
Abstract
Purpose. Pediatric femoral supracondylar fractures are difficult to reduce by either closed or open reduction. The abnormal muscle forces around the knee tend to significantly displace the distal short metaphyseal fragment. We describe a novel technique utilizing the combination of a temporarily intraoperative external fixation in order to achieve and maintain the reduction followed by internal fixation. Method. Three male patients younger than 16 years of age were operated in our department. The fractures were defined as pathological in 2 patients. In order to facilitate and maintain fracture reduction, an external fixator was temporarily used intraoperatively; once the fractures were internally fixed, the fixator was removed. Results. Anatomical reduction was achieved in all patients. In an average follow-up of 2 years, all the fractures are solidly healed and the various bone lesions are healing. All patients have returned to regular physical activity. Conclusion. Difficult supracondylar femur fractures in children are easier to manipulate and reduce with the assistance of an intraoperative external fixator. Once the fracture is internally fixed and stable, the external fixator is removed.
Introduction
Pediatric supracondylar fractures of the femur are one of the commonest major pediatric injuries managed by the orthopedic surgeon and represent as many as 12% of femoral shaft fractures. 1 In the older child, the preferred operative interventions include elastic nailing, plating, and external fixation. 2 Recently, more surgeons are advocating the less invasive stabilization system, which allows fracture fixation using a minimally invasive technique with sub-muscular plating. The muscle forces on the distal fragment may present problems in obtaining and maintaining proper alignment of displaced fractures by means of either closed or open reduction. Generally, the distal fragment will displace posteriorly, often with exaggerated flexion, because of the pull of the 2 heads of the gastrocnemius muscle. If the fracture line is just proximal to the distal insertion of the adductor magnus muscle, the distal fragment may also angulate into a varus position. Some of these fractures are pathologic and located very close to the distal femoral physis, leaving a short metaphyseal segment for purchase of internal fixation.1,3-5
We report our experience in treating 3 children with supracondylar femoral fractures, utilizing the combination of a temporarily intraoperative external fixation in order to achieve and maintain the reduction of these difficult fractures, followed by definitive internal fixation. Once the fractures are stably fixed with a plate, the external fixation is removed. To the best of our knowledge, this novel technique for treating pediatric supracondylar femoral fractures has never been described in the English literature.
Materials and Method
This study was approved by our institutional review board (045-19-EMC). We reviewed hospital records and radiographs of 3 male patients younger than 16 years of age, operated during the last 4 years.
Supracondylar femur fractures were defined as fractures within the supracondylar region, extending from the femoral physis distally to proximally, a distance equivalent to the measurement of the widest part of the physis on anterior-posterior radiographs (Figures 1 and 2a and b). 6

Distal segment of the right femur of a child. To be defined as a supracondylar fracture, the center of the fracture should be within the box; in other words, the difference from the center of the fracture to the knee joint should be equal to or less than the width of the condyles.

Patient 1: Supracondylar femur fracture: (a) anterior-posterior view; (b) lateral view.
Operative Technique
All operations were performed on a regular radiolucent operating table. Prior to application of an external fixation, two 5-mm half-pins are inserted anteromedially under fluoroscopic control. The anterior insertion relative to the femur avoids damage to the femoral artery, since the course of the femoral artery is posterior to midline of the femur on the sagittal plane. The first half-pin is distal to the physis and, the second, proximal and perpendicular to the anatomical axis of the femur. At this stage, the fracture is manipulated and reduced, using the 2 half-pins as joysticks. The external fixation with 2 clamps, a swivel type and a regular, is applied to the pins and stably fixed (Figure 3). Through a distal-lateral incision, the femur is approached and a locking compression plate (Synthes, Paoli, PA) is inserted beneath the vastus lateralis and fixed to the bone (Figure 4). In the 2 younger patients, the proximal humeral plate was used, 7 while an adult locking plate was used for the older patient. Once the fracture fixation is completed, the external fixator with the 2 half-pins is removed.8,9

The external fixator in surgery.

Locking plate is fixed to bone, while the external fixator secures the reduction.
A knee immobilizer was used for comfort for 3 weeks. After that, knee range of movement was allowed. The patient was allowed to start weight-bearing on the affected side after signs of union were seen in the radiograph (after 6 weeks). Full level of activity was obtained by 3 months after surgery.
Ethical Approval and Informed Consent
This study was approved by the Emek Medical Center Institutional Review Board (045-19-EMC). Due to the retrospective nature of the study, informed consent of the patients was not required.
Results
Three male patients (aged 12, 12.5, and 15 years) were treated with the same technique by the same senior author (NB; Table 1). All had a supracondylar femur fracture after a fall while playing. Two patients had a pathologic fracture (Figure 5a and b) that was curated and filled with tricyclic calcium phosphate bone substitutes. In an average of 2 years of follow-up, all fractures are solidly healed, and the bone cysts are healing (Figure 6a and b). All patients have returned to full physical activity, except one who is still refraining from any sport.
Patients’ Characteristic and Clinical Data.

Abbreviation: LRS, limb reconstruction system.
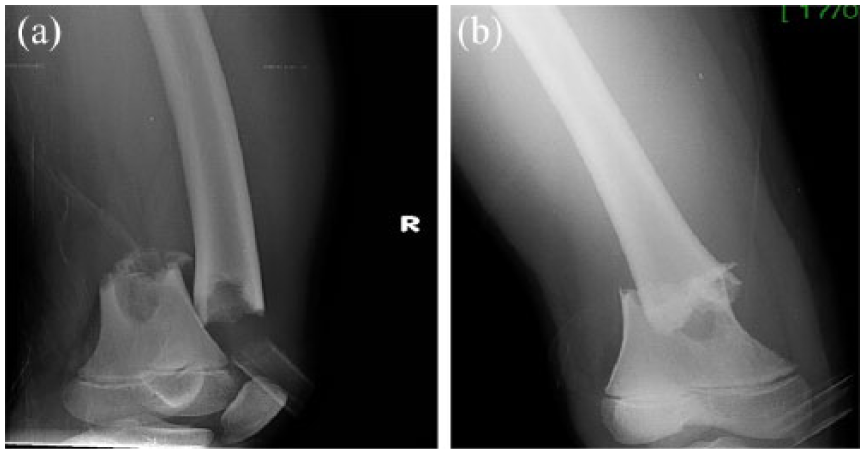
Patient 2: Pathologic supracondylar femur fracture: (a) anterior-posterior view; (b) lateral view.
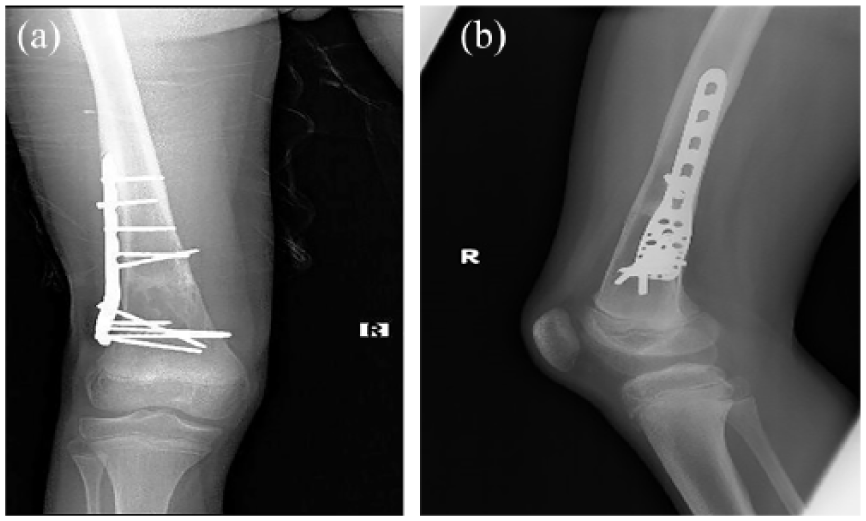
One-year follow-up: The fracture is healed: (a) anterior-posterior view; (b) lateral view.
Discussion
Pediatric supracondylar femur fractures can be challenging to treat, due to instability and displacement of the short metaphyseal fragment. The characteristic muscle forces on the distal fragment present problems in obtaining and maintaining proper alignment of the fractures. Many of these fractures are pathological.2,4 Difficulties in management of displaced supracondylar fractures have been identified by several authors, principally in personal monographs in orthopedic textbooks. Despite this, there is no literature advice on the ideal way to manage the displaced fracture.
Treatment options for this injury include traction, cast brace, external fixation, percutaneous K-wire fixation, open reduction, and internal fixation by titanium elastic nails. All these treatment options have their drawbacks, especially in treating older age children.1,4,5,10-12
For young children (less than 8 years of age), these fractures can usually be treated by closed reduction with percutaneous K-wire fixation and cast augmentation. However, for larger sized children, K-wire fixation with cast immobilization may not provide adequate stability. Also, this treatment is not devoid of complications, such as peroneal nerve injury, growth plate damage, and septic knee. 5 The alternate way of treating these kinds of fractures with external fixation has its downsides: refracture and pin-tract fracture present major impediments to the use of external fixation in the management of femur fractures in the young child. Skaggs et al found a total rate of secondary fractures in the treatment of femur fractures on children treated with external fixation to be 12%. 12
Eight major complications were noted in 6 of 27 patients treated by Gregory et al, corresponding to an overall rate of 30%, including refracture through the original fracture site, fracture through a pin site, post immobilization supracondylar femur fracture, and varus malreduction of 12. 10
Sabharwal described 5 patients with distal femoral metadiaphyseal fractures treated with the Ilizarov external fixation. In 1 patient, a transient drop foot occurred, with isolated loss of motor function of the toes and ankle dorsiflexors, which required the exchange of 1 wire and a half-pin under general anesthesia. There are other drawbacks associated with the use of an external fixator: the bulkiness of the fixator, soft-tissue binding by the bony anchors hindering joint motion along with the possibility of pin site drainage, and prominent scars. Finally, patients may spend a long time in the fixator, which many might not be willing to undergo. 11
Parikh et al describe the treatment of supracondylar femur fractures with elastic nailing in 2 boys and 6 girls with a mean age of 9.0 ± 2.6 years (range = 6-14 years). Four of these patients had pathologic fractures involving a nonossifying fibroma of the distal femur. In their results, 2 of 7 fractures (29%) healed in varus, 3 (43%) healed in valgus, 5 (71%) healed with anterior angulation, and 1 (14%) healed in posterior angulation. The authors found that retrograde insertion of elastic nails for supracondylar femur fractures can be technically challenging, due to the low entry level for nail insertion and the difficulty in crossing the nails distal to the fracture site. 4
In a study by Smith et al, 12 supracondylar fractures of 102 fractures in 96 patients were identified, 7 of which were displaced. 1 Difficulty in obtaining and holding a reduction was encountered in 2 patients, one in a child aged 8 years and 9 months. Failures of reduction with skin traction, closed reduction with crossed pinning, and closed reduction and flexible nailing were noticed. The fracture was finally opened and plated.
Achieving an anatomical reduction with proper alignment of these unstable fractures requires special skills, which are sometimes beyond the ability of many orthopedic surgeons. Therefore, in our patients we suggested the technique that was described for correction of long bones deformities. This combines the accuracy and safety of external fixation together with the patient convenience of internal fixation. The external fixator is helpful in achieving and maintaining reduction of the fracture during the operation, while the plate is inserted and the fracture is fixed. At the end of the operation, the external fixator is removed. 9
In 2 of our patients the fractures were defined as pathological, in one patient through a simple bone cyst, in another through a fibrous cortical defect. Both of these benign lessons are generally seen in metaphyseal areas of long bones, adjacent to the growth plates, and in high frequency at the femoral supracondylar area, needing adequate treatment by curettage, bone grafting, and stable internal fixation.13,14 These fractures, which are very distal in the bone, create a real challenge when it comes to deciding on the measures of internal fixation to be chosen.
Nowadays, internal fixation by plates is the preferred method of most orthopedic surgeons for treating distal femur fractures, where locking plates can be used.15-18 However, regular locking plates will only allow minimal points of fixation in the distal segment between the fracture and the distal femoral physis. The presence of a short distance between the fracture and the distal femoral physis is the main anatomic obstacle to using a simple compression plate (dynamic compression plate). In most cases, there will be a room for only 1 or 2 bicortical screws. This will not be enough fixation for teenagers. The option of extending the plate across the physis and inserting screws in the epiphysis is reserved for older patients near the end of the adolescent growth spurt. Such a plate was used in one of our patients who was 15 years old at the time of injury. Otherwise, in younger patients, early (after few months) removal of the plate is required, and still can result in damage to the physis if the screws violate the physis.
Therefore, in 2 of our patients, we used the adult proximal humeral precontoured locking plates, which have a shape that can easily fit over the distal femur in the pediatric population, as described by Abdelgawad et al. 7 There are multiple options for screw positioning in the proximal part of the plate (applied to the distal part of the bone), and the screws have different directions (divergent, convergent, and straight), which allows for better fixation. It must be emphasized that this plate uses 3.5 mm screws, and therefore may not be strong enough for older patients.
In conclusion, the technique of fixation of the very distal supracondylar femoral fractures described in our article is easy to apply, friendly for the surgeon, and avoids intraoperative difficulties in achieving an anatomical reduction and stable fixation of these fractures.
Footnotes
Author Contributions
NB - Conception and design, acquisition of data, analysis, and interpretation of data, drafting the article, final approval
NR – Analysis and interpretation of data, revising the article, final approval
ED – Acquisition of data, Revising the article, final approval
GR - Conception and design, Acquisition of data, revising the article, final approval
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.