
Abstract
Background. Exclusive breastfeeding is important for immunity and lack of breastfeeding during the neonatal age impedes that. Our aim was to assess the consequences of lack of breastfeeding on infants with diarrhea in the neonatal period. Methods. In this design, infants from DDSS (Diarrheal Disease Surveillance System) from 2009 to 2013 were studied. Those who did not have breastfeeding or had cessation of breastfeeding at the neonatal age constituted the cases, whereas infants who continued breastfeeding since birth or for at least 6 months since birth constituted the controls. Results. The cases more often presented at a younger age, had an illiterate mother, frequently presented with complicated diarrhea, had severe wasting, and had abnormal mental status compared with the controls. In logistic regression, after adjusting for potential confounders, infants who lacked breastfeeding at the neonatal period had an independent association with dehydrating diarrhea. Conclusions. The results of our analyses suggest that infants with diarrhea who did not have breastfeeding at the neonatal age are prone to develop some or severe dehydration.
Introduction
The advantages of breastfeeding for infants with its dose-response effects that are related to the amount of breast milk received are well demonstrated in multiple studies.1-4 Breastfeeding is known as a highly effective strategy for the prevention of infectious disease–related morbidity and mortality in infancy as well as in early childhood. 5 Human milk contains glycans including free and conjugated forms of oligosaccharides. This forms a natural immunological mechanism and also acts as soluble receptor resisting the pathogens to adhere to their target receptors on the mucosal surface of the host gastrointestinal tract. 5 Higher concentrations of α-1,2-linked fucosylated glycans in human milk protect infants against diarrhea caused by Campylobacter, calici viruses, and stable toxin of enterotoxigenic Escherichia coli, and all forms of moderate-to-severe diarrhea.5,6 Furthermore, breastfed infants and children are less exposed to contaminated fluids and foods compared with the non-breastfed infants and also are benefited by achieving optimum nutrition and nonspecific immunity. 7
Although exclusive breastfeeding during the first 6 months of life has been prioritized by international policy with promotion of early initiation of breastfeeding8,9 to improve the rate of breastfeeding, it is yet to achieve the global targets for both developed and developing countries.10,11 Uninterrupted breastfeeding for at least the first 6 months of life is a matter of global importance for achieving adequate immunity against infection including diarrhea, the second leading cause of child death globally.12-14 Importantly, lack of breastfeeding in early infancy, especially at the neonatal period, is associated with a number of fatal diseases including diarrhea 15 and malnutrition. 16 To our knowledge, we did not find any published literature on the impact of lack of breastfeeding at the neonatal period in infants hospitalized for diarrhea. In this study, we evaluated the consequences of lack of breastfeeding at the neonatal period on infants hospitalized for diarrhea.
Materials and Methods
Study Site
The study was conducted in the Dhaka Hospital of icddr,b, established in 1962 in Dhaka city. The hospital provides care and treatment to people with diarrheal illnesses mostly from urban and peri-urban areas. More than 140 000 diarrheal patients receive treatment each year. The Diarrheal Disease Surveillance System (DDSS) has been operating since 1979, 17 which systematically sampled 2% of all patients since 1996. This system collects information on the clinical, epidemiological, and demographic characteristics; feeding practices, particularly of infants and young children irrespective of age, sex, and disease severity or socioeconomic status; and also collects microbiological data such as stool culture to see the etiology such as Vibrio cholerae, shigella, salmonella, Campylobacter, Escherichia coli, and ELISA (enzyme-linked immunosorbent assay) for Rotavirus by administering a structured questionnaire. A trained research assistant interviews either the patient himself/herself or the caregiver, in case of young children, following the questionnaire (details provided elsewhere 17 ).
Study Design
We gathered information prospectively from the electronic database of DDSS of the Dhaka Hospital of icddr,b. In this unmatched case-control design, infants of either sex, aged
Measurements
Case Report Forms (CRFs) were developed for the collection of data from the participants. Sociodemographic information (age, sex, monthly income and education of parents/care givers, residence status, etc), breastfeeding history at the neonatal period, vaccination status as per ongoing Expanded Programme on Immunization schedule in Bangladesh, and nutritional status, such as severe wasting (z score for weight for length/height <−3 of median of the WHO [World Health Organization] growth standard) were collected. Information regarding complicated diarrhea (defined as patients having diarrhea with complications such as electrolytes imbalance [most commonly hypernatremia and hypokalemia] or any other comorbidities like pneumonia, malnutrition, sepsis, and required admission to longer stay ward or intensive care unit of the Dhaka Hospital of icddr,b) and also medications and rehydration therapy needed for diarrhea along with current clinical history such as type of diarrhea, nature of stool, vomiting, and so on, were obtained from the respondents. Clinical conditions such as status of dehydration (no sign/some/severe) and abnormal mental status (restless/lethargic/drowsy/comatose) were assessed by the attending physicians and entered into the CRF. Information in the CRF was authenticated through quality control by repetition of interview and data check by reviewing all data collection tools on a daily basis by a supervisor, by consistency and frequency check during/after data entry on a daily basis, logical and range checks during/after data entry on a daily basis, and interim analysis on a weekly basis.
Data Analysis
All data were entered into SPSS for Windows (version 15.0; SPSS Inc, Chicago, IL) and Epi-Info (version 6.0, USD Inc, Stone Mountain, GA). In qualitative variables, differences in proportion were compared by the χ2 test. Student’s t test was used to compare the means of normally distributed quantitative data, and Mann-Whitney test was used for comparison of data that were not normally distributed. A probability of less than .05 was considered statistically significant. Strength of association was determined by calculating the odds ratio and their 95% confidence intervals. In the univariate model (2/2 table), characteristics that were analyzed include age and sex of children, literacy and residence status of parents, dehydration status, fever, abdominal pain, fast breathing, severe wasting, abnormal mental status, invasive diarrhea, and also presence of cholera and shigella in stool. Finally, logistic regression analysis was performed to identify characteristics that were independently associated with the infants who had non-breastfeeding or cessation of breastfeeding at the neonatal age after adjusting for potential confounders. All categorical variables that were significantly associated with the infants who were non-breastfed or had cessation of breastfeeding at the neonatal age in univariate analyses were included in the model as independent variables, whereas the infants who were non-breastfed or had cessation of breastfeeding at the neonatal age acted were included as the dependent variable. The regression model was checked for multicollinearity.
Ethical Approval and Informed Consent
DDSS (Ref No.: 92-011) has been approved by the research review committee and the ethical review committee, collectively called institutional review board of icddr,b. At the time of enrollment, the caregivers or the guardians used to provide verbal consent on behalf of the patients for their information to be stored in the hospital database and used for conducting researches. This verbal consent was renowned by keeping a check mark in the questionnaire, which was again given away to the patient or the caregivers. Parents or guardians were guaranteed about the nondisclosure of information obtained from them, and they were also well-versed about the use of data for analysis and using the results for improving patient care activities as well as publication without disclosing the name or identity of their patients. The ethical review committee was pleased with the controlled participation, safeguarding of the civil liberties of the participants, and confidential handling of individual information by the hospital clinicians and provided consent.
Results
A total of 13 411 patients were enrolled into the DDSS from 2009 to 2013 who were admitted in the Dhaka Hospital of icddr,b. Of them, 3989 were infants (<12 months of age) having diarrhea. Among them, 876 met the inclusion criteria of the study. There were 464 cases and 412 controls. Median age of the patients among cases was 6 months and that of controls 7.9 months, and the difference was statistically significant (Table 1). In univariate analysis, the cases more often presented with illiterate mother, complicated and dehydrating diarrhea, severe wasting, and abnormal mental status compared with the controls (Table 1). Other variables in Table 1 were comparable among the groups. In the logistic regression analysis, after adjusting for potential confounders, it was found that the infants who were non-breastfed or had cessation of breastfeeding at the neonatal age had an independent association with dehydrating diarrhea (Table 2).
Admission Characteristics of Infants With Diarrhea With and Without Breastfeeding at the Neonatal Period a .
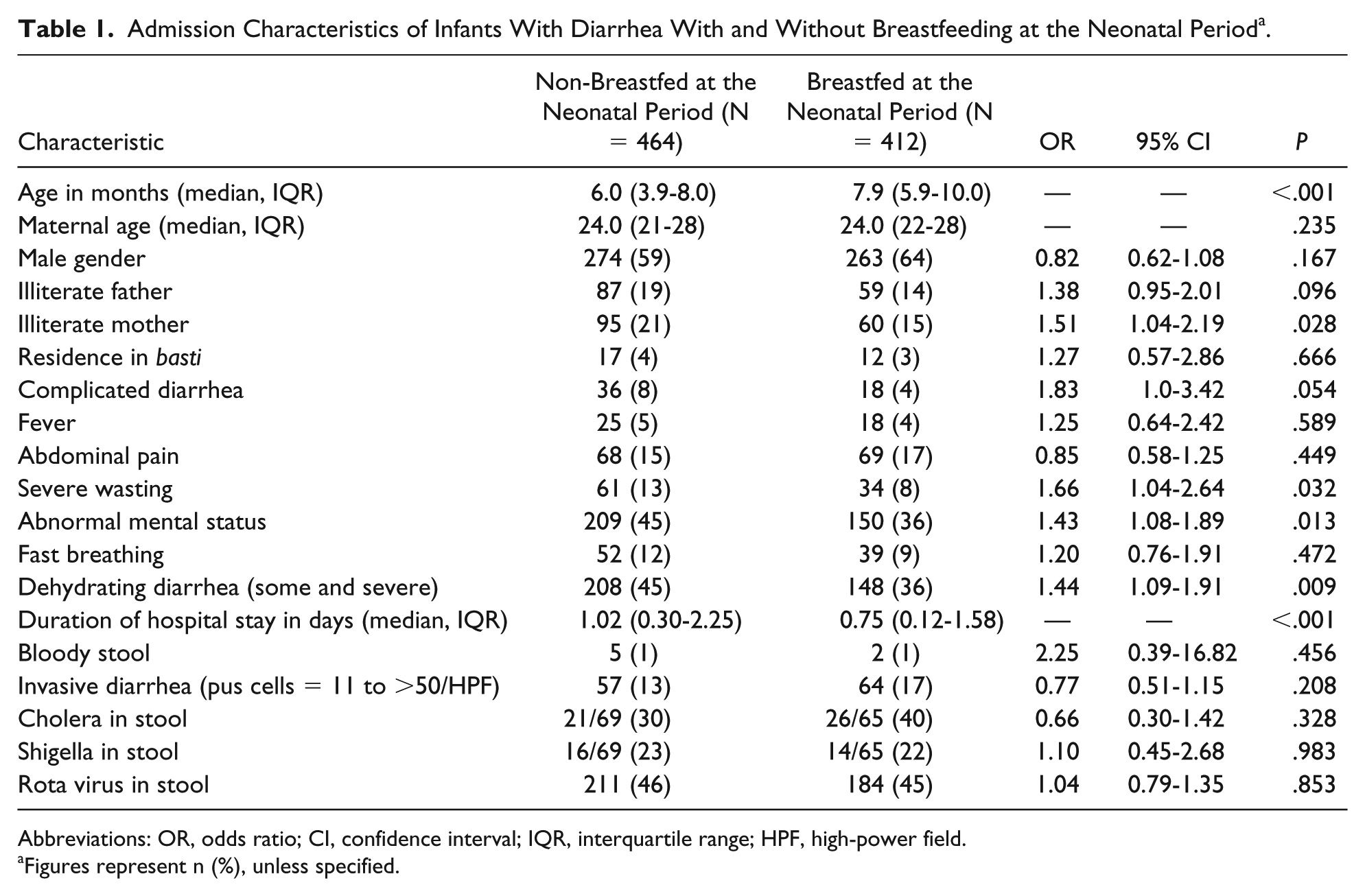
Abbreviations: OR, odds ratio; CI, confidence interval; IQR, interquartile range; HPF, high-power field.
Figures represent n (%), unless specified.
Logistic Regression to Explore the Independent Association of Lack of Neonatal Breastfeeding in Infants With Diarrhea.

Abbreviations: OR, odds ratio; CI, confidence interval.
Discussion
This is the pioneer study that evaluated the impact of lack of neonatal breastfeeding in infants who were hospitalized for diarrhea. The main observation of the study is the independent association of dehydrating diarrhea with infants who were non-breastfed or had cessation of breastfeeding in their neonatal age. Non-breastfed infants usually suffer from rota viral as well as Campylobacter, shigella, and Vibrio cholerae induced diarrhea, which are the most important etiologies of dehydrating diarrhea in infants, 18 and they are more likely to develop dehydrating diarrhea than exclusively breastfed infants.19,20 Although the observation is quite understandable, it essentially further underscores the importance of promotion of breastfeeding, which is still underachieved despite continued global effort.
Another important observation of this study was the association of lack of maternal education and non-breastfeeding in the neonatal period. Although the finding did not remain significant after adjusting with potential confounders, we found a number of studies that evaluated the positive impact of maternal education on initiation and duration of breastfeeding,21-23 which indirectly supports association of lack of maternal education and non-breastfeeding in the neonatal period. Moreover, some studies observed the association of less breastfeeding tendency 24 and negative conception regarding breastfeeding with less educated mothers. 25
The observation of association of complicated diarrhea with infants having non-breastfeeding or cessation of breastfeeding at the neonatal period in univariate analysis was quite understandable. These children were deprived of immunological substances of breast milk necessary for boosting up their immunity against infectious diseases like diarrhea along with complications such as malnutrition or other infectious comorbidities. This observation also became insignificant after logistic regression analysis; however, a number of previous studies found association of lack of breastfeeding with comorbidities of diarrhea with other infectious diseases.26,27
Another key observation of our study is the association of severe wasting with lack of or cessation of breastfeeding in infants in univariate analysis, which is also quite understandable. Anorexia in infants with diarrhea may reduce energy intake by 5% to 40% 28 ; however, breastfeeding usually remains incessant and intake may even increase during diarrhea. As a result, lack of breastfeeding during diarrhea further affects nutrient and energy intake.28,29 However, this observation also became insignificant after adjusting for potential confounders. Nevertheless, the association of severe acute malnutrition with the cessation of breastfeeding in early infancy has been reported earlier. 16
Another observation is the association of abnormal mental status in infants with non-breastfeeding or lack of breastfeeding in their neonatal age in univariate analysis, but lost its significance after logistic regression analysis. We do not have any ready explanation for this observation, and to our knowledge, no reported association of lack of breastfeeding with abnormal mental status was found.
The main limitation of the study is that observations are based on infants who attended the hospital and thus our data may not represent the general population. However, systematic sampling of patients including infants and large data set is the strength of our analyses. Moreover, despite variations, some differences were not statistically significant possibly due to lack of power with smaller sample size.
Conclusion
The results of our data suggest that diarrheal infants who were not breastfed at the neonatal age were at higher risk of developing some or severe dehydration compared with those who continued breastfeeding since birth (if age <6 months) or at least up to 6 months of age (if age >6 months). The observation essentially reemphasizes the critical need for the relentless promotion of breastfeeding for at least up to 6 months of age in order to prevent ramification of diarrheal illnesses.
Footnotes
Author Contributions
ASMSBS, TA, SK, KATMEH, KMS, ASGF, MMR, MMI, and MJC conceived and designed the study; ASMSBS collected, merged, and cleaned the data; ASMSBS, TA, SK, KATMEH, KMS, ASGF, MMR, MMI, and MJC analyzed and interpreted the data; ASMSBS, MMI and MJC gave technical support and conceptual advice; ASMSBS wrote the first draft of the manuscript and all the authors reviewed the manuscript; MJC finally approved the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Diarrheal Disease Surveillance System in the Dhaka Hospital of icddr,b was funded by icddr,b and the Government of the People’s Republic of Bangladesh through its IHP under HNPSP. icddr,b acknowledges with gratitude the commitment of the Government of the People’s Republic of Bangladesh to its research efforts. icddr,b also gratefully acknowledges the following donors who provide unrestricted support to the Centre’s research efforts: Government of the People’s Republic of Bangladesh; the Department of Foreign Affairs, Trade and Development (DFATD), Canada; Swedish International Development Cooperation Agency (Sida); and the Department for International Development (UK Aid).