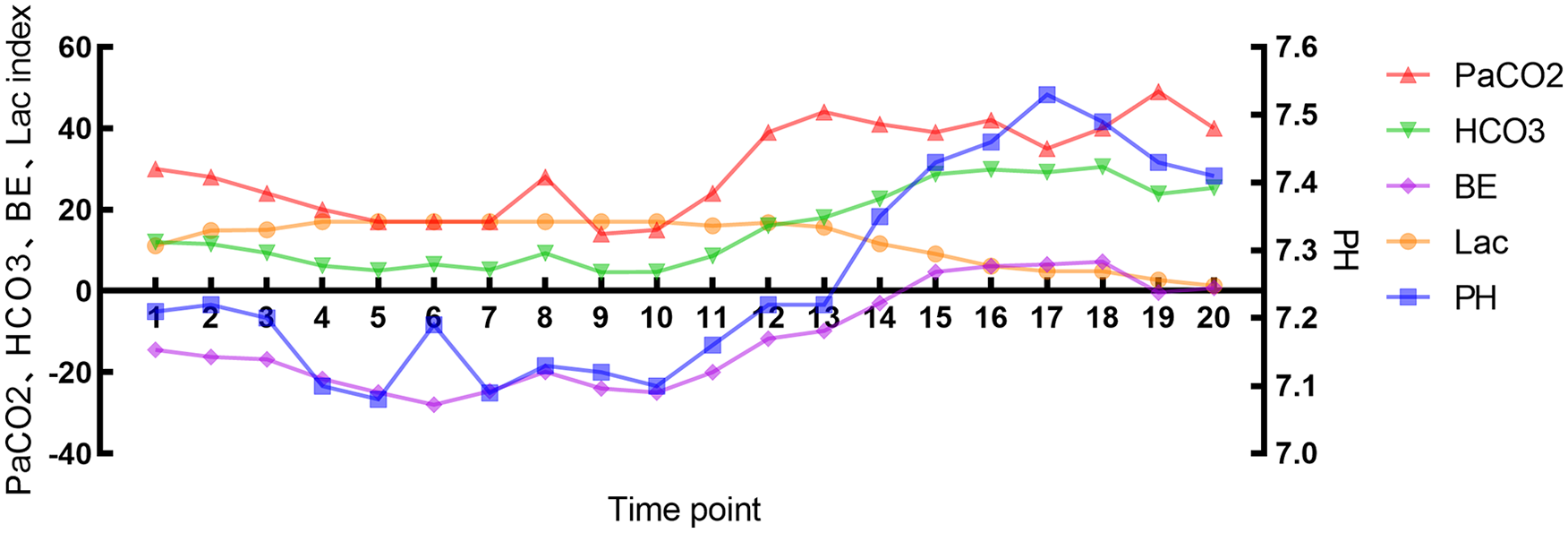
Arterial blood gas results of the patient at different time points. Time point 1 represents the date for the first arterial blood gas analysis on January 26, 2024, at 14:50. Each time point interval is 1 h.
Physical examination revealed spontaneous breathing, unconsciousness, involuntary limb agitation, equal and round pupils with light reflex present, blood pressure 105/60 mmHg, heart rate of 110 beats/min, central venous pressure 7 cm H2O, SpO2 99%, respiratory rate of 16 breaths/min, and body temperature 36.7 °C. Laboratory tests showed a white blood cell count of 4.22 × 109/L, neutrophil ratio of 9.14, Na+ 140 mmol/L, K+ 3.9 mmol/L, Cl− 106 mmol/L, and creatinine 65 μmol/L. Blood and urine cultures were collected and later found to be negative. ECG and echocardiography were performed and showed no significant abnormalities. Pulse contour cardiac output (PICCO) monitoring indicated the following: global end-diastolic index 534 mL/m2, global ejection fraction 26%, cardiac index 3.29 L/min/m2, stroke volume index 35 L/min, extravascular lung water index 6.4 mL/kg. Venous blood gas analysis showed a central venous oxygen saturation of 74% and an arteriovenous CO2 difference of 4 mmHg, suggesting adequate oxygen delivery. After ICU admission, the patient was given ventilator-assisted ventilation, remifentanil 0.10 μg/kg/min for analgesia, propofol 10 μg/kg/min, fluid resuscitation to correct acidosis and lower the blood glucose, and maintain water-electrolyte balance. Meropenem 1 g was administered every 8 h for 2 days to prevent any infection. On January 26, 2024, at 23:35, liver function tests showed the following: glutamic-pyruvic transaminase 22 U/L, glutamic-oxaloacetic transaminase 63 U/L, alkaline phosphatase 56 U/L, total bilirubin 17.1 mmol/L, direct bilirubin 8.7 mmol/L, and albumin 33.1 g/L. Renal function test showed the following: urea nitrogen 3.94 mmol/L and creatinine 75 mmol/L. Blood electrolytes test showed the following: K+ 4.57 mmol/L, Na+ 155 mmol/L, Cl− 107.2 mmol/L, and Mg2+ 0.73 mmol/L. Continuous renal replacement therapy (CRRT) was initiated at 00:00 due to persistent, uncorrectable acidosis. After literature review, PRIS was highly suspected in this patient, so propofol was discontinued at 02:42 on January 27, 2024, and midazolam was administered for sedation. The patient’s acidosis gradually improved. At 01:30, cardiac injury markers were checked, showing myoglobin 274 ng/mL (reference range: 0–121 ng/mL), creatine kinase-MB 8.03 μg/L (reference range: 0–3.38 μg/L), high-sensitivity troponin 0.219 ng/mL (reference range: 0–0.034 ng/mL), and procalcitonin 0.45 ng/mL (reference range: 0–0.8 ng/mL). On January 27, 2024, at 17:04, blood lipids test showed: triglyceride 0.64 mmol/L, total cholesterol 2.82 mmol/L, high-density lipoprotein 0.90 mmol/L, and low-density lipoprotein 1.53 mmol/L. Serum amylase and lipase were not tested. On January 28, 2024, at 08:00, midazolam was discontinued, the patient’s consciousness cleared, and the tracheal tube was removed. The general condition, respiratory, circulatory, and internal environment were stable, so the patient was transferred to the urology department on the next day.
Discussion
Since propofol is commonly used to maintain sedation in ICU patients, it is usually continuously infused over a long period within the recommended safe dosage range. However, even with strict dose control, some susceptible individuals still develop PRIS. ICU patients with prolonged exposure to propofol are the most susceptible group to PRIS. This case differs from the reported PRIS among critical patients, as it did not involve long-term infusion of propofol. However, there have been cases of non-critical patients developing PRIS after receiving a large amount of propofol infusion over a short period. These patients also exhibited some PRIS symptoms, such as unexplained metabolic acidosis and ECG changes. 8 Due to the large dosage of use in a short period, it is acceptable that there may not be other clinical manifestations2,3 besides metabolic acidosis or ECG changes without the continuous long-term use of propofol.
In this case, we considered several differential diagnoses for the patient’s severe metabolic acidosis. Transurethral resection of prostate syndrome was unlikely as no irrigation fluid was used during the seminal vesicle exploration procedure, and the patient’s sodium levels remained normal throughout. Diabetic ketoacidosis was considered, but treatment with insulin and glucose did not improve the patient’s condition. Infectious causes were also unlikely given the normal temperature, negative blood and urine cultures, and normal procalcitonin levels. The timing of the metabolic acidosis following propofol administration, the elevated cardiac injury markers, and the improvement following discontinuation of propofol strongly suggested PRIS as the most likely diagnosis.
The mechanism causing PRIS is still controversial. The prevailing theory supports that propofol blocks the mitochondrial oxidative respiratory chain function, leading to PRIS. According to the theory, propofol acts as an uncoupler during oxidative phosphorylation in mitochondria, blocking the functions of complex I, complex IV, cytochrome C, and acyl-carnitine transferase in the mitochondria. This results in the obstruction of the β-oxidation process of free fatty acids and a reduction in adenosine triphosphate (ATP) production. 6 It is important to note that due to increased energy demands during surgery or severe illness, free fatty acids derived from adipose tissue become the main energy source for skeletal and cardiac muscles. Under high-dose propofol infusion, the body’s ATP production is hindered, causing a state of energy demand and supply imbalance, leading to tissue hypoxia and metabolic acidosis. Cumulative use of propofol exceeding 240 mg/kg is one of the risk factors for inducing PRIS. 3 In this case, the patient was given ~100 mg/kg of propofol during treatment, which is far below the dangerous dose. Therefore, there may be other unidentified factors in this patient that led to the occurrence of PRIS.
Since PRIS is also considered as a condition of mitochondrial dysfunction induced by propofol, individuals with mitochondrial diseases or pathogenic mutations in mitochondrial genes may be more prone to develop PRIS. 9 Shimizu et al. 10 reported a patient with mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes who developed PRIS on the fifth day of using propofol to control seizures, with the maximum dosage of propofol reaching 5.4 mg/kg/h during treatment. In addition, Savard et al. 11 reported a case of a 27-year-old woman who developed persistent seizures 1 month postpartum and experienced PRIS on the third day of high-dose propofol administration (10.7 mg/kg/h) to control her condition. Further genetic testing revealed two pathogenic mutations in the POLG1 gene, suggesting the patient had a mitochondrial disease prior to the development of PRIS. These two case reports indicate that patients who develop PRIS may have an underlying mitochondrial gene defect. In this case, our patient denied any history of neurological conditions such as seizures, stroke, or cerebral hemorrhage, as well as any family history of mitochondrial diseases, before undergoing surgery. Notably, despite having a low risk for PRIS, the patient still developed unexplained metabolic acidosis after receiving propofol. Since propofol has been used in millions of patients since its introduction in clinical practice, and our patient did not have any risk factors before using propofol, what distinguishes the cases of PRIS that occurred after short-term propofol administration (like our case) from others? Some scholars proposed that these patients may have subclinical forms of mitochondrial diseases affecting the respiratory chain complexes or fatty acid oxidation, which become apparent after propofol infusion. 12 Mitochondrial diseases vary widely, ranging from primary diseases (possibly genetic) to secondary conditions that may affect mitochondrial function (such as untreated hyperthyroidism or hypothyroidism, diabetes, etc.).13,14 As we did not conduct genetic testing on this case, we cannot rule out the possibility of other unknown genetic factors contributing to the occurrence of PRIS.
Due to the lower incidence of PRIS in perioperative anesthesia compared to ICU patients, misdiagnosis or missed diagnosis by anesthesiologists can lead to severe consequences when PRIS occurs. Currently, there is no antidote for propofol, and successful treatment for PRIS depends on early recognition and timely discontinuation of propofol, as well as switching to other sedatives, and maintaining the patient’s electrolyte balance and hemodynamic stability. 15 For metabolic acidosis that is difficult to alleviate with sodium bicarbonate, CRRT may help improve acidosis symptoms and remove harmful water-soluble propofol metabolites.16,17 In this case, the patient achieved a good prognosis after discontinuing propofol and receiving CRRT, suggesting that early blood purification treatment can provide significant benefits for PRIS patients. For PRIS patients with severe cardiogenic shock requiring extensive use of vasopressors and inotropic drugs, mechanical circulatory support—such as ventricular assist devices or extracorporeal membrane oxygenation—can provide temporary end-organ perfusion and oxygenation. 18 PICCO monitoring indicated that the overall cardiac function of this case was stable, and therefore additional circulatory support was not needed.
In conclusion, PRIS is a rare but fatal condition caused by propofol, most commonly occurring in critically ill patients in the ICU, and is less common during perioperative anesthesia. The rarity of PRIS makes its prevention particularly challenging, especially in non-critical patients who develop PRIS during the perioperative period, as reported in this case. Therefore, early and accurate identification of PRIS and the timely discontinuation of propofol are crucial for treatment. Early blood purification therapy can aid in better recovery from PRIS. For patients who were previously healthy but developed PRIS, related genetic testing to screen for potential mitochondrial diseases or mitochondrial gene defects is recommended if feasible.
Footnotes
Ethical considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient for their anonymized information to be published in this article.
Author contributions
Haibo Zhang and Yezu Liu contributed to conceptualization, validation, formal analysis, investigation, resources, data curation, manuscript writing, and editing. Minlong Liu contributed to conceptualization, validation, manuscript writing, and editing. Bing Li contributed to conceptualization, validation, manuscript writing and editing, and supervised the study. Haima Li contributed to visualization, manuscript writing and editing, and supervised the study. All authors have read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.