
Abstract
Background. The Choosing Wisely (CW) campaign informs physicians and the public about safety and quality in medical practice. Objective. To evaluate a CW campaign in a medical internship in pediatrics. Methods. An interventionist study with teachers of medicine and pediatric internship students in which the Delphi technique was applied using online questionnaires. Specialists identified 3 unnecessary situations that commonly occur in clinical practice. Following the Objective Structured Clinical Examination (OSCE) model evaluation, a group of students who participated in the educational interventions was compared with another group that was not exposed to the campaign. Results. Most students evaluated the CW campaign content as excellent (64%) or very good (31.6%). The level of successes in the OSCE evaluation was higher in the exposed group when compared with the nonexposed group (P = .001). Conclusions. The CW campaign improved the clinical skills of pediatric internship students.
Keywords
Introduction
Wise management of health resources in medical practice may improve health policies. 1 In the past years, the United States 2 and Brazil 3 spent almost 18% and 8%, respectively, of their gross domestic product on health care. As health care delivery in the technological era has become increasingly complex, cost measurement in health is a challenge.4,5 The treatment of a patient involves many different resources, including personnel, equipment, space, and supplies. Physicians, clinical staff, administrative, and finance professionals should be trained to estimate the costs of resources involved in patient treatment over the care cycle in a conscious and responsible way, to integrate both quality assistance and appropriate use of resources.4,5
Patients would like their personal needs and values to be taken into account. 6 As decision-making is evidence-based and shared with the patient, the management of care has achieved a degree of personalization. 6 The active participation of physicians and patients, as well as the involvement of medical specialties and health institutions, play a fundamental role in reducing the use of unnecessary procedures that result in little or no benefit to the patient. 6 Major drivers of action and initiatives in health care costs include ethics, to ensure patient safety; quality, which involves better clinical practice; reducing costs and increasing the diffusion of innovations for a favorable cost-benefit ratio.5,6
The Choosing Wisely (CW) campaign, launched in 2012 by the American Board of Internal Medicine Foundation, is an initiative to reduce unnecessary conduct in clinical practice. 7 This campaign aimed to change medical practice by assigning specialist organizations the task of pointing out 5 to 10 frequent behaviors (not supported by scientific evidence) that may result in harm or need not be taken and should not be adopted.7,8 The main objective of this campaign is not to rationalize resources, but to “improve the quality of care,” always based on evidence, increasing the likelihood of benefit and reducing the risk of harm to individuals’ health.7,8 Currently, more than 20 countries have adopted the Choosing Wisely International and are already implementing the program in several medical specialties.8,9
The American Academy of Pediatrics (AAP), as part of the CW campaign in 2013, released the first list of 5 topics of testing and treatment considered unnecessary, containing instructions on the use of antibiotics, prescription of cough and cold medications, recommended computed tomography and other neuroimaging tests in cases of suspected cranial trauma and abdominal pain. 10 In Brazil, the CW campaign has not yet been developed by the Brazilian Society of Pediatrics. The objective of this work is to describe and evaluate the strategies of implantation of the CW campaign in the medical internship in pediatrics.
Methods
We conducted an interventionist study with medical teachers and internship students in pediatrics, ninth semester, at a private medical school. The internship in Pediatrics lasts 8 weeks (320 hours). We applied the Delphi 11 technique, using online questionnaires. We asked specialists to list 3 unnecessary situations that commonly occur in clinical practice, obtaining 17 items. Of the 17, the specialists selected the top 5 in total agreement (100%). We conducted this phase of validation using a panel of specialists, grouped the situations by frequency and theme, and adapted the situations to the format proposed by CW. Repeated themes, those lacking scientific evidence or inappropriate recommendations, were excluded. We used a Likert-type scale (4: strongly agree, 3: agree moderately, 2: disagree moderately, 1: strongly disagree) to obtain the specialists’ opinion via e-mail. The situations were ranked, and the 5 situations considered most relevant were used as a guide for educational interventions. An Objective Structured Clinical Examination (OSCE) model evaluation, as a clinical case, using images and a video, based on the recommendations were applied before the introduction of CW campaign (110 students).
During the 1-year period of CW campaign, all students and teachers participated in the following educational interventions: (1) a 2-hour workshop, using audiovisual resources and an active learning methodology. The educational activities covered the following content: presentation of objectives, workshop steps, and CW campaign; discussion about the 5 items on the pediatrics recommendation list with evidence-based justifications; conclusions and discussion of the contents of the workshop. After completing the workshops, the students answered an online training assessment questionnaire, consisting of 3 subjects: the content of the presentation of the campaign, quality of presentation, and discussions in class. (2) We placed banners, containing the 5 propositions in the internship area. (3) The campaign was spread through institution communication channels (literature on propositions and videos). (4) The theme of the campaign was presented in theoretical-practical activities.
The theme of the CW campaign was revisited twice: (1) the theoretical evaluation, at the end of the stage, as a descriptive clinical case, where the recommendations were dealt with in a reflective context. (2) In the OSCE model evaluation, as described before. In this evaluation, 2 groups were compared: a group of students who participated in the educational actions for a period of 1 year (98 students) and another group who underwent the same evaluation before the implantation of CW campaign (110 students).
The questionnaires in all research phases were applied electronically, using the SurveyMonkey platform and sent to the teachers and students’ e-mails. The quantitative variables were analyzed using SPSS 23.0 software. The results were described in tables of distribution by frequency and percentage for categorical variables and in mean and standard deviation or median and interquartile range (IQR) for quantitative variables. The χ2 test was used to compare the performance of the 2 groups of students.
To enhance the transparency and reproducibility of our study, we used the specific Equator checklist for reporting evidence-based practice in educational interventions and teaching (GREET [Guideline for Reporting Evidence-based Practice Educational interventions and Teaching]). 12
This study was approved by the Ethics Review Board of the Bahiana School of Medicine and Public Health, Number 1.627.477, in accordance with the Declaration of Helsinki. All volunteers signed an informed consent form.
Results
The panel of experts was composed of 8 specialist teachers. The median age was 51 years (IQR = 43.2-62.5), with a predominance of females (75%). The median time after graduation was 28 years (IQR = 21.5-36.5) and the weekly workload of 50 hours (IQR = 25-60). All the experts carried out outpatient activities; 87.5% also worked in public and/or private hospitals and 50% reported prior knowledge of the CW campaign.
Ninety-eight out of the 102 students enrolled in the ninth semester participated in the study. Four were excluded for the following reasons: 3 students did not complete the questionnaires fully; and another for being a participant in the CW research group at the institution. The median age was 23 years (IQR = 22-24), with a predominance of females (64%).
The specialists had indicated 3 unnecessary situations that commonly occur in clinical practice, resulting in 24 items. Two of them were excluded due to the absence of theoretical bases and their generalized approach, not specifying the situations in which the recommendation could be applied: “Laboratory tests for discharge in acute patients—clinical improvement defines satisfactorily the moment of discharge” and “To reduce the use of antipyretics in acute febrile illness is a current challenge.” After adapting the propositions to the CW campaign format, excluding repeated themes, we obtained 17 items. The 17 items were sent back to the specialists, using the Likert-type scale, to choose the top 5 items described in Table 1.
Frequencies of the 17 Items Suggested by 8 Specialists of Internship in Pediatrics From a Medical School, Salvador, Bahia, 2018 a .

Abbreviation: n, number of students; CT, computed tomography.
Source: authors’ database.
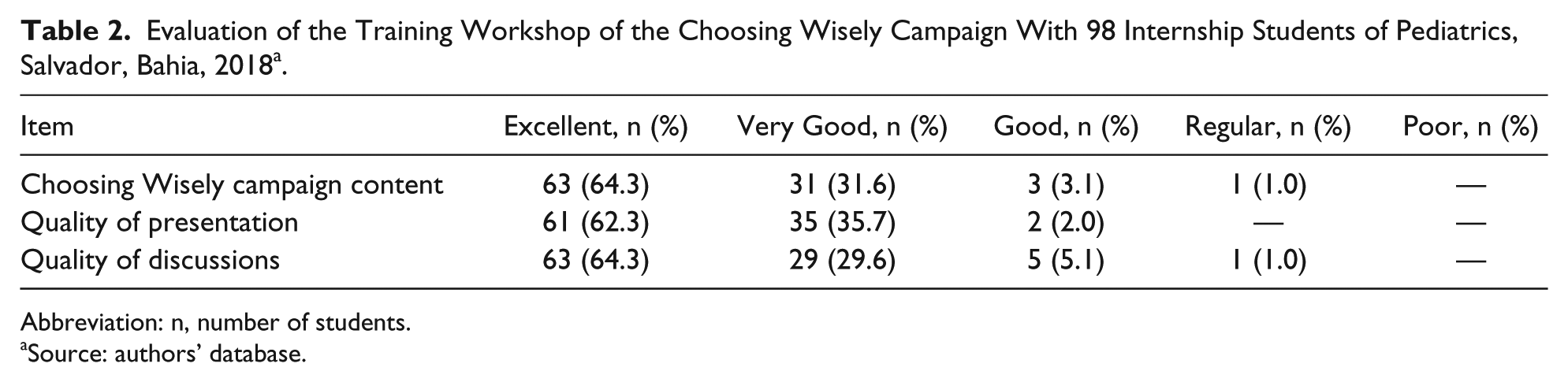
The educational activities were carried out with the participation of all participants, students, and teachers. We conducted 2 workshops and the CW campaign was presented, outlining its history, objectives, and theoretical basis, using audiovisual resources and videos. The research methodology of the CW campaign and the 5 final recommendations were dealt with in a discursive and interactive way. The evaluation of the workshop carried out by the students is described in Table 2. The majority of students evaluated the CW campaign content positively (excellent, 64%; very good, 31.6%).
Evaluation of the Training Workshop of the Choosing Wisely Campaign With 98 Internship Students of Pediatrics, Salvador, Bahia, 2018 a .
Abbreviation: n, number of students.
Source: authors’ database.
At the end of the period, the students carried out a theoretical descriptive evaluation using clinical cases, and 2 of the items in pediatrics were dealt with. All of the 98 (100.0%) students agreed with the assertion, “Don’t request CT scans for minor head injury without warning signs for complications,” and 96 (98.0%) agreed with the item, “Don’t prescribe antibiotics for acute diarrhea without evidence of bacterial infection.” In the evaluation of the OSCE, 2 groups were compared, a group of students who participated in the CW campaign (98 students) and another who did not participate (110 students) as shown in Table 3. The level of successes in the OSCE evaluation was higher in the exposed group when compared with the nonexposed group (P = .001).
Frequency of Answers in the OSCE Evaluation Among Students Who Participated and Did Not Participate in the CW Campaign in the Medical Internship in Pediatrics, Salvador, Bahia, 2018 a .

Abbreviations: CW, Choosing Wisely; OSCE, Objective Structured Clinical Examination; n, medical students.
Source: authors’ database.
Chi-square test.
Discussion
The adoption of cost-conscious attitudes can result in behaviors that do not contribute to the excessive use of resources and bring benefits to patients.1,7 In the present study, we created a list of 5 main items, including examinations and conducts, which doctors should avoid.
Using a method with a panel of experts, the 5 items are supported by evidence in the literature. The first, “Don’t request chest X-rays for non-severe acute asthma without evidence of complications,” is consistent with the finding that it is important to avoid unnecessary exposure to radiation. In addition, in the vast majority of cases of non-severe asthma, especially in the emergency room, there is no recommendation for a chest X-ray, since the initial assessment should be based primarily on clinical criteria. 13
The use of chest radiography in acute asthma in emergencies is indicated especially in severe asthma, which is not responsive to initial treatment, in the presence of comorbidities, pneumothorax and pneumomediastinum, and in very severe asthma with the indication of assisted ventilation. 13 Chest radiography is often normal in about 80% of cases of acute asthma, and when abnormal, most of the findings are nonspecific, typical of the disease, and there is a need for radiological confirmation. 14
Upper respiratory tract infections are one of the most common health problems in pediatric medical care. 15 The second, “Don’t prescribe antibiotics for respiratory diseases of the upper airways suggestive of viral etiology (sinusitis, pharyngotonsillitis, acute otitis media, and rhinopharyngitis),” reflects a recurring theme in medical practice, which is mostly of viral etiology. 16 This coincides with that proposed by the AAP during the CW campaign in the United States. 10 Excessive and unnecessary use causes damage that outweighs the potential benefits, contributing to the formation of bacterial strains, which are more resistant to certain antibiotics, besides adding costs to health services and increasing the risks of adverse events. 16
In Europe, children younger than 3 years of age have between 0.5 and 2 episodes of acute diarrhea per year, one of the main causes of hospitalization in this age group. 17 Between 2000 and 2011, 33 million cases of diarrhea were reported in Brazil, most of them occurred in children younger than 1 year of age. 18 These cases are self-limiting, lasting less than 14 days and usually with resolution in up to 3 days. 16 The episode is secondary to viral agents, rotavirus being the most frequent agent in developed countries, as well as parasitic causes.17,19
The third, “Don’t prescribe antibiotics for acute diarrhea without evidence of bacterial infection,” is related to the use of antimicrobials. Their use is restricted to cases of blood in the stool; with compromised general condition and fever; cases of cholera; acute infection by Giardia lamblia or Entamoeba histolytica; immunosuppression; sepsis; and sickle cell anemia with febrile diarrhea.17,19 The unnecessary use of antibiotics can cause damage to the intestinal flora, leading to the worsening of the clinical status and an increase in adverse effects, which may lead to the development of a resistance to antibiotics.19,20
Traumatic brain injury in children up to 4 years of age is a public health problem. It is an important cause of morbidity and mortality.21,22 Traumatic brain injury is classified as mild, moderate, or severe using the Glasgow Coma Scale. It is classified as mild when the Glasgow Coma Scale has a score higher than 12. The majority of these patients, after a cautious clinical examination, can be released, requiring no specific therapy and have no sequelae. In case of neurological damage, the computed tomography (CT) is the best indication. 23
The Brazilian Society of Pediatrics 22 recommends that CT be used in cases of traumatic brain injury in the following situations: moderate and severe trauma; in mild cases where there is a change in mental state such as restlessness, drowsiness, repetitive questioning, or slow response to verbal communication; when there is a suspected cranial fracture to palpation; prominent subgaleal hematoma in the occipital, temporal, or parietal region; loss of consciousness; when there is a mechanism of severe trauma; falls greater than 0.9 m in children younger than 2 years of age or greater than 1.5 m for children older than 2 years of age; and when the child is not acting normally in the perception of the parents.
Our fourth item is similar to the AAP 10 stating the following: “Don’t request CT scans for a minor head injury without warning signs for complications.” The excessive use of CT in children with mild trauma brain injury exposes them to unnecessary ionizing radiation, potentially increasing their risk of developing cancer, especially in brain tissue. In addition, these examinations also increase costs to the health system. 23 The Brazilian Society of Pediatrics 22 considers clinical observation prior to CT scan to be a more effective approach.
In 2016, a Brazilian study on self-medication showed that cough and cold medications correspond to the fourth most used medication, being 19.2% in the population younger than 19 years of age. 24 Due to this, the number of prescriptions to alleviate the symptoms of upper respiratory infections was very high. 24 Since 1997, the AAP had stated that indications for its use in children had not been established yet. In 2006, the American College stated that there was no literature support for the use of cough medications in the pediatric age group. 25
Our last recommendation is in agreement with the American Association of Poison Control Centers. In 2013, these centers reported that these compounds are in the list of categories of 25 substances most commonly involved in pediatric death due to acute poisoning in patients younger than 5 years. 26
The educational interventions developed over a year in the medical school internship were important not only for knowledge of the CW campaign but also to stimulate reflection on better quality medical practice, based on evidence and less likely to cause harm to the health of the individuals. The workshops were a space for reflection on more cost-conscious attitudes and more adequate use of health resources.
The insertion of the theme of the CW campaign in the theoretical evaluation at the end of the pediatric internship revealed a high percentage of answers to the questions where the items were contextualized with clinical situations of the medical practice. It was possible to evaluate the cognitive learning of theory. When comparing 2 groups of students in the OSCE model evaluation after 1 year of campaign implementation, a significant difference in the correctness of the propositions was observed in the group that was trained, demonstrating the permanence of the acquired knowledge in the long term.
Competence-based learning plays a key role in medical education. Since 1975, OSCE has been used as an important tool for the assessment of clinical skills, knowledge, attitudes, communication, and professionalism. It has been applied in the evaluation of medical students and residents, in summative or formative assessments around the world. Therefore, the OSCE is among the gold standard examinations that may objectively evaluate medical competencies as it is not restricted to the evaluation of knowledge. 27
There is growing evidence that students take unnecessary conduct in training into medical practice. The CW campaign is expected to involve medical students; however, it has still been poorly applied in medical schools. 28 Canada and New Zealand have already systematized this initiative by making students reflect on the harm that excessive examinations and treatments can have on patients, to think about patient-based health care and patient safety. Students are encouraged to create lists of unnecessary procedures involving the participation of patients and teachers.29,30
Research into training in cost-consciousness care in health suggests that the learning of medical students should be accomplished through a combination of specific knowledge transmission, reflective practice, and a supportive environment.31,32 The conscious use of resources in medicine is a topic that is not routinely present in the curriculum of medical courses.33,34
Formal education on cost-consciousness care is necessary and important in the undergraduate curricula. A study with resident physicians showed that only 4.3% strongly agreed that they were aware of the costs and 70% stated that they would reconsider their behavior if they had more knowledge about costs. These results indicate that residents are aware of the limitations of knowledge about procedural costs and, if better informed, would modify the number of requests for tests that would not add value to patient care. 35
Conclusions
The implementation of the CW campaign at the medical school in the area of pediatrics resulted in a reflective process between teachers and students on the adoption of unnecessary behaviors that could generate harm to the patient. The results of the evaluations demonstrate that not only was an increase in knowledge of the CW campaign by medical students achieved but also an improvement in their clinical skills.
Studies at the undergraduate level may help in the training of professionals who can adopt reflexive, evidence-based decision-making, shared with the patient, improving the quality of care with cost-conscious attitudes regarding the rational use of health resources.
Footnotes
Author Contributions
We declare that all coauthors included in this article fulfill the criteria of authorship. DRM has written the article, worked on acquisition, analysis, and interpretation of data; CVNA, LLK, and MSM have worked on analysis and interpretation of data and revised the article critically; RIdO has worked on acquisition of data and critically reviewed the article. All coauthors have critically reviewed it and approved its last version for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.