
Abstract
Introduction. S100B protein is a cytosolic calcium-binding protein with a molecular weight of 21 kDa, which is present in various cells and concentrated mainly in the glial cells, which play a vital role in the maintenance of cellular homeostasis in the central nervous system. It is possible that increased S100B protein level might be considered as sensitive and specific indicator to predict early brain damage. Aim. To investigate the prognostic value of serum S100B protein in neonates with perinatal asphyxia (PA) at 24 hours of postnatal age. Methods. A systematic review was performed. Inclusion criteria were studies including data of neonates with PA, monitored with serum S100B, and with neurodevelopmental follow-up of at least 2 weeks. The period of bibliographic search was until January 2017. The consulted databases were MEDLINE, PsycINFO, and Embase. A combination of the following subject headings and keywords was adapted for each electronic database: “perinatal asphyxia,” “hypoxic ischemic encephalopathy,” “hypoxia-ischemia, brain,” and “S100B.” Meta-Disc1.4 software was used. Results. From the 1620 articles initially identified, 6 were finally included and reviewed. The overall diagnostic sensitivity of serum S100B was 0.80 (95% confidence interval [CI] = 0.68-0.88) and the specificity was 0.79 (95% CI = 0.70-0.87). But there was lower predictability value, that is, the positive likelihood ratio was only 3.26 (95% CI 1.74-6.12) and the negative likelihood ratio was 0.32 (95% CI = 0.20-0.5). The diagnostic odds ratio was 12.40 (95% CI = 4.66-33.0). Conclusion. Increased serum S100B level at 24 hours of postnatal life can demonstrate brain damage, but it should not be the only one used to predict PA outcome.
Introduction
Perinatal asphyxia (PA) is an important cause of early mortality and permanent major disability in full-term infants with an incidence rate of 1.14% to 11.7% in China. 1 Approximately 15% to 20% of affected newborns will die within the neonatal period, and 25% to 30% will develop neurological handicaps. 1 PA is caused by impaired placental gas exchange and consists of a cluster of clinical features, including anoxia, metabolic acidosis, and multi-organ failure in neonates. The involvement of the central nervous system is the most consistent clinical feature, and it is the major cause of immediate and delayed brain damage in the newborns, causing life-long neurological disabilities.1-3 It has been shown that there is 49% changes in electroencephalography and 40% changes in cerebral imaging, such as cerebral magnetic resonance imaging, in newborns with PA. 2 Brain damage not only occurs during the acute stage of asphyxia, but also continues for hours, even up to days on and after reoxygenation and reperfusion of the central nervous system. 2 There are 2 stages of neuronal death during PA, primary phase and secondary or delayed phase. Both phases are caused by excitotoxicity, apoptosis, and cytotoxic actions of the activated microglia. It has been reported that the degree of the second stage of neuronal cell energy failure occurring at 24 to 48 hours post-asphyxia can strongly predict the neurodevelopmental outcomes of infants.2-5 Despite the vigorous postnatal monitoring procedures, early diagnosis of the therapeutic window and prediction of long-term neurodevelopmental outcomes of infants remain a challenge. 2 With more understanding of the neuropathology of PA, more biomarkers have been found and are being used in clinical settings. Research studies on animal and human beings showed that selective neuronal necrosis occurs in the basal ganglia, midbrain, brainstem, cerebellum, and spinal cord commonly associated with severe metabolic acidosis. 3 Any involvement with organs, such as brain, liver, cardiac, renal, blood, lungs, and gastrointestinal system, will release organ-specific biomarkers in the cerebrospinal fluid (CSF), blood, and urine. These biomarkers may have a special role in diagnosing the severity and long-term outcomes in newborns with PA.3,4
There are numerous biomarkers indicated for PA. S100B is a member of the S100 family. Because it is soluble in 100% saturated ammonium sulfate solution, it was named “S100.” 5 S100 protein is a cytosolic calcium-binding protein with a molecular weight of 21 kDa consisting of 2 monomers, α and β, which are present in various cells and concentrated mainly in the glial cells of the central nervous system.6-8 Because of its molecular weight, only S100B will be detected in peripheral blood.6-8 It is predominantly released from the astroglial cells after there is hypoxic ischemic damage to the brain, and the ongoing glial cell death will increase the serum concentrations of S100B protein.7-9 Moreover, glia cells play a vital role in the central nervous system, and its function includes regulation of developing brain and maintenance of cellular homeostasis. If glial function is destroyed in pathological conditions, it will enhance neuroinflammation and further neurologic injury. 9 Studies have shown that serum S100B concentration is affected by disturbed blood-brain barrier integrity, renal secretion, or brain volume redistribution; therefore, its concentration level will have positive correlation with brain damage, such as subarachnoid hemorrhage, intracerebral hematoma, subdural hematoma, and cerebral hypoxia.6-8 Due to the breakdown of blood barrier after hypoxia in neonates, S100B protein will continually release into blood and urine and increase the concentration level of S100B. Although S100B protein will come from other organs, that is, muscle, heart, fractured bone, and adipose tissue, extracerebral sources of S100B do not contribute to the increase in serum concentrations. 10 Hence, serum S100B protein is considered a specific protein of brain damage. S100B acts as a neurotrophic factor and neuronal survival protein, and overproduction of S100B can lead to exacerbation of neuroinflammation and neuronal dysfunction. 9 It is possible that increased S100B protein level might be considered as a sensitive and specific indicator to predict early brain damage in newborns with PA.2,11
The aim of this review is primarily to investigate present research evidence on the relationship between S100B protein and the severity of the PA, and the sensitivity and specificity to predict the long-term outcomes in newborns with PA.
Methods
Data Sources and Search Strategy
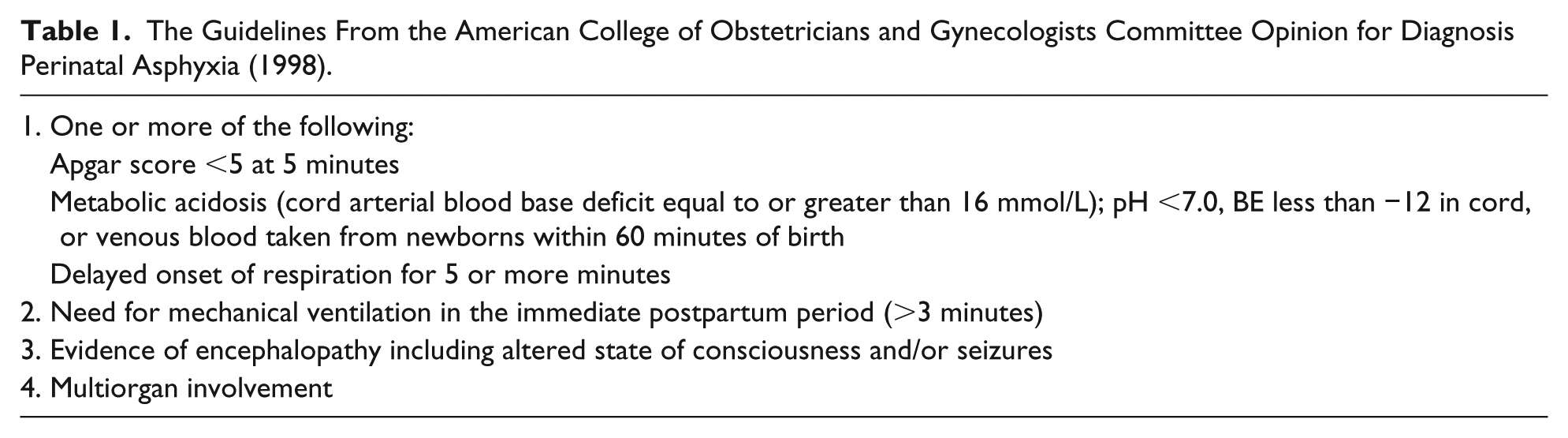
The inclusion criteria for this review followed the guidelines from the American College of Obstetricians and Gynecologists Committee Opinion as listed in Table 1. 12 Infants who fulfilled at least one of the listed criteria were included among the PA newborns. Severity of hypoxic-ischemic encephalopathy was scored according to modified Sarnat and Sarnat score. 13 The period of bibliographic search was until January 2017. The consulted databases were MEDLINE, PsycINFO, and Embase. A combination of the following subject headings and keywords was adapted for each electronic database: “perinatal asphyxia,” “hypoxic ischemic encephalopathy,” “hypoxia-ischemia, brain,” and “S100B.” The initial search strategy is shown in Table 2.
The Guidelines From the American College of Obstetricians and Gynecologists Committee Opinion for Diagnosis Perinatal Asphyxia (1998).
Initial Search Strategy.

Study Selection and Data Extraction
Only studies including (1) human infants with a gestational age of 36 weeks or more, (2) neonatal encephalopathy caused by PA, and (3) neurodevelopmental outcome data follow-up of at least 2 weeks available were eligible. Review articles, opinion articles, and editorials were excluded as well as abstracts of proceedings. A standardized extraction form was used to record the characteristics of each study. For each study, S100B level at 24-hour time point of life was analyzed, and neurodevelopmental outcome after follow-up was recorded. Rates of true positive, true negative, false positive, and false negative were recorded. Neurological outcome was defined as the combination of death or moderate/severe disability.
Statistical Methods
Using Meta-Disc1.4 software, forest plots were constructed to graphically show sensitivity and specificity for all included studies. Summary statistics (sensitivity, specificity, likelihood ratios, diagnostic odds ratio) were calculated. We calculated rates of true positive, true negative, false positive, and false negative data from each study to obtain positive or negative likelihood ratio (LR). A positive LR more than 10 and negative LR less than 0.1 means there is higher accuracy of diagnosis and examination methods and has higher diagnostic value.
Results
A total of 1620 articles were identified. Seventy-two publications were initially preselected on the basis of the articles’ titles and abstracts. Finally, only 6 articles fulfilled the inclusion and exclusion criteria (Figure 1).14-19 Table 3 presents the characteristics of all included articles. Forest plot of sensitivity and specificity with 95% confidence intervals (CI) is shown in Figure 2. To evaluate the predictive value of serum S100B at 24 hours, 6 studies included 364 full-term PA with moderate/severe disability. The overall diagnostic sensitivity of serum S100B was 0.80 (95% CI = 0.68-0.88) and the specificity was 0.79 (95% CI 0.70-0.87). But the positive LR at 24 hours of life was 3.26 (95% CI = 1.74-6.12), and the negative LR was 0.32 (95% CI = 0.20-0.5). The diagnostic odds ratio was 12.40 (95% CI = 4.66-33.0).

Search and section process.
Characteristics of Included Articles.


Forest plot for all included studies.
Discussion
This review provides a summary of the prognostic value of serum S100B in PA with death or moderate/severe disability, as recorded during the first 24 hours after birth. Serum S100B at 24 hours had higher sensitivity, but its positive LR value was only 3.26, less than 10, and the negative LR value was 0.32, more than 0.1; thus, the statistical results showed a lower predictive value. Increased serum S100B level at 24 hours of life should not be the only parameter used to diagnosis or predict PA outcome. Animal experiments have shown that serum S100B concentration level increased between 0 and 24 hours after severe cortical injury in rats, and an increased bilateral S100B mRNA expression 24 hours after mild unilateral cortical contusion in rats in the cortex and hippocampus. 20 In human studies, S100B protein has demonstrated the close relationship with different brain damages, such as traumatic brain injury, ischemia, neurodegeneration, inflammation or infection, and psychiatric disorders. The aim of most human studies was to establish a biomarker of central nervous system damage that could be easily measured, and this biomarker could be an early assessment method. Stroke studies have shown that the peak value of serum S100B after acute stroke occurred 48 to 72 hours after the event. 21 After hypoxic brain damage due to cardiopulmonary bypass and extracorporeal circulation, the S100B peak was reported to occur within 24 hours. 22 However, there are differences for newborns with PA. Comparative studies have investigated S100B in urine, umbilical arterial blood, peripheral arterial blood, saliva, CSF, and serum. This methodology problem would influence the value of S100B, because the half-life of S100B is only 2 hours, and such brain-derived S100B needs to pass at least 2 filters (blood-brain barrier and renal filtration) before it turns up in urine; furthermore, it is hard to obtain S100B level from renal-derived or brain-derived values. Collecting CSF specimens and peripheral blood are invasive processes that need lumbar puncture and femoral artery puncture; thus, it is hard to continue observation for neonate patients. On the other hand, the S100B value is susceptible to the shorter half-life and the treatment of PA. For these reasons, serum S100B could have advantages to reflect the function of astrocytes.20-25
But the results of this meta-analysis demonstrate an opposite situation that could have several reasons. (1) The present study included a relatively small number of patients, making significance difficult to achieve for most of the variables analyzed. (2) Because of different angles attention and error on research means and methods, error produced by various therapeutic effects or individual difference of neonate patients developing nerve system. Similarly, the squeeze and hypoxia in the production process can also damage multiple cells and release cytokines. The effect of factors other than ischemic anoxia is also very important for us to consider. This has led to various cutoff values for serum S100B. (3) There are different neurodevelopmental assessment methods to follow-up the PA patients, such as Amiel-Tison Neurological Assessment, Griffiths Developmental Scales, Bayley Scales of Infant and Toddler Development TM III, Tsumori-Inage Developmental Questionnaire, or nonstandard neurological development test.14-19 The outcomes of PA neonates based on these assessment methods did not generate the research results, which cannot show a strong relationship between the serum protein S100B at 24 hours after asphyxia and neurodevelopmental outcome. S100B mRNA expression will be downregulated after 12 hours and 24 hours of oxygen and glucose deprivation, respectively, and after 48 hours, its value will have significant reduction. However, from genetics, whether the individual S100B gene locus differs in the regulation of chromosomes and whether it will increase the individual specificity of the S100B value remains to be studied. Therefore, serum specimens should be collected before 12 hours of life. In addition, as the half-life of S100B is only 2 hours, its level will drop in a short time. S100B levels peaked in asphyxiated newborns within 2 to 6 hours after birth due to increased permeability of the blood-brain barrier.25-29 Neurotransmitter pathways also affect the S100B concentration because the ischemic anoxic process is completely different from normal physiological processes. The spontaneous generation and the asphyxiation of S100B cause interference in the experimental results. The human body is extremely complex, and the regulatory factors of nerve cells are also very complicated for the regulation of various cells and tissues in the body, and it is bound to have an impact on the S100B value.
In future studies, S100B will be useful as a biomarker because of its reproducibility of measurement, but there are the methodological problems surrounding the measurement of serum S100B. At present, the quantitative measurement methodology of S100B value is not mature enough, which may result in error of measurement. It is possible and necessary to study the dynamic monitoring method of S value in this field. It is also necessary to explore whether the patient’s duration of asphyxia affects the S100B value. What is the time of peaks of the cytokines and the interaction for the PA that we need to talk about in the future? The specimen collection timing within 6 hours and combination of imaging studies, amplitude integrated electroencephalogram, standard neurodevelopment assessment, or evoked potential investigations might help understand the change of S100B concentrations in serum and explore the interrelationship with neurodevelopmental retardation after asphyxia.
Footnotes
Author Contributions
QL, LD, and GC: contributed to conception and design.
QL contributed to analysis and interpretation data and draft the article.
YC, FT, and MZ: contributed to acquisition of data.
TP: contributed to conception and design as well as revise article critically for important intellectual content.
All of authors approval of the vision to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.