
Abstract
Children and youth with special health care needs (CYSHCN) comprise a growing proportion of the pediatric population; the patient- and family-centered medical home provides a comprehensive model for caring for these patients. Given the limited literature available as well as extreme patient vulnerability, we sought to understand the experience of Latino parents in caring for their CYSHCN within our patient-centered medical home in an urban neighborhood in North Philadelphia. A convenience sample of 14 mothers or grandmothers of CYSHCN participated in semistructured interviews, which were analyzed using a thematic, constant comparative approach to identify common themes. Themes identified included “Waiting,” “Communication/Trust,” “All-Consuming Requirements of Care/Sacrifice,” and “Fate/Faith/Blessings.” These themes corresponded with identified goals of the patient-centered medical home. Our findings suggest that the principles of the patient-centered medical home can be applied in unique ways to caring for this unique patient population.
Keywords
Introduction
Children and youth with special health care needs (CYSHCN) comprise a rapidly growing proportion of the pediatric population. 1 First defined by McPherson et al in 1998, CYSHCN are those who “have or are at increased risk for a chronic physical, developmental, behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.” 2 This definition, based on increase need for services rather than on specific diagnoses or functional status, has been used by the National Survey of CYSHCN to estimate the prevalence of these children. 1 In their 2009-2010 survey, they estimated an overall prevalence of 15.1%, an increase from prior years. 1 Of this cohort, the percentage of Hispanic CYSHCN is 22.4% nationally and about 8.1% in the Commonwealth of Pennsylvania. 1 A subset of CYSHCN has recently been termed “children with medical complexity” and is defined as children with multiple chronic health conditions affecting multiple organ systems and resulting in extremely high health care utilization and a reliance on medical technology. 3 These children comprise about 1% of the pediatric population, but account for approximately one third of all pediatric health care spending. 4 Due to the improved survival rates of premature infants and advances in medical technology, it is believed that this number will continue to rise steadily with a concurrent rise in cost of caring for these patients, making CYSHCN in general, and children with medical complexity specifically, a patient population of particular interest. 5
Our Center for Children and Youth with Special Health Care Needs provides a unique model for caring for this medically fragile patient population. 6 Our Center is located within St. Christopher’s Hospital for Children, a free-standing children’s hospital in an urban neighborhood of Philadelphia. Most of the patients seen at St. Christopher’s Hospital for Children are living at or below the poverty line, with 26% of residents of the hospital’s zip code living below 50% of the poverty line. 7 In our Center, we see 2800 patients, 92% who represent minority race/ethnicity, of which 60% are Black/African American, and 28% identify as Latino. Many of our patients’ families (about 40% of the Latino-identified families) are primarily or exclusively Spanish speaking. Several studies suggest Latina mothers of children with intellectual as well as physical disabilities report a lack of support and satisfaction, as well as lower levels of parenting confidence and heightened levels of anxiety, even when adjusting for socioeconomic status.8,9
Given the particular vulnerability of our patient population based on their increased need for medical care, their socioeconomic status, and their racial and ethnic disparities, our Center functions as a primary care medical home for our patients and their families. The medical home is defined in the pediatric literature as an approach to providing primary care that is “accessible, continuous, comprehensive, family-centered, coordinated, compassionate, and culturally effective.” 10 The medical home is the standard of care for health care delivery but is not sufficient without care coordination, family-centered care, and culturally and linguistically effective care.11-13 Though literature exists describing differences in Latino beliefs with regard to health care, 14 achieving cultural competence mandates an ongoing process of inquiry and active listening. 15 In striving to provide a true medical home to all of our patients, we sought to understand the experience of our Latino families with Spanish as their preferred spoken language in navigating their child/youth’s journey through the health care system as there is a dearth of their perspective in the literature.
Objectives and Research Questions
This qualitative study was initiated to enhance understanding of the circumstances and unique needs of exclusively or primarily Spanish-speaking families in our CYSHCN patient population. The study involved a series of semistructured in-depth interviews of parents/caregivers, designed to explore 2 objectives:
Identify special issues associated with language and culture beyond the customary challenges of caring for a CYSHCN confronting Spanish-speaking parents/caregivers in our Center.
Explore the role of our Center in mitigating or exacerbating the unique barriers experienced by population of interest and foster addressing these barriers in the delivery of services.
Study Design and Methods
Respondents were chosen via a convenience sample from the practice registry and were contacted via phone or in person at a scheduled medical appointment. Selection criteria included families who were exclusively or primarily Spanish-speaking and who, in the assessment of the program staff, had sufficient experience with our Center (a minimum of 1 year as a patient) and would be willing to provide a thoughtful interview. Interviews were conducted in the patient’s home.
Four basic questions guided the interviews and served as part of the interview guide. The interviewer initially asked the respondent to “Tell me about your child.” The ensuing discussion followed with open-ended questions about experiences of language barriers in health care for the child, other obstacles in caring for the child, and suggestions for improvement of the Center’s services.
A total of 14 in-depth interviews were completed: 11 with mothers, 2 with grandmother primary caretakers, and 1 with a mother/grandmother dyad. The majority of interviewees were from Puerto Rico; 5 were from South America. Interviews ranged from 30 to 90 minutes, conducted and audiotaped entirely in Spanish by a certified Spanish-speaking interpreter. Participants were given a nominal gift card for their participation in the study. Interviews were translated, transcribed into English, back-translated into Spanish, and subsequently reviewed by 2 independent translators for accuracy.
A thematic, constant comparative approach to grounded theory was used to identify common themes among respondents, 16 with special attention given to issues of Latino culture and language. The analysis team included 3 physicians (the Center’s medical director—RT, a senior attending physician of the Center—FM, a third-year medical resident—NB, and the General Pediatrics Section Research Director trained in medical anthropology—BB). An iterative series of consensus sessions were held among team members after individual review of sets of transcripts. Themes were consolidated through a consensus process after all transcripts had been reviewed and discussed.
Ethical Approval and Informed Consent
This study was supported by an American Academy of Pediatrics Community Access to Child Health (CATCH) Grant. The study was approved by the Drexel University College of Medicine Institutional Review Board (Protocol Number 16110: “Building Centers for Philadelphia’s Children with Special Health Care Needs”).
Results
Response to the initial prompt, “Tell me about your child,” typically resulted in an expansive description of the first experience of the child’s condition and diagnosis, critical interactions with health care providers, the child’s current abilities and limitations, and the mother’s dedication to and love for the child. Our examination of the transcripts produced a rich set of major interconnected themes, which we categorized as “Waiting,” “Communication/Trust,” “All-Consuming Requirements of Care/Sacrifice,” and “Fate/Faith/Blessings.” These themes and corresponding subthemes are outlined in Figure 1. Throughout these interviews, the mothers’ and grandmothers’ unconditional love and relentless striving to maximize the comfort and experiences of their children was compelling.
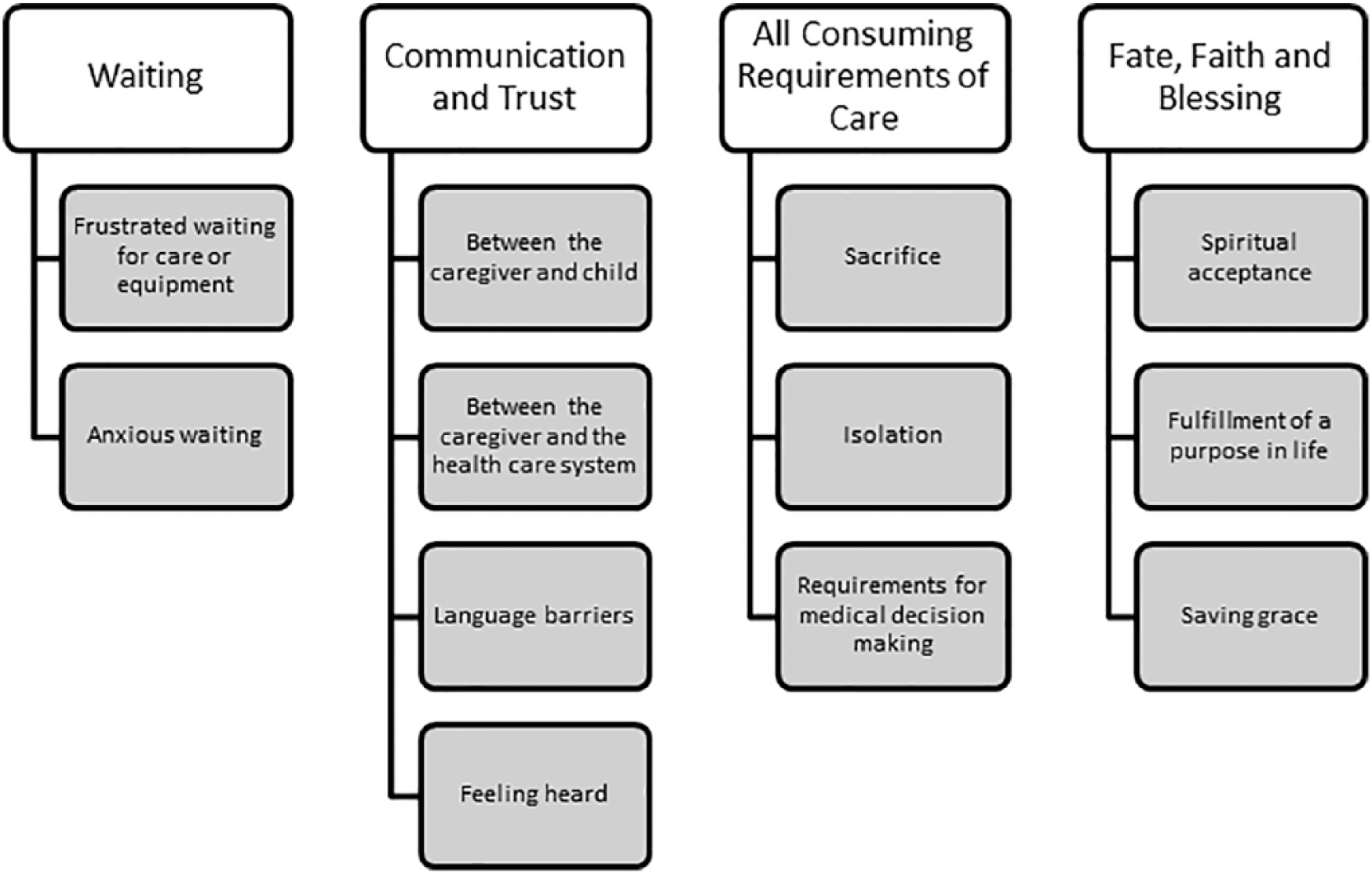
Themes and subthemes.
Waiting
We conceptualized one of the prominent themes, described by virtually all respondents, as “waiting,” in various contexts. Their daily lives as caretakers involved recurrent events of frustrated waiting, such as waiting in medical encounters in the emergency department or at scheduled appointments; waiting for transportation, which often required special vehicles; or waiting for necessary equipment required for the child’s mobility and comfort (customized wheelchairs, mobility aids, and specialized beds) and for service arrangements, especially related to housing and school. Obtaining the necessary services or equipment could require days, months, or even years.
Anxious waiting, waiting with a sense of impending suffering, related to diagnosis, prognosis, and the child’s life course, was an overriding feature of these caretakers’ lives. One mother said: He is 8 years old. When he was born, they told me that he would only live for 2 weeks.
Another mother expressed a pervasive feeling among respondents: I worry that one day one of these bruises can be her last. That is my biggest worry.
Communication and Trust
Three recurring communication issues were significant features of the interviews: communication between the caregiver and child, between the caregiver and the health care provider/team, and between the caregiver and the medical home team. Several respondents noted communication with the child, especially when nonverbal or of limited language capability, as a particular concern. In one mother’s words: It is not easy to see your child in the condition that he is in—he cannot tell you when he does not feel good or if he is in pain. All he can do is cry. . . . The biggest barrier is knowing how he is feeling. . . . I would like to understand him a little better.
More frequently the communication concern was with doctors specifically, especially subspecialists, and the medical system more generally. Much of this was related to basic language understanding and the delays and misunderstandings that could come from this. Several mothers noted a lack of translators or having to wait for a Spanish-speaking staff member to become available. This circumstance was typically presented as a routine difficulty that could be overcome, but could be problematic, as one mother explained: They never give me a translator. I understand, but I do not feel comfortable talking with a doctor. There can be a delicate subject, they may say something I don’t understand and I say “yes” and it’s inappropriate. I do not want to make things complicated.
A more serious issue detailed by a number of mothers was the experience of health providers not listening to their observations and concerns. This was not a matter of language, but rather one of respect. Mothers routinely indicated that they had spent the majority of their children’s lives caring for them and knew them better than anyone else. They were particularly distressed when their recommendations were ignored: I called [specialist’s] nurse. I said I needed a smaller catheter, because the 12 French is irritating the baby. He said “she is always complaining or she always needs something.” . . . Sometimes I think that the doctor doesn’t believe me with what [child] has or what she’s doing. Sometimes I feel that they don’t listen to what I am trying to say.
Another mother stated: I asked her neurologist to do her levels and the level came back as a level of 4. I told him that it was low, usually if it’s that low she’ll have a seizure. . . . Let’s check it maybe in the lab. He tried to tell me that she was not going to have a seizure, but I told him that usually she was at a level of 10 to 20. She did have a seizure; these are things that can be avoided. I told them that if they had listened to me, then my daughter would be home with me today. Now she is here (hospital).
In contrast, mothers were uniform in their praise of the concern, feeling of partnership and mutual respect they had in their association with the Center for Children and Youth with Special Health Care Needs, the team, and its medical home model. Several mothers made observations: I cannot complain, with the entire physician/staff, everyone has been very good to us. It’s like having a friend there. The physician sees me, we talk. The social worker from the hospital treats us well . . . they have always helped us. They have offered telephone numbers and pager, and we’re told to call whenever we need help. So, if we have an emergency with her, we know we can count on people.
All-Consuming Requirements of Caring for CYSHCN
Interviews with all mothers and grandmothers were replete with descriptions of the unremitting physical, emotional, and intellectual challenges that come with being the primary caretaker of their CYSHCN. Sacrifice and isolation were palpable and repeated in the descriptions of their lives. Most observed in some way they had given their lives over entirely to their child’s care and well-being. Several reported they had moved from their home in Puerto Rico or another country to the United States to take advantage of better care and services.
Two types of narratives were prominent. A number provided a detailed description of the ongoing attention to managing the medical needs of the child. These descriptions generally highlighted the emotional toll of caring for a CYSHCN, requirements for the mother to make medical decisions, as well as to develop and utilize new skills with medical equipment. This mother’s report was representative: She also has other machines, hospital bed, pulse-ox, oxygen, and other machines: feeding pump, a machine to help her with her lungs, like to massage her chest. She also has the albuterol machine. She has a lot of machinery. But I am happy because if there is an emergency, I can give her oxygen until the help arrives.
Others recounted a particularly demanding and stressful event that encapsulated the caregiver experience.
Fate, Faith, and Blessings
Despite the all-encompassing requirements and ongoing challenges of sustaining their CYSHCN and all of the resources and supports needed to maximize their potential, most mothers had come to a spiritual acceptance of their child’s condition and their caretaker role as fate and the will of God. Comments such as that of one mother of a child with permanent consequences of encephalopathy including difficult to manage self-injurious behavior were common: God knows what He does. I have accepted what God has sent me.
Many viewed their responsibility for their children as fulfillment of a purpose in life or a saving grace: If I would have had a normal child, I would probably leave her with my mom and just run around. God knows what could have happened to me. She was born to save me from something, I don’t know what.
Paradoxically, a number of mothers called their child “a blessing.”
Discussion
The major themes identified in our analysis are easily mapped to the themes identified as the important elements of a patient- and family-centered medical home (Figure 2). These major themes have also been identified in some form and strength in a number of previous qualitative studies with parents of children with chronic conditions and special health care needs.17-19

Themes linked to the medical home principles.
We note the theme of waiting can be linked to the need for care that is accessible in the medical home model, but that waiting can mean so much more for a parent of a CYSHCN. One prior study with parents of children with progressive neurodegenerative illness (neurofibromatosis) described the anxious waiting as “holding both joy and sorrow, and containing both suffering and love . . . living in the in-between.” 20 Larson, in her poignant study with 6 Mexican American mothers parenting children with “high burden disabilities,” referred to this consciousness as “the embrace of paradox.” 21
The theme of communication and trust highlights the paramount importance of family-centered care. Similar to our findings, one qualitative study of Mexican mothers living in the United States at or near poverty with children with “high caregiver burden” disabilities noted a paradox in the mothers’ relationships with their children—all of the mothers wished for a cure for their child while at the same time expressing a deep love for the child just as they were. 21 In their study, mothers talked about tensions between their child’s current condition and their hopes for the future, often leading to disagreement with doctors who talked about a poor prognosis.
Cultural and linguistic competency are well understood as core elements of health care delivery systems and the medical home. 22 Studies have looked at the role of language support in caring for non–English-speaking patients. Atkin and Ahmad included 21 interviews conducted in Punjabi, Bengali, and Urdu. These authors characterized the inadequacy of information and lack of language support provided by the health care system as “institutional racism.” 18 Our study highlights the way in which difficulties with language exacerbate issues of waiting, communication, trust, and the cumulative requirements of providing care in often subtle but occasionally dramatic ways. Our study further explores the need for ensuring culturally and linguistically effective care for this vulnerable population.
The all-consuming requirements of caring for CYSHCN speaks to the critical role of comprehensive care coordination in the medical home. 13 A study looking at semistructured interviews with Mexican-American family members of children with chronic medical conditions noted that parents respected their children’s individual characteristics, needs, and preferences; and they planned for an uncertain future. 23
The theme of fate, faith, and blessings further speaks to the need to provide culturally competent care. Our findings are consistent with other literature regarding the role of faith in the families of CYSHCN, but offers a new perspective as caregivers expressed their child was a “blessing” or meant to be their child. The love and caring spirit of the caregivers in our study was consistent and pervasive. Many research studies with parents of CYSHCN note the spiritual path to acceptance of their fate, appreciation of their children, tempting one to think this a common, if not universal experience for parents in these circumstances. 24 Parents of children with significant developmental disabilities who were also members of the Church of the Latter Day Saints used the same terminology as our Latina mothers—my child has been a “blessing.” 25
This study highlights some key challenges and opportunities for Latina parents of children with special health care needs. The unique and supportive role of the medical home for this population suggested by our findings supports prior literature.26,27 However, embracing family-centered care and understanding the plight and care burden of caregivers of CYSHCN is an important lesson. 28 This study affords an in-depth understanding of a vulnerable population often underrepresented in the literature, informing care delivery for practitioners caring for Latino families and CYSHCN.
Conclusion
Latina mothers represent a significant yet underrepresented cohort of caregivers of CYSHCN and medical complexity. The principles of the patient- and family-centered medical home including culturally and linguistically effective care can be applied in unique ways to caring for this unique patient population. Future studies should explore interventions on this population and its association with caregiver and provider satisfaction and health care outcomes and quality of life of their children to promote achieving the quadruple aim (increased patient satisfaction, improved population health, lower costs, and improved provider satisfaction). 29
Footnotes
Acknowledgements
We wish to acknowledge the parents and families who participated in our study. We also acknowledge our staff and the AAP CATCH Grant for supporting this study.
Author Contributions
Dr. Brodie, Bernstein, McNesby and Turchi conceptualized the study design and participated in data analysis. Dr. Brodie and Bernstein drafted the initial manuscript. Dr McNesby and Turchi provided feedback on the manuscript. All authors approved the final version and agree to be responsible for its content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: American Academy of Pediatrics CATCH Grant for supporting this study.