
Abstract
The relationship between maternal symptoms and problematic infant feeding in the context of tongue-tie is unknown. In a sample of infants with tongue-tie undergoing frenotomy and their mothers, the aims of this study were to: (1) describe changes in maternal symptoms pre- and post-frenotomy, and (2) evaluate the relationships between maternal symptoms and symptoms of problematic feeding pre- and post-frenotomy. Mother-infant dyads were recruited from 1 pediatric dental office between July and November 2020. The sample included 102 mother-infant dyads; 84 completed the follow-up survey. Maternal symptoms of painful and difficult latch, creased/cracked nipples, bleeding, or abraded nipples, chewing of the nipple, and feelings of depression were significantly less common after tongue-tie revision. Poor latch onto the breast was associated with feeding difficulties at both time points. Frenotomy resulted in a decrease of symptoms in breastfeeding mothers. Maternal symptoms and feeding problems persisting post-frenotomy warrant further evaluation.
Ankyloglossia, also known as tongue-tie, occurs in approximately 8% of infants. 1 Mills et al 2 recognize that the wide degree of variation in morphology limits our ability to determine a definitive classification for the diagnosis of abnormal frenulum anatomy. The lingual frenulum is a complex structure formed by a midline fold that has a role in both providing stabilization of the tongue as well as allowing movement in multiple directions. 2 Tongue-tie occurs when this midline fold forms abnormally, resulting in a tight connection between the tongue and base of the mouth that restricts tongue motion and/or function.2,3 During breastfeeding, this restriction affects the ability of the tongue to produce the movement necessary to transfer milk from the breast to the mouth and into the posterior pharynx 4 and prevents effective latch onto the breast. 5 When latch is impaired, maternal nipple pain, decreased milk transfer, and infant feeding difficulties may ensue. 6
There are significant limitations to the current literature that restrict our understanding of who benefits most from frenotomy, and in what ways the breastfeeding mother and infant may benefit from frenotomy with regards to feeding. 7 While researchers have explored maternal symptoms, such as nipple pain8-13 more evidence is needed to examine the effects of frenotomy on the mother-infant dyad. 7 Current studies evaluating frenotomy for the treatment of tongue-tie lack the methodological rigor necessary to promote a change in screening, assessment, and treatment guidelines. 14 A recent study reported an 866% increase in frenotomy rates from 1997 to 2012. 15 In a sample of infants less than 7 months old with tongue-tie undergoing frenotomy and their mothers, the purpose of this study was to: (1) explore changes in maternal symptoms pre- and post-frenotomy, and (2) evaluate the relationships between maternal symptoms and symptoms of problematic feeding pre- and post-frenotomy.
Methods
Design
This was a prospective, sequential, 1-group pre/post intervention study design. We compared infant feeding and maternal symptoms immediately before and 2 weeks after frenotomy.
Setting
This study took place at 1 pediatric dentist office in Albany, New York. There is 1 pediatric dentist at the location where this research was conducted, who performs all the assessments using the Kotlow 16 criteria and completes all the frenotomy procedures, allowing for consistency across infants. The pediatric dentist recommended follow-up with a lactation support provider after the frenotomy procedure. Participation in this research study did not alter the course of clinical care provided to infants.
Sample
To be included in this study, the infant had to be less than 7 months old, diagnosed with tongue-tie, undergoing frenotomy. Mothers needed to be proficient in English to complete the surveys. Exclusion criteria were prematurity (born earlier than 37 weeks’ gestation); anomalies of the head, face, or neck that may impair feeding; or the presence of comorbid conditions associated with feeding difficulty. Convenience sampling was used and all eligible mother-infant dyads during the study period were invited to participate.
G*Power 3.1.9.4 (G*Power, Germany) was used to conduct an a priori power analysis. Independent t-test was used to calculate the required sample to achieve 90% power, given alpha of .05 (2-tail), using a standardized effect size method (Cohen’s d) to detect a medium change in differences between means (0.5). Our final sample of 84 mother-baby dyads was adequately powered for all statistical analyses.
Measurement
Therapy to assist with feeding was coded into 2 options, yes or no. If participants endorsed receiving therapy, 12 possible options were provided to choose from: feeding specialist; lactation support provider; orofacial myofunctional specialist; speech therapist; pediatrician; occupational therapist; physical therapist; dietician/nutritionist; gastroenterologist; chiropractor; ear, nose, and throat (ENT) specialist; craniosacral therapist. Kotlow’s 16 diagnostic criteria was used to classify tongue-tie. This tool measures the length of the freely mobile tongue in millimeters, with tongue-tie graded from least restrictive (Class 1) to most restrictive (Class IV).
Maternal symptoms
Mothers indicated if they experienced any of the following symptoms: creased, cracked or blanching of their nipples; painful latch onto the breast; gumming or chewing of their nipples; infant unable to achieve a tight latch; poor or incomplete breast drainage; infected or abraded nipples; plugged ducts; mastitis; nipple thrush; over or under supply; or feelings of depression. A total sum of all maternal symptoms was calculated both pre- and post-frenotomy.
Infant feeding
Symptoms of problematic feeding were measured using the Neonatal Eating Assessment Tool (NeoEAT), a parent-report measure of feeding intended for use with infants under 7 months old. There are 3 versions of the NeoEAT 17 : the NeoEAT—Breastfeeding, for infants who have exclusively breastfed in the past week;18,19 the NeoEAT—Bottle-feeding, for infants who have exclusively bottle-fed in the past week;20,21 and the NeoEAT – Mixed Feeding, for infants who have both breastfed and bottle-fed in the past week.22,23 Each question on the NeoEAT is rated on a 5-point Likert scale, with answer options ranging from “never” to “always.” Scores are summed to create a total score as well as subscale scores, with higher scores indicating more symptoms of problematic feeding. Descriptors for each subscale are summarized in the Supplementary File. All 3 versions of the NeoEAT have been found to have adequate psychometric properties, including content and construct validity, internal consistency reliability, and test-retest reliability. 24
For the sample included in this study, internal consistency reliability of the NeoEAT was excellent for all 3 versions pre- and post-frenotomy. Cronbach’s alpha for the NeoEAT—Breastfeeding scale was α = .94 pre-frenotomy and α = .90 post-frenotomy. Reliability for the NeoEAT—Bottle-feeding scale was α = .98 pre-frenotomy and α = .94 post-frenotomy. Reliability of the NeoEAT—Mixed Feeding was α = .96 and α = .94 for pre- and post-frenotomy, respectively.
Ethical Approval and Informed Consent
This study was approved by the Institutional Review Board of Boston College (#20.267.01). All parents provided informed consent for participation for both themselves and their infants prior to data collection.
Data Collection
The sample was recruited between July and November 2020. Medical record data was provided by the dental office staff to the principal investigator. Study data were collected and managed using REDCap electronic data capture tools.25,26 Tongue-tie classification and maternal symptoms pre-frenotomy were extracted from the medical record by the first author. Baseline maternal information collected included maternal age, race/ethnicity, marital status, pregnancy and birth history, and prior experience with breastfeeding. Baseline infant data included gestational age at birth, current age at the time of frenotomy, sex, current feeding mode and medical status. Two weeks post-frenotomy, participants received an electronic survey via email which asked about changes in infant medical history and maternal symptoms since treatment of their infant’s tongue-tie. At each time point, participants completed the NeoEAT version (Breastfeeding, Bottle-feeding, or Mixed Feeding) that reflected the mode(s) of feeding used the prior week.
Data Analysis
All data were analyzed in SPSS v.25. Descriptive statistics were used to characterize the study population. Aim 1 included participants who reported breastfeeding in any capacity at time 1 or time 2. For this aim, McNemar’s test was used to compare proportions of maternal symptoms pre- and post-frenotomy for each individual symptom. We then used Poisson regression to determine if there were significant changes in the number of symptoms pre- to post-frenotomy.
Aim 2 included participants that were exclusively breastfeeding at either time point. For this aim, the relationship between maternal and infant symptoms were compared. Mean scores for NeoEAT total and subscale scores were calculated for participants who reported the same mode of feeding at both time points and paired t-tests were performed to compare mean scores for the NeoEAT total and subscales. Point biserial correlations were performed for each maternal symptom and NeoEAT total and subscale scores to examine which maternal and infant symptoms were related at each time point. The strength of the relationship between maternal symptoms and NeoEAT scores was evaluated using generalized linear modeling, excluding variables that were highly correlated with each other (P < .05). Next, reliability analyses of each NeoEAT scale at both time points were evaluated using Cronbach’s alpha. Statistical significance was set at α = .05 (2-tailed) for all statistical tests.
Results
A total of 102 participants completed the pre-frenotomy survey and 84 completed the post-frenotomy survey for a study completion rate of 83.3%. There were no significant differences between respondents and non-respondents on pre-assessment variables that could explain results of the follow-up survey. Participants were from 5 northeast states, with parent age ranging from 19 to 45 years (M = 31.6, SD = 5.2). Infant age ranged from 3 days to 29 weeks, 3 days (M = 6 weeks, SD = 6.23). Participants were primarily referred to the pediatric dentist either by a lactation support provider (n = 37) or a pediatric primary care provider (n = 23). In the month prior to frenotomy, 8 of the dyads received therapy to help with feeding via lactation support providers (n = 4) or chiropractic care (n = 4). Tables 1 and 2 describe the sample characteristics.
Demographics of Participants (N = 102).

Demographics of Participants’ Infants (N = 102).
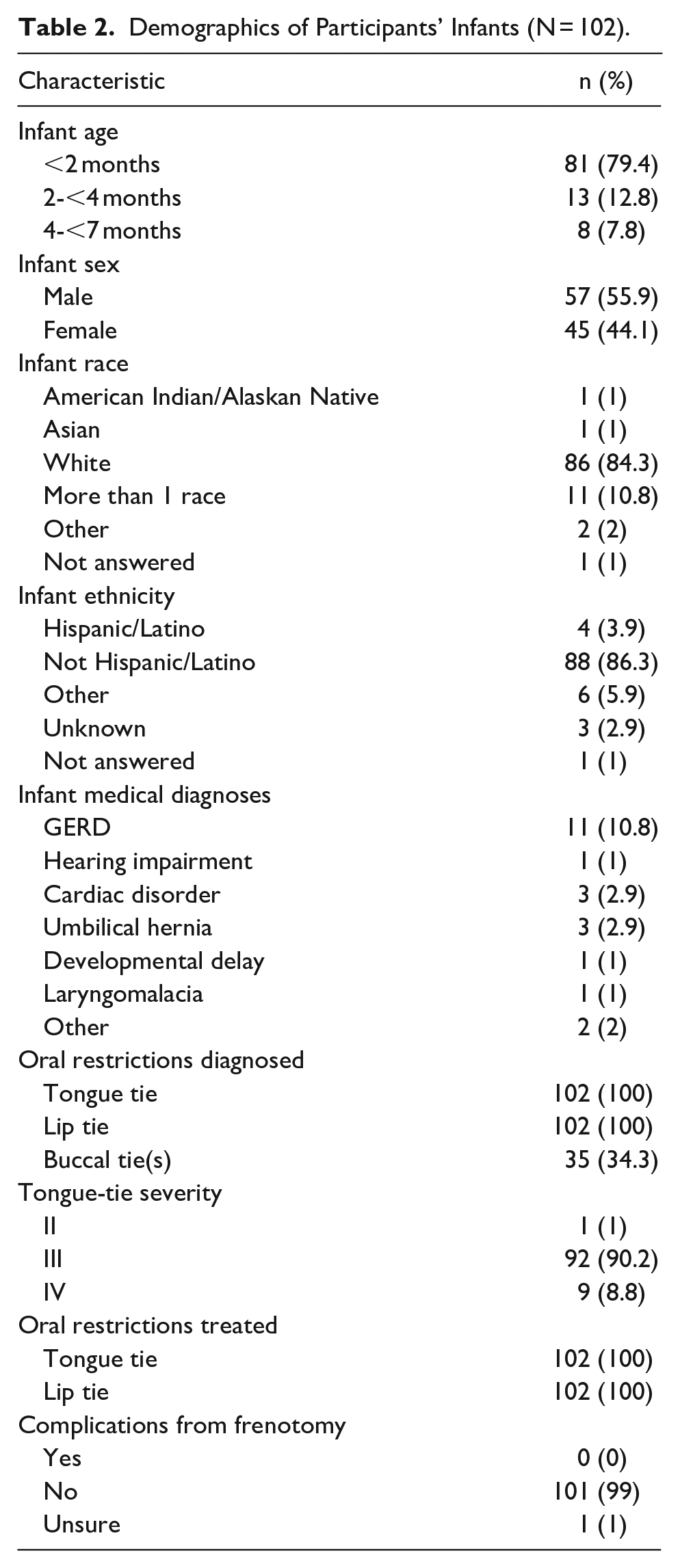
Most infants (n = 101) presented with a Kotlow Class III or IV tongue-tie, indicating “severe” restriction. All the infants were also diagnosed and treated for lip tie. Approximately one-third (35%) of infants were diagnosed with buccal ties, although none of these were corrected. Within 2 weeks of the procedure, 23 (27.4%) dyads received therapy to assist with feeding, including lactation support (n = 12), chiropractic care (n = 10), and craniosacral therapy (n = 4). From pre-frenotomy to post-frenotomy, 24 participants (28.6%) changed the method of feeding their infant based on the NeoEAT scale used at each time point. Of this subsample, 17 (70.8%) increased breastfeeding. Fourteen of the 24 mothers (58.3%) switched from mixed breast/bottle feeding to exclusive breastfeeding, 2 (8.3%) changed from exclusive bottle to exclusive breastfeeding, and 1 (4.2%) changed from exclusive bottle to mixed breastfeeding and bottle-feeding. Seven (29.2%) of the participants who reported a change in feeding method changed from exclusive breastfeeding to mixed feeding.
Aim 1: Maternal Symptoms
Participants who were breastfeeding in any capacity (n = 85, 83.3%) reported up to 8 concurrent symptoms pre-frenotomy, with the most common symptoms being painful latching (n = 61), difficulty achieving successful latch (n = 50), and gumming/chewing of the nipple while eating (n = 49). All reported maternal symptoms decreased from pre- to post-frenotomy. Post-frenotomy, 75 (89.3%) participants (n = 84) were breastfeeding. The most common symptoms were painful latch (n = 21), gumming/chewing of the nipple (n = 17), and incomplete breast drainage (n = 14).
Seven of the 15 symptoms assessed had significantly greater likelihood of occurring prior to frenotomy. Comparison of symptoms at both time points are presented in Table 3, with an overall percentage of the sample reporting improvement. Using Poisson loglinear modeling, the likelihood ratio chi-square test indicated that the full model, which included total maternal symptom count, was a significant improvement in fit over a null (no predictor) model (P < .001). The number of maternal symptoms was significantly different pre- to post-frenotomy (β = .88, SE = .106, P < .001). The predicted number of maternal symptoms was .88 greater pre-frenotomy. The incidence rate ratio (ExpB) indicates that for every one-unit decrease on the predictor (time), the incidence rate of maternal symptoms increased by a factor of 2.41. In other words, the incidence rate of maternal symptoms was 141% higher before frenotomy.
Comparison of Maternal Symptoms using McNemar’s Test.

Binomial distribution used.
Aim 2: Relationships Between Maternal Symptoms and Infant Feeding
Participant report demonstrated decreased infant symptoms post-frenotomy in nearly all symptoms. Despite an increase in utilization of feeding support following tongue-tie revision, one-third of participants continued to endorse difficulty with latching onto the breast. There were 35 participants (N = 102) (34.2%) exclusively breastfeeding pre-frenotomy and 39 (46.4%) exclusively breastfeeding post-frenotomy (n = 84). Tables 4 and 5 depict the point biserial correlations between maternal and infant symptoms pre- and post-frenotomy, respectively.
Correlation of Maternal Symptoms and NeoEAT Scores Pre-Frenotomy in Exclusively Breastfeeding Mother-Infant dyads (n = 35).

Correlation of Maternal Symptoms and NeoEAT Scores Post-Frenotomy in Exclusively Breastfeeding Mother-Infant Dyads (n = 39).

Creased, cracked, or blanched nipples, bleeding nipples, and gumming/chewing of the nipple were excluded for multicollinearity with painful latching onto the breast. In the regression analyses, oversupply was significantly associated with increased total NeoEAT score (28.9-point increase, t = 2.50, P = .02), Energy and Physiologic Stability (7.4 points higher, t = 2.77, P = .01), Feeding Efficiency and Sensory Responsiveness (4.5 points higher, t = 2.66, P = .01), Oro-Pharyngo-Esophageal (7.5-point increase, t = 2.41, P = .02), and Compelling Symptom (2.5 points higher, t = 2.45, P = .02) subscale scores, indicating more severe symptoms of problematic feeding before tongue-tie revision. Feeding Efficiency and Sensory Responsiveness subscale score increased by 4.9 points (t = 2.73, P = .010) when participants reported poor latch onto the breast. Under supply of breastmilk corresponded with a 16.8-point increase in Energy and Physiologic Stability subscale scores (t = 2.1, P = .04).
Following frenotomy, the total NeoEAT score was 35.4 points higher (t = 2.39, P = .03) in participants reporting painful latching, 37.1 points higher when poor latch was present (t = 3.38, P = .002), and 24.5 points higher (t = 2.42, P = .03) in participants reporting incomplete breast drainage. Infant Regulation subscale scores were 15.1 points higher in participants with painful latch (t = 4.44, P < .001). Report of poor latch or incomplete breast drainage were associated with higher Energy and Physiologic Stability scores (7.5 and 7.9 points higher, respectively, t = 2.78 and 3.52, P = .008 and .002). Poor latch was also associated with Gastrointestinal Function (β = 4.91, t = 2.69, P = .01) and Feeding Efficiency and Sensory Responsiveness subscale scores (β = 6.62, t = 3.26, P = .002). Oro-Pharyngo-Esophageal scores were 6.2 points higher (t = 2.14, P = .04) when incomplete breast drainage was present. Compelling Symptoms of Problematic Feeding subscale scores were 2.4 points higher in infants when participants reported poor latch (t = 2.29, P = .03) and if participants were experiencing incomplete breast drainage (t = 2.64, P = .02). Table 6 provides mean scores for NeoEAT total and subscales for participants using the same mode of feeding at each time point.
Differences in NeoEAT Total and Subscale Scores.
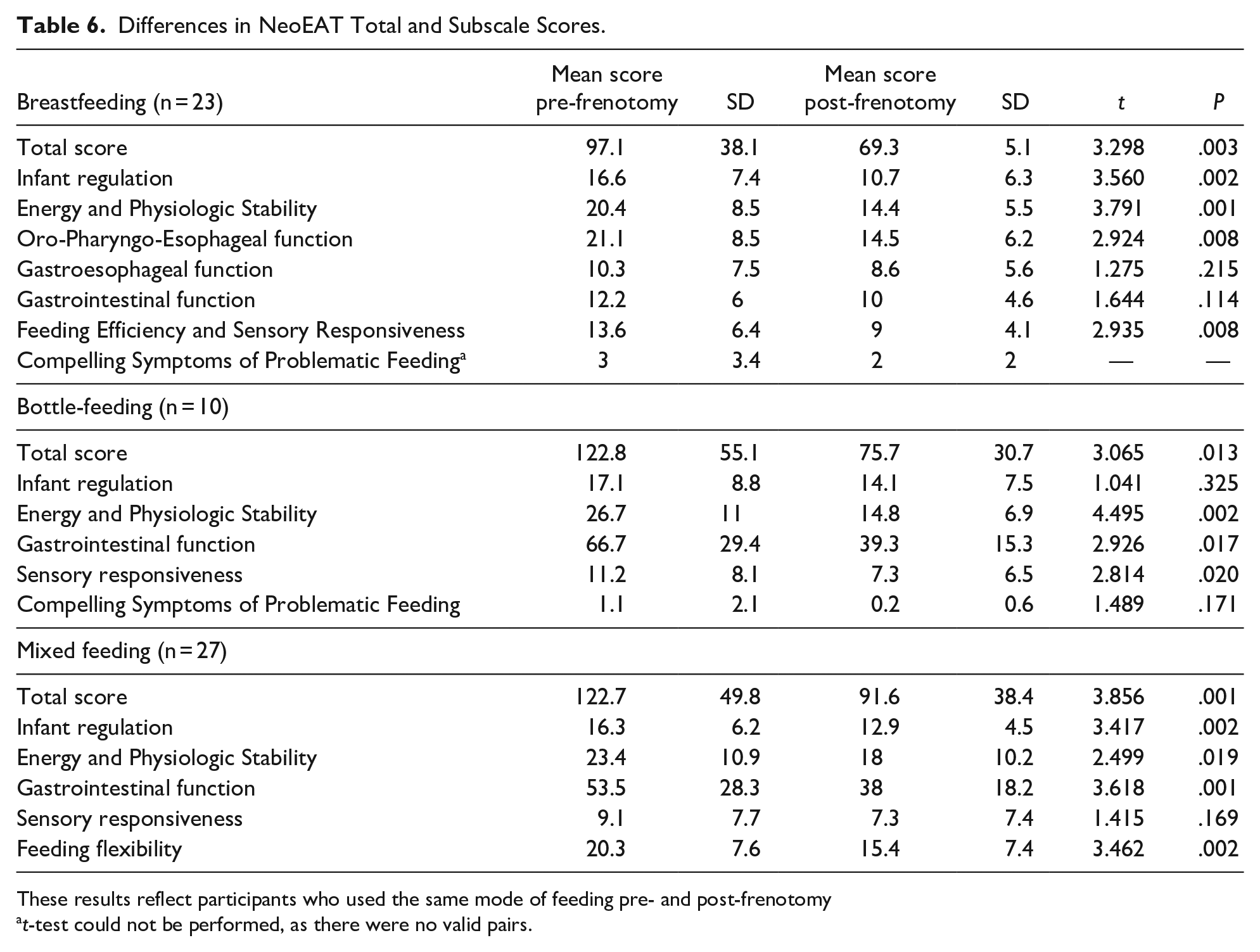
These results reflect participants who used the same mode of feeding pre- and post-frenotomy
t-test could not be performed, as there were no valid pairs.
Discussion
This is the first known study where researchers explore the relationship between infant feeding and maternal symptoms in breastfeeding mothers in the context of frenotomy for tongue- tie. It is important to acknowledge that in this sample of infants with severe tongue tie, there was a transition to exclusive breastfeeding after frenotomy in mothers who were using bottle-feeding or a mixed approach to feeding before tongue-tie revision. There was also an increase in breastfeeding in those who were bottle-feeding prior to frenotomy. Like other studies, we found that maternal symptoms significantly decreased post-frenotomy. The most common symptoms were consistent with those described in previously published research. 7 For mothers reporting these symptoms, evaluation of a breastfeeding session to examine latch, position, and infant ability to sustain a breastfeeding session will assist providers in identifying differential diagnoses such as tongue-tie, or breastfeeding mechanics that can be adjusted to reduce maternal discomfort. With the significant decrease in maternal symptoms post-frenotomy without other intervention, tongue-tie should be considered as a potential cause of painful or difficult latching or infant chewing on the nipple during feeding. To our knowledge, there are no published studies where researchers have examined depressive symptoms in the setting of tongue-tie; this was an important finding that warrants further investigation.
The association between maternal symptoms and infant feeding challenges helps explain how maternal symptoms and infant feeding symptoms are intertwined in the breastfeeding mother-infant dyad. Replication of this research on a larger, multi-site sample will help to explain the strength of the relationship between maternal and infant symptoms in the setting of tongue-tie. Conceptually, it is reasonable to expect that actual or perceived oversupply of breastmilk would be related to several of the NeoEAT subscales, as they relate to how an infant responds to breastfeeding. An infant with tongue-tie and poor tongue mobility may have difficulty effectively removing milk from the breast, leaving the breastfeeding mother with a perception of oversupply. At the same time, poor tongue mobility may affect the infant’s swallow and an oversupply of milk may cause the infant to take frequent breaks while eating, to be unable to handle how fast milk comes out of the breast, or to drool breastmilk from the sides of the mouth. 28 Choking on breastmilk is another possible sign of oversupply, 27 a symptom assessed on the Oro-Pharyngo-Esophageal Function subscale. Additionally, impaired Sensory Responsiveness of the infant can lead to gagging during eating that may be related to nipple position in the mouth, or a hypersensitive gag reflex secondary to a narrow palate. 28 Poor tongue elevation caused by tongue-tie may impair the ability of the palate to widen. 29
While many mothers reported improvement in symptoms, some persisted following frenotomy. In those that reported poor or painful latch onto the breast or incomplete breast drainage after frenotomy, infants continued to have challenges with feeding. This may suggest that the infant needs additional time to re-learn proper breastfeeding or that other factors are present beyond tongue-tie causing these persistent maternal symptoms. Evaluating maternal symptoms and infant feeding longitudinally, in conjunction with feeding support mothers receive would provide additional information on why and how tongue-tie revision or other factors may reduce these symptoms over time. In the research published to date, the outcomes of interest have been either the mother or the infant but lack dyadic evaluation necessary for the feeding pair. A better understanding of how the dyad is affected by severe tongue-tie gives insight to providers of symptoms the mother or the infant may have if severe tongue-tie is present and how the combination of these symptoms may result in early breastfeeding cessation or continued feeding challenges.
Limitations
The sample was homogenous, representing mainly white mother-baby pairs in the northeast region of the United States. As regional differences exist regarding tongue-tie diagnosis and dyadic care, 30 we do not know if the results would have been different if the study were conducted in another region of the nation. We do not have data to compare respondents to non-respondents and do not know if the follow-up survey results would have been significantly different in the 18 participants who did not complete the follow-up survey. We do not have information on how many mother-baby dyads presented to the office between July and November who did not have a diagnosis of tongue-tie, who declined treatment of the anomaly, or who declined to participate in this study.
With most of the sample diagnosed with Class III tongue-tie, it is not possible to generalize how other degrees of tongue-tie restriction might alter maternal symptoms associated with the condition. It is also important to consider that tongue function, in addition to tongue appearance is a critical assessment before making the decision to treat. All infants who were treated and included in this study were also diagnosed and treated for lip tie, so we cannot determine if it was the tongue-tie, lip-tie, or a combination of both oral restrictions that contributed most to the improvements in maternal symptoms post-frenotomy. The treatment of lip-tie is controversial; we do not have data to support the revision of lip-ties, nor do we know how the restricted maxillary frenulum affects feeding.31,32 Of note, all the infants being diagnosed and treated for both tongue and lip-tie in this study contradicts prior work where researchers did not find an association between these 2 anomalies occurring concurrently. 33 Future research should be directed at both a larger and more diverse sample, with a variety of tongue-tie classifications and functional assessments, and specific evaluation between infants with and without concomitant lip-tie. It is important to note that the Kotlow criteria has not been assessed for reliability or validity. Longitudinal evaluation of maternal and infant symptoms that includes a control group of infants without tongue-tie would strengthen our understanding of how this oral anomaly influences feeding.
Inherent to pre/post study designs, there are threats to internal validity due to the absence of a control group. Specifically, history, maturation, testing, and spontaneous remission are potential threats to the study design. 34 By the two-week follow-up survey, other factors may have led to improvements in maternal or infant symptoms. Infant maturation and experience with feeding may have decreased problematic feeding scores simply based on the additional time the infant was learning to properly feed. The participants were familiar with the NeoEAT survey as the instrument was repeated in both surveys, which may have altered responses. We cannot determine if a “wait and see” approach would have resulted in spontaneous improvement in maternal or infant symptoms and caution must be used regarding inferring causality in this pre/post design methodology. Despite these limitations, these findings make an important contribution to our understanding of the effect of frenotomy on the mother-infant dyad.
Conclusion
In infants with severe tongue-tie, the authors found that frenotomy significantly decreased maternal symptoms in breastfeeding mothers. Two-weeks after frenotomy, most of the sample increased breastfeeding. In breastfeeding mother-infant dyads, symptoms of problematic feeding and maternal symptoms are highly inter-related. Comprehensive evaluation of the breastfeeding mother-infant dyad needs to include assessment of both the mother and the infant, using valid and reliable measures whenever possible. Similarly, future research evaluating the efficacy of frenotomy in breastfeeding mother-infant dyads must acknowledge that the mother and baby are inextricably linked partners in feeding and must comprehensively evaluate the dyad. For infants and/or mothers with persistent symptoms 2 weeks after frenotomy, further evaluation and intervention is warranted.
Supplemental Material
sj-docx-1-gph-10.1177_2333794X211072835 – Supplemental material for Effect of Frenotomy on Maternal Breastfeeding Symptoms and the Relationship Between Maternal Symptoms and Problematic Infant Feeding
Supplemental material, sj-docx-1-gph-10.1177_2333794X211072835 for Effect of Frenotomy on Maternal Breastfeeding Symptoms and the Relationship Between Maternal Symptoms and Problematic Infant Feeding by Rebecca R. Hill, Karen S. Lyons, Susan Kelly-Weeder and Britt F. Pados in Global Pediatric Health
Footnotes
Acknowledgements
The authors wish to thank Dr. Larry Kotlow and his office staff for their support and assistance with participant recruitment. The authors also wish to thank the parents and infants for participating in this study.
Author Contributions
RRH: contributed to conception and design; contributed to acquisition, analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
KSL: contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SKW: contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
BFP: contributed to conception and design; contributed to acquisition, analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Seed grant provided by the MGH Institute of Health Professions School of Nursing.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.