
Abstract
Family-based interventions are the current standard for the treatment of pediatric obesity, yet the details of how providers are involving family members, and the barriers to family involvement, are largely unknown. The objective of this study is to describe how providers in pediatric weight management (PWM) involve family members, identify barriers to family involvement, and how they address challenging family dynamics. A cross-sectional survey was administered to PWM centers/clinics and their providers in the United States and Canada. Analyses included descriptive statistics at the participant (N = 71) and clinic/center (N = 47) levels. Providers indicated that they assessed patients and parents’ perspectives, not other family members, motivation, weight/medical history, dietary and activity behaviors, goals, and barriers. Providers also reported that they asked patients’ perspectives about their parents’ aforementioned behaviors, and siblings’ dietary, activity, and sedentary/screen time behaviors, and weight/medical history. Providers reported that the balance between the patient and parent changed as children aged, with more focus given to the child, and less to the parent, as the child grew older. The most frequent barrier to involving family members in treatment included challenging family dynamics. The most challenging family dynamics were divorce/separation and parent-child conflicts. Providers often refer to and rely on mental/behavioral health providers to address barriers to family involvement and challenging family dynamics. Further research is needed to determine adequate provider training and comfort in dealing with family dynamics in treatment, and ways to mitigate barriers to involving families in PWM.
Introduction
In 2007, a multidisciplinary team of experts in pediatric weight management (PWM) developed the Expert Committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity. 1 These recommendations state that providers should be family-based in their treatment of all youth with overweight and obesity seen in PWM centers/clinics. Furthermore, the balance between parents/caregivers and youth during the clinical encounter changes as youth age, where parents are more heavily involved when youth are younger and less involved as youth grow in autonomy as they get older. 1 Family-based PWM involves a targeted caregiver (often parent) and youth,1-3 and is primarily delivered through motivational interviewing and family-based behavioral therapy (FBBT). 4 FBBT targets youth and/or parents’ specific weight-related behaviors and skills, including self-monitoring, goal setting for diet and physical activity, problem solving, behavioral contracting, and relapse prevention.5-7 FBBT has demonstrated robust short-term weight loss and behavior change8,9 and modest long-term weight loss (10 years 5 ). Additionally, one qualitative study found that children valued the increased time spent with families during PWM, which may indicate that family dynamics are improving. 10 Yet it is unclear if youth and/or parent behavior change also leads to changes in how the overall family interacts (ie, family dynamics), which may be needed for long-term sustainable change of behavior.
Without addressing the family dynamics of youth seen in PWM, it is possible that youths’ newly adopted behaviors will not be sustainable long-term without changing family routines, rules, and communication around behaviors that contribute to the development of obesity. Interventions grounded in Family Systems Theory (FST) expand the treatment plan beyond individual behaviors to the dynamics among family members. 11 Relevant to PWM, overall family and parent-youth dynamics around weight-related behaviors are targeted.12,13 According to FST, change happens at the family level to influence overall family functioning and long-term patient and family behavior change. 14 However, there is little guidance and evidence on how providers should involve youths’ family members and how to address challenging family dynamics in PWM.
In 2013, the Children’s Hospital Association (CHA) conducted a survey of 85 hospital-based, Stage 3 comprehensive, PWM departments outlining their structure of care and services. 15 The report details inconsistency in types of services offered from single-clinician to multidisciplinary team-based intervention, increasing referral rates and demand for services, and resulting lengthy wait times for treatment. PWM services commonly included a dietitian (97%) and one or more physicians (86%); mental health and physical activity professionals were included at lower levels (75% and 67%, respectively). The report also noted the required involvement from a parent or caregiver (89%) among the PWM departments surveyed. Despite the information in this report, there was no discussion of how providers are involving family members that attend PWM, and how they are addressing challenging family dynamics and barriers to involving family members. Given that the greatest determinant of a child’s well-being is his/her family, 16 and the centrality of the family to PWM, 1 knowledge and understanding of family dynamics could provide further information for the successful implementation of family-based PWM programming. Thus, building on the CHA report and in line with FST, the purpose of this study is to describe how PWM centers/clinics and providers involve family members, address challenging family dynamics, and experience barriers to family inclusion.
Methods
Subjects
Providers currently employed in PWM centers/clinics were invited to participate in a onetime electronic Qualtrics survey. There is not a central list of PWM programs in the United States, and often PWM centers/clinics are difficult to locate given the variance in naming and labeling of these sites (ie, Center for Pediatric healthy weight, obesity, nutrition, etc). The authors determined the best way to access providers working in PWM would be through commonly used national listservs relevant to PWM providers. Three listservs were used to contact potential participants based on reach to providers working in PWM programs. Building on their prior survey work to operationalize and define hospital-based treatment models in PWM, the CHA listserv was used. 15 The Obesity Society (TOS) Pediatric Obesity and Clinical Treatment of Obesity section listservs were also used given their focus on clinical pediatric and obesity treatment. The survey invitation was posted twice through both the CHA and 2 TOS listservs. The only inclusion criterion was that providers should currently be employed within a PWM center or clinic, and be actively working with youth and/or families in this capacity. More than one provider at each treatment center or clinic could participate in the survey. There were 71 unique and complete participant responses, and 47 unique centers/clinics that participated.
Ethical Approval and Informed Consent Procedure
The survey was approved by The Ohio State University’s Institutional Review Board (#2016B0170) in Columbus, Ohio. Participants were provided a description of the study, the research teams contact information, inclusion criteria, and a link to the survey. Upon clicking the link to the survey, a prompt was provided requesting consent to participate. If participants consented by checking yes, they progressed to the first question. If participants checked no, the survey closed. Following the survey, participants provided their contact information to receive a $10 retail gift card. The survey took participants approximately 20 minutes to complete.
Survey
The authors developed the survey questions to address common barriers and dynamics from the pediatric literature. The survey went through several drafts where feedback was obtained from both providers and graduate students in the process. Prior to distribution, the final survey was piloted among a group of medical, allied health, and mental/behavioral health providers working in PWM. The final survey was divided into 3 different sections: (1) questions about participants and the center/clinic model and team; (2) questions about the inclusion of family members in PWM; and (3) questions about barriers to family inclusion and challenging family dynamics. The survey is provided in the appendix.
Section 1
The first item in Section 1 gave participants the option to provide the name of their center/clinic in order to control for multiple responses from the same setting. This is how we were able to provide both a total number of participating PWM providers and a total number of participating PWM centers/clinics. Participants were asked what discipline(s) they identified with, and which disciplines were included at their center/clinic as part of the routine treatment team: medical (including specialty), allied health (nutrition, physical therapy), mental/behavioral health, and “other.” Participants were also asked to indicate which stage of treatment the center/clinic operated (stages 1-41).
Section 2
Participants were asked to indicate the balance between child and parent involvement, grounded in the Expert Recommendations, 1 during clinical encounters based on the child’s age and development: young child (ages 0-5), school age child (ages 6-10), adolescents (ages 11-15), and older adolescents (ages 16 and older). Participants could select between a 0, indicating they were focused exclusively on the youth, and 10, indicating they were focused exclusively on the parent; middle scores, 4 to 6, indicated a balance between the youth and parent. The next question queried providers about their involvement of other individuals not living in the youth’s home, including family members, friends, or others involved in the child’s life (yes, no) during PWM visits. If providers indicated “yes,” the next set of questions were open-ended inquiring about when during the visit they ask about those not living in the youth’s home, and whom, specifically, they ask about during the encounters.
The following set up questions documented what PWM providers assess during routine clinical visits and from whom (patients, parents, siblings, and additional family members living in the home). Areas of assessment included motivation and readiness to change, weight status and medical history, dietary behaviors, physical activity behaviors, sedentary/screen time behaviors, initial goal setting, follow-up on goals, and barriers to change. There were 3 questions in this section: “I assess the behaviors, histories, and goals from the following family members”; “I assess the perspectives of the patient’s behavior, history, and goals from the following family members”; and “I assess the patient’s perspective of their parent and/or family member’s behaviors, histories, and goals.” The last question contained the responses for parent(s), siblings(s), and additional family member(s) in the home. These 3 questions were quantified by the frequency of “yes” and “no” responses for each individual item.
Section 3
Participants were asked to indicate if they had experienced (yes, no) the listed common barriers when working with parents and family members in treatment, including challenging family dynamics, parents and family members resistant to change their own behavior(s), lack of resources in family (ie, insurance, transportation), unhealthy parental modeling, family history of obesity, time limitations, resistance to change child’s behavior, parent/family does not agree that the child’s weight status is a concern, and other. Participants were also asked to rank order the top 3 barriers they commonly experienced from this list. A weighted ranking of participants’ top 3 noted barriers was computed by multiplying their first ranked barrier by 3, second ranked barrier by 2, and third ranked barrier by 1.
Participants were queried about common time limitations experienced by families in PWM, including work schedule, school schedule, or other time limitations (yes, no). Participants were asked to indicate if they experience common challenging family dynamics in PWM (yes, no), including divorce/separation, parent-child conflicts, parenting skills, inappropriate expectations of child’s level of responsibility for behavior change, siblings with different weight statuses, custody arrangements, extended families’ influence on child, weight teasing from parent to child, weight teasing from sibling to patient, sibling conflicts, and other. Following this question, providers were asked via an open-ended question how they address challenging family dynamics in treatment. They were then asked how satisfied they are with their approach to addressing challenging family dynamics, using a 5-point Likert-type scale (very dissatisfied, dissatisfied, somewhat satisfied, satisfied, and very satisfied). The categories “very dissatisfied and dissatisfied” and “satisfied and very satisfied” were collapsed for analysis. If providers indicated experiencing any of these challenging family dynamics, they were asked if they refer out to other professionals to treat these dynamics (yes, no), and if so what discipline(s) they refer to (open-ended). Finally, participants were asked how challenging family dynamics are shared with the treatment team (open-ended), if they are routinely documented (yes, no), and where they are routinely documented: intake forms, medical record, intake form, not document, or other.
Analysis
Analyses were conducted at the participant/provider and center levels. Descriptive statistics and cross tabulations were used. Open-ended text was coded to produce frequencies for participant responses within each open-ended question, and only the top categories of participant responses were reported. Results and discussion are organized based on the 3 survey sections.
Results
Section 1: Questions About PWM Centers/Clinics Care Model
Seventy-one providers participated, representing 47 centers/clinics in the United States and Canada. Only providers with completed surveys (N = 71) were used in the analysis. Seven out of 71 providers did not include the name of their clinic/center, but were included in analyses at the provider level. Based on the CHA study, 15 this roughly represented 55% of their center/clinic respondents (47 vs 85). Providers were allowed to select more than one discipline (ie, RN and RD); hence, the number of disciplines reported for the sample sizes are slightly higher than the overall number of participating providers. Providers identified as medical (n = 51), allied health (n = 29), medical specialty (n = 11), and/or mental and behavioral health (n = 13) providers. Out of 47 treatments centers/clinics, 44 reported having a medical provider, 45 an allied health provider, 24 a medical specialist, and 39 reported having a mental/behavioral health provider as part of their treatment team. Four providers indicated the inclusion of “other” on their treatment team (ie, health educator and child life specialist). Providers reported that their center/clinic conducted care at stage 1 (n = 4, 6%), stage 2 (n = 14, 20%), stage 3 (n = 24, 34%), and stage 4 (n = 29, 41%). All providers that include the names of their PWM centers/clinics also reported having at least 2 providers from different disciplines on their teams. Two providers, who did not include the name of their PWM center/clinic, only reported having one medical provider.
Section 2: Overall Questions About Including Family Members
In line with the Expert Recommendations, 1 providers reported adjusting the focus of their encounter between children and parents depending on the child’s age (see Table 1). Greater emphasis was placed on parents of younger children ages 0 to 5 years (mean [M] = 8.85, standard deviation [SD] = 1.41, range 3-10), and more emphasis was placed on older adolescents ages 16 and older (M = 4.18, SD = 2.31, range 0-10). Providers somewhat equally targeted parents and children ages 6 to 10 (M = 7.18, SD = 1.54, range 2-10) and adolescents ages 11 to 15 (M = 5.55, SD = 1.78, range 3-10).
Balance Between Child and Parent Involvement During Clinical Encounters Based on Child Age Group, on a Scale From 0 (Child Only) to 10 (Parent Only).

The majority of providers indicated that they ask about additional individuals not living in the child’s home, but who are involved in the child’s life during the encounter (n = 63, 89%). Providers indicated that they asked about these individuals during history taking (n = 26; general, family, social, and medical history), at the intake or first visit (n = 16), varying times and as needed (n = 11), and during the initial assessment (n = 7). When asking about additional individuals not living in the child’s home, providers most frequently asked about the category (n = 25) of school/childcare, afterschool care providers, and time spend with others during weekend and extracurricular activities. The second most frequent response (n = 21) was grandparents, third (n = 18) was parent/caregivers not living in the home (ie, stepparents), and then friends in general (n = 16), and family in general (n = 14; ie, aunt, uncle, cousins).
Providers indicated that they assess both the patient and the parent for motivation/readiness to change (RTC), weight and medical history, dietary behaviors, physical activity behaviors, initial goals, follow-up goals, and barriers to change (see Table 2, top section). However, for sedentary and screen time behaviors they reported mainly assessing only the patient’s perspective (n = 61, 87% yes). They less frequently assessed siblings and additional family members.
Assessment of Patient and Family Members’ Behaviors, History, and Goals (n, [% Yes]).
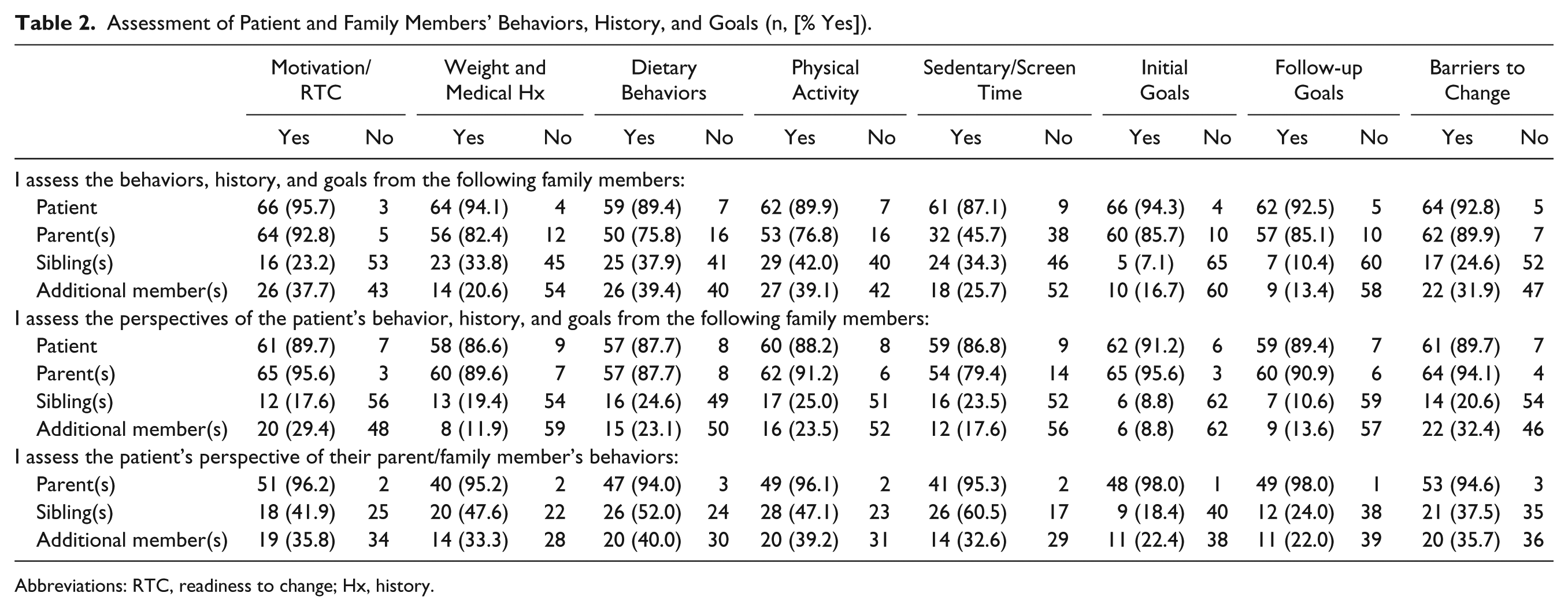
Abbreviations: RTC, readiness to change; Hx, history.
Providers asked both the patient and the patients’ parent(s) about patient’s own motivation/RTC, weight and medical history, dietary behaviors, physical activity behaviors, sedentary and screen time behaviors, initial goals, follow-up goals, and barriers to change (see Table 2, middle section). Providers did not frequently ask the siblings and additional members living in the home about the patient. Overall, providers reported asking patients about their parents’ behaviors in all categories (see Table 2, bottom section). Providers reported asking patients about their siblings’ physical activity behaviors (yes n = 28, 47%) and sedentary/screen time behaviors (yes n = 26, 61%); however, providers were divided between asking patients about their siblings’ weight and medical history (yes n = 20, 48%) and dietary behaviors (yes n = 26, 52%);and did not ask about the patient about their siblings when considering initial (yes n = 9, 18%) and follow-up goals (yes n = 12, 24%) and barriers to change (yes n = 21, 36%). Providers were split in asking patients about the dietary behaviors of additional family members living in the home (yes n = 20, 40%), but otherwise did not ask the patients’ perspective about additional family members in the home on the rest of the categories.
Section 3: Family Barriers and Challenges Questions
Providers indicated that the most frequent barriers to involving parents and family members in treatment were the following (see Table 3): challenging family dynamics (yes n = 66, 93%), parents and family members that are resistant to change their own behaviors (yes n = 64, 90%), and lack of resources (yes n = 61, 86%). The top 3 ranked barriers by providers were parents and family members that are resistant to change their own behaviors, unhealthy parental modeling, and lack of family resources.
Barriers Experienced When Involving Parents and Family Members in Treatment.

Weighted ranking done by multiplying first by 3, second by 2, and last by 1.
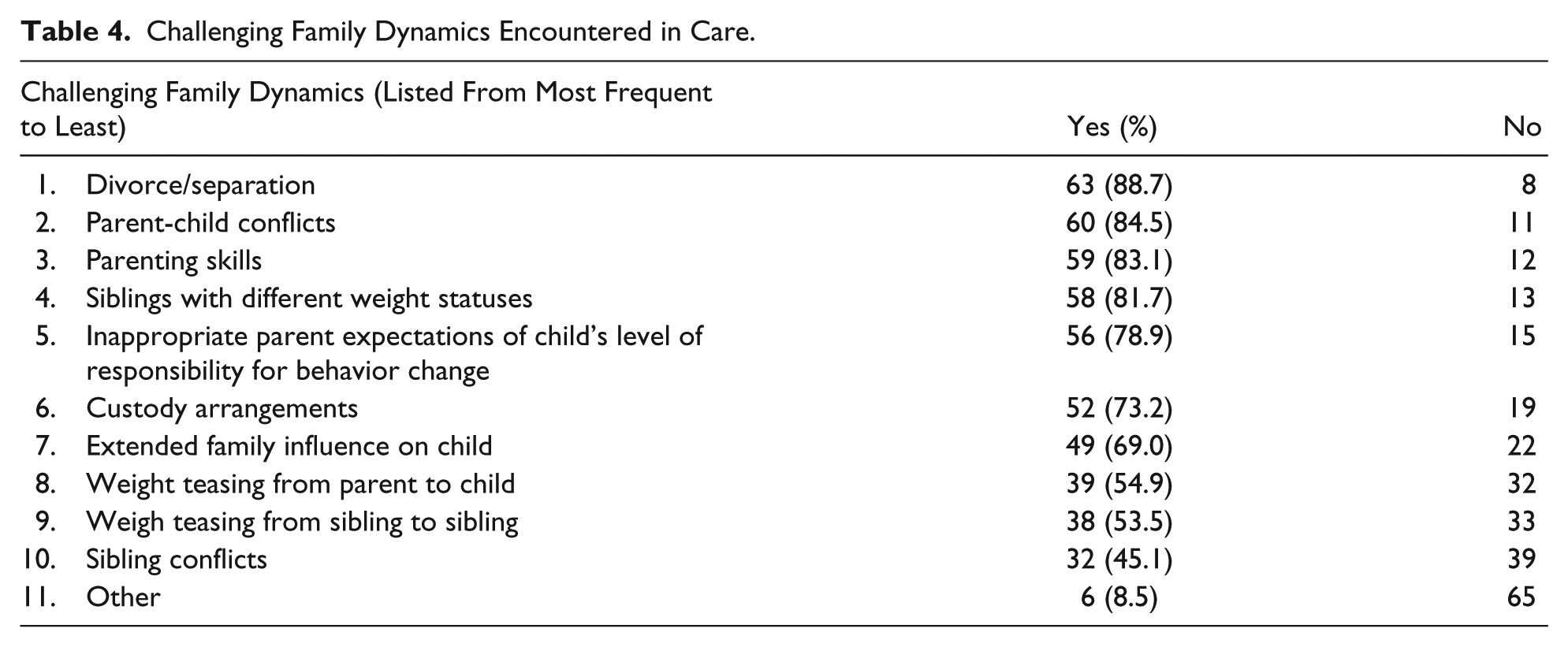
Providers noted frequent time limitations of work (yes n = 48, 68%) and school schedules (yes n = 45, 64%). Other time limitations providers mentioned included afterschool and extracurricular activities, sibling schedules, homework, travel time, and distance to appointments. The most common challenging family dynamics reported by providers included the following (see Table 4): divorce/separation (yes n = 63, 89%), parent-child conflicts (yes n = 60, 85%), and parenting skills (yes n = 59, 83%).
Challenging Family Dynamics Encountered in Care.
Providers indicated that they addressed challenging family dynamics by referring to mental/behavioral health providers (n = 26), use motivational interviewing (n = 12), apply their own communication skills (n = 10), include all family members in treatment (n = 9), and set small, realistic goals (n = 7). Providers were closely split in their satisfaction with their approach to addressing challenging family dynamics: satisfied/very satisfied (n = 22, 29%), somewhat satisfied (n = 28, 41%), very dissatisfied/somewhat dissatisfied (n = 18, 26%).
The majority of providers reported referring out when they experienced challenging family dynamics (yes n = 55, 81%). Providers indicated that they referred most frequently to psychologists (n = 28), social workers (n = 14), behavioral therapist in general (n = 7), family therapist (n = 7), and counselors (n = 5) for challenging family dynamics. The majority of providers reported a history of documenting challenging family dynamics (yes n = 66, 97%). However slightly less routinely did so (yes n = 57, 92%), most often in the medical record (yes n = 58, 82%), intake form (yes n = 20, 28%), or other places like notes by mental/behavioral health providers (yes n = 8, 11%). Providers shared challenging family dynamics verbally (n = 19), during team meetings (n = 15), in chart notes (n = 12), through mental/behavioral health provider communication (n = 8), and in a multidisciplinary/collaborative way (n = 7) or during rounds (n = 5).
Discussion
Consistent with the CHA 2013 report, 15 the majority of providers in our study were part of multidisciplinary PWM teams, with at least one medical provider and dietician, and offered a variety of different services. Additionally, providers in our study also reported assessing parental health and weight history in addition to the patient. Congruent with the Expert Recommendations, providers reported that the balance between the patient and parent changed as children aged, with more focus given to the child, and less to the parent, as the child grew older. 1
The majority of providers reported that they asked about additional family members (siblings, others living in the home) and friends, but there was no consistency about when this was assessed or whom they tend to ask about. Similar to prior research, 17 in this survey providers overwhelmingly only ask the patient and parent about motivation/readiness to change, weight and medical history, dietary and physical activity behaviors, screen time/sedentary behaviors, goals, and barriers to change. This indicates an inconsistency between providers’ reports that they ask about additional family members, but do not inquire about clinical behaviors, history, goals, or barriers from these members. A small qualitative study in a PWM program gives evidence that other family members are both aware of and affected by the patient and parent participating in treatment. 13
Although providers identified barriers to family involvement and challenging family dynamics, the majority reportedly refer to mental/behavioral health practitioners, who may not be part of their treatment teams, to deal with these barriers and dynamics. It is not known how often families accept these referrals and engage in counseling. Additionally, the documentation of family dynamics and sharing of these dynamics among the treatment team was inconsistent. Researchers have identified that poor family functioning (an indication of the overall family dynamic) is associated both with childhood obesity and the risk of children developing obesity. 18 Furthermore, Zeller and colleagues found impaired family functioning in approximately 1 out of every 2 to 3 families in their sample of adolescents receiving weight loss surgery. 19 Given prior research about impaired family functioning among youth with obesity, assessing family functioning in childhood obesity clinical encounters could give providers a structured way to assess and monitor the aforementioned barriers and challenging dynamics.
Clinical Practice Implications
Overall, providers indicated that they ask about additional family members and individuals beyond the parent-patient dyad, and noted barriers and challenging family dynamics about these groups. Yet how these groups were assessed or involved in the encounter was inconsistent, and when challenges arose, referrals were made to mental/behavioral health providers. It is likely that these barriers and dynamics place further challenges on families with respect to attendance and compliance and contribute to their attrition from treatment. Providers likely do not have a framework for what to do with information from additional family members and individuals beyond the behaviors of the patient-parent dyad, and need further training for how, when, and to what extent to assess and involve these members in the encounter.
Family Systems Theory suggests expanding the treatment plan beyond individual behaviors to the dynamics among family members, so that change happens at the family level to influence overall family functioning and long-term change. 14 Additionally, according to FST, the family and PWM team become a sort of system, creating their own dynamic where the team and family ultimately influence and are influenced by each other. Therefore, if barriers to family involvement and challenging family dynamics are not addressed and integrated into treatment, the alliance between the patient, family, and team may suffer.13,20,21 Furthermore, relying heavily on mental/behavioral health referrals to deal with challenging dynamics may provide additional complication, as many of these providers are not specifically trained in dealing with family dynamics in relation to obesity and PWM.22,23 The reliance on mental/behavioral health referrals without clear communication channels may also lead to fragmented care, without a clear mechanism for integrating treatment goals. Future research should look to determine ways to mitigate barriers to family involvement and design training for providers on family inclusion and treatment of challenging dynamics.
Strengths and Limitations
We cannot assess a nonresponse rate since we do not have an accurate idea of how many individuals are part of the 3 listservs, and the likelihood that listserv numbers fluctuate over time. However, a strength of this study is that the survey was nationally distributed through 3 different listservs to providers working in PWM centers/clinics. Given that the purpose of the study was to obtain a baseline description of how challenging family dynamics and barriers to family involvement are treated, this study provides a foundation to more rigorously assess these challenges and barriers. The greatest strength of this study was the assessment of barriers to family inclusion and challenging family dynamics. The lack of empirical evidence assessing family dynamics in PWM is limited, and there are no validated survey measures to assess these topics from providers. Thus, it is possible that there are other important barriers and dynamics relevant to PWM that we did not assess that should be included in future studies. A final strength of our study was the inclusion of providers from any clinical discipline working in PWM. Due to our sample size and the diversity in disciplines, we did not have adequate power to run analyses comparing responses with all discipline categories.
The purpose of this survey was first to understand what is happening, descriptively, with respect to barriers for family involvement and challenging family dynamics. Future research should look to determine ways to mitigate barriers to family involvement and design training for providers on family inclusion and treatment of challenging dynamics.
Footnotes
Appendix
Author Contributions
KJP: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JAS: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
IE: Contributed to conception; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
DNC: Contributed to conception; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SL: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.