
Abstract
Objective. To assess gender differences in infants diagnosed with neonatal abstinence syndrome at the Cabell Huntington Hospital in Huntington, West Virginia. Methods. This is a single-site retrospective chart review involving 97 infants born treated for neonatal abstinence syndrome at the Cabell Huntington Hospital between April and December 2015. Data were obtained from electronic medical records using a secure online survey tool designed using Qualtrics. Maternal demographics and drug screenings were collected. Infant information was collected for the first 7 days of life including withdrawal symptoms, treatment, and growth parameters. These data were analyzed based on gender, male (N = 62) and female (N = 35), to assess any gender differences among the infants. Results. No significant differences were found regarding birth weight, length, and gestational age between male and female infants. Differences among the percentage of symptoms experienced were found with females experiencing a greater percentage of symptoms affecting the autonomic nervous system compared with males. Significant differences in head circumference were found in these infants; females were found to have a greater head circumference at time of birth compared with males (P = .003), whereas at time of discharge head circumference was greater in males than in females (P = .035). Conclusion. Differences in symptoms, physical characteristics, and methadone treatment were found between male and female infants diagnosed with neonatal abstinence syndrome at the Cabell Huntington Hospital during 2015. Further studies are needed to assess both the short- and long-term effects of antenatal drug abuse.
Introduction
The current state of the nation’s substance abuse and addiction epidemic has reached emergency status. However, this status has been in a state of emergency in rural West Virginia for over 5 years. In Cabell County, West Virginia, arguably the epicenter of the state’s substance abuse emergency there has been a sharp increase in the prescribing rate for opioid analgesics, rates of opioid overdose (from 146 in 2012 to 944 in 2015), and of overdose deaths from 2012 to 2016. 1 In addition to the rate of overdoses in Cabell County, there has also been a significant increase in substance abuse among pregnant females that has resulted in an increase in number of infants being diagnosed with neonatal abstinence syndrome (NAS). NAS is a postnatal drug withdrawal syndrome that occurs following in utero exposure to drugs. Nationally, the incidence of maternal opioid use during pregnancy is 5.6/1000 live births. During this time, there was a subsequent 5-fold increase in the incidence of NAS, resulting in an estimated 21 732 infants born in the United States in 2012.1,2 Using Centers for Disease Control and Prevention reports, West Virginia has the highest rate of babies born with NAS in 2013 at 33.4 per 1000 births. 3 Infants suffering from NAS are more likely to develop adverse health outcomes including low birth weight, preterm birth, admission to the neonatal intensive care unit (NICU), and may require pharmacological treatment that can lead to an extended hospital stay and higher health care expenses. The average length of stay for an infant with NAS was 16.9 days compared with the average 2.1 day stay for non-NAS infants. This extended length of stay is associated with an estimated average cost between US$66, 700 and US$93, 400 per infant depending on need for treatment for the infants with NAS, compared with the US$3500 for infants without NAS. Medicaid coverage accounted for many hospital charges, with 81.5% of infants diagnosed with NAS enrolled in state programs during 2009 to 2012. 1
In infants suffering from NAS, maternal opioid use is the most common cause for this syndrome; however, other drugs such as psychostimulants, selective serotonin reuptake inhibitors, barbiturates, benzodiazepines, and cannabis have also been shown to cause neonatal withdrawal.4,5 There are many factors that influence the onset, severity, and duration of withdrawal symptoms, including duration of exposure, time since last dose, as well as the type, amount, half-life, and ability of the drug to cross the placenta. Polysubstance abuse of drugs, tobacco, and alcohol are also common among substance abusers and can affect the development and degree of withdrawal in exposed infants. 6
This postnatal withdrawal syndrome is characterized by a variety of symptoms that typically manifest during the first 48 to 72 hours after birth involving the central nervous, autonomic, and gastrointestinal (GI) systems. 7 Opioids are most commonly seen in infants with NAS, and their action on opioid receptors within the developing fetus is the underlying mechanism for an array of withdrawal symptoms. For example, symptoms might include numerous changes in neurological functions such as tremors, seizures, exaggerated moro reflex, and yawning. Infants with NAS often experience GI disturbances and common symptoms include vomiting, diarrhea, and poor feeding. Fever, sweating, mottling, increased heart rate, and sneezing are symptoms associated with dysregulation of the autonomic nervous system. 7 To monitor the progression of withdrawal symptoms associated with NAS, babies are commonly evaluated using the Finnegan scoring system. 8 Developed in 1975, infants are assessed every 3 to 4 hours for signs of withdrawal, and observed symptoms are quantified and recorded as abstinence scores. These abstinence scores are used to determine severity of withdrawal, need for pharmacological intervention, and guidance for weaning. 9 Morphine and methadone are commonly used to treat infants with increased abstinence scores who need pharmacological intervention.
In this retrospective study, we have collected both maternal and patient data from infants who were diagnosed with NAS at the Cabell Huntington Hospital (CHH) in Huntington, West Virginia, which is Marshall University’s major medical teaching institution. Recently, the clinician-academics group treating and monitoring infants with NAS at CHH published that between 2010 and 2015, the number of infants treated for NAS at CHH increased by 219%. 10 The goals of our report is to provide details on infants with NAS who were born in 2015, the peak of this region’s NAS epidemic during this 5-year period with details on demographics, infants born with NAS physical measurements, average Finnegan scores for the first 7 days of treatment, methadone doses and frequencies, and potential gender differences.
Methods
Data Collection
This is a single-site, retrospective chart review conducted between April 2015 and December 2015. Before data were collected, institutional review board approval was obtained from Marshall University Institutional Review Board. Data were collected from the electronic medical records used at CHH using a specialized and secure online survey designed using Qualtrics. This survey was designed to collect an extensive list of patient information from the mother and the infant before and during treatment for NAS and was designed to minimize user error during the extraction and collection of data from the electronic medical records used at CHH. Only infants admitted to the NICU and/or the neonatal therapeutics unit between April 2015 and December 2015 treated with methadone for NAS were collected and analyzed. Details of age, ethnicity, marital status, level of education, insurance status, recipient of prior treatment for substance abuse, hepatitis C status, drug screen results from either urine of umbilical cord, and the type of delivery were collected from each mother who delivered an infant suffering from NAS. For each infant diagnosed with NAS, the following maternal information was collected: prenatal care, polysubstance abuse, and toxicology screen results. Also, the following infant birth parameters were collected: gestational age, day, month and year of birth, weight, length, head circumference (HC) at birth and on discharge, gender, ethnicity, and Finnegan (ie, NAS) scores for up to 7 days following the initial diagnosis of NAS. All data were recorded without identifiers to maintain patient confidentially. For collecting scores and recording withdrawal, the standard, most commonly used 21-point Finnegan scoring method was used. We recorded the initial day of scoring following birth up until the seventh day of life. The day and time of the highest Finnegan score was also recorded. The Finnegan scoring method is divided into systems: central nervous system, GI, respiratory, and autonomic disturbances. The following were assessed for central nervous system disturbances: crying, sleep, reflexes (eg, hyperactive Moro reflex), tremors, muscle tone, myoclonic jerking, convulsions, and excoriation. The following were assessed for GI disturbances: excessive sucking, poor feeding, projectile vomiting, and loose and watery stools. For respiratory system disturbances, nasal flaring and respiratory rate with and without retractions were recorded; and last, for disturbances in the autonomic system, the following were recorded: sweating, fever, frequency of yawning, mottling, nasal stuffiness, and sneezing were recorded for each infant diagnosed with NAS.
Regarding data on methadone treatment, the methadone protocol initiation date and time following birth was recorded as well as the termination date and time. Also, the frequency and doses of methadone administered at each step of the treatment protocol as well as the total (mg) amount of methadone administered were all recorded for up to 7 days following initiation of the methadone treatment. We also collected the in utero exposure information from what was either self-reported (maternal history) or provided from urine and/or umbilical cord toxicological reports either during pregnancy or at time of delivery. Inclusion criteria included patients initiated on methadone between April 2015 and December 2015 admitted to the NICU and/or neonatal therapeutics unit at CHH. Exclusion criteria included patients started on methadone prior to admission at CHH and infants transferred to or from another facility during treatment. The primary outcome was to determine the differences in NAS symptoms and scores between male and female infants receiving oral methadone. Also, total amount of methadone (mg/kg), time (hours) to recording the first NAS score, peak NAS score within the 7-day period following birth, and the peak NAS score during the first 24 hours of life were recorded and compared between genders. Patient information included birth weight (kg), length (cm), HC (cm), gestational age (weeks), and the duration of treatment (days).
Data Analysis
Infants were divided into 2 groups for analysis based on their gender, male (N = 62) or female (N = 35). Mean data and percentage (%) difference between males and females with NAS symptoms were calculated and are presented in Tables 1 and 2. Statistical analysis was run on the data using the Student’s unpaired t test. P < .05 was considered statistically significant.
Comparison of Neonatal information data at birth and discharge between genders.
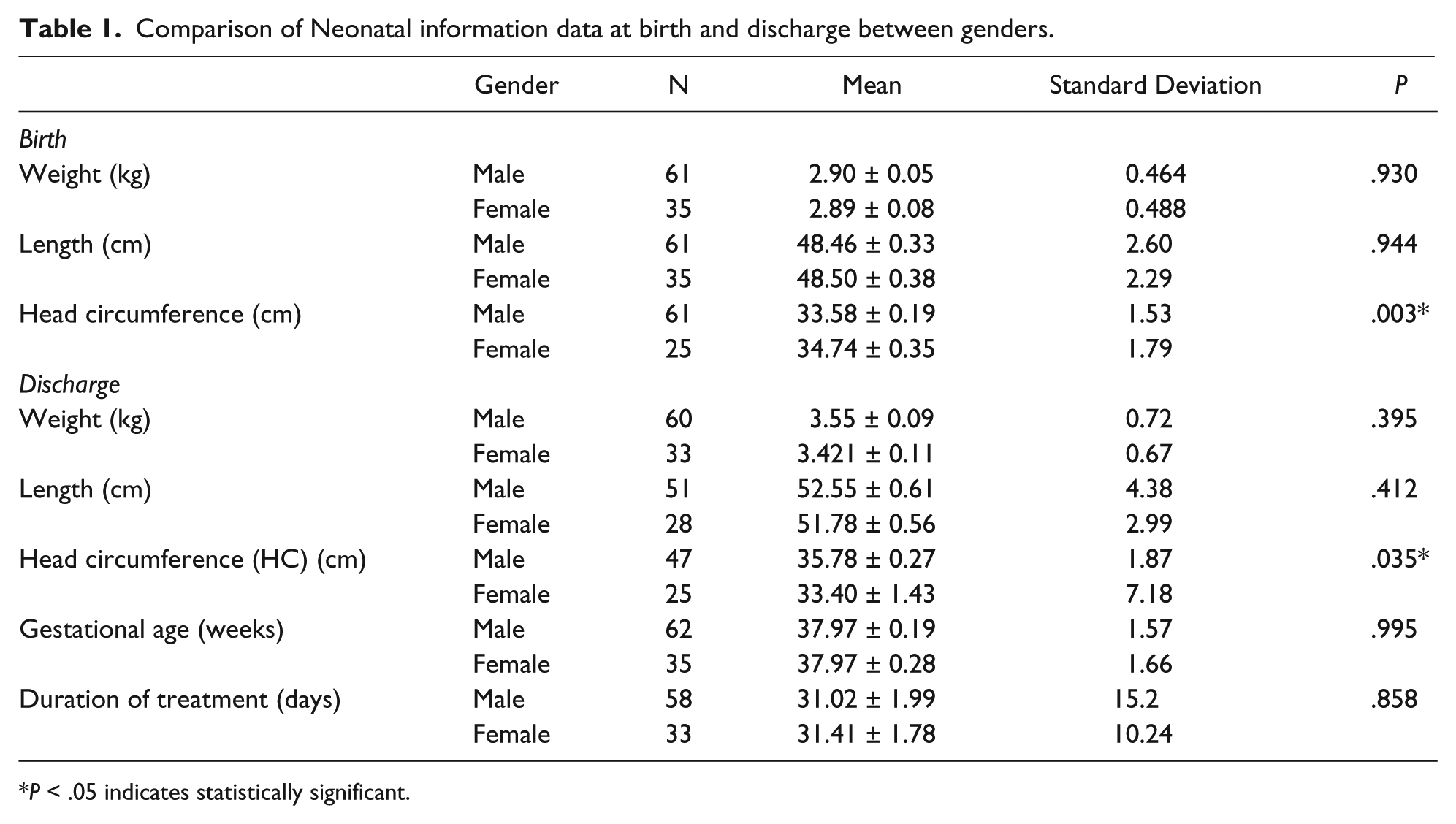
P < .05 indicates statistically significant.
Comparison of NAS symptoms scores and methadone dosing (mg/kg) between genders.
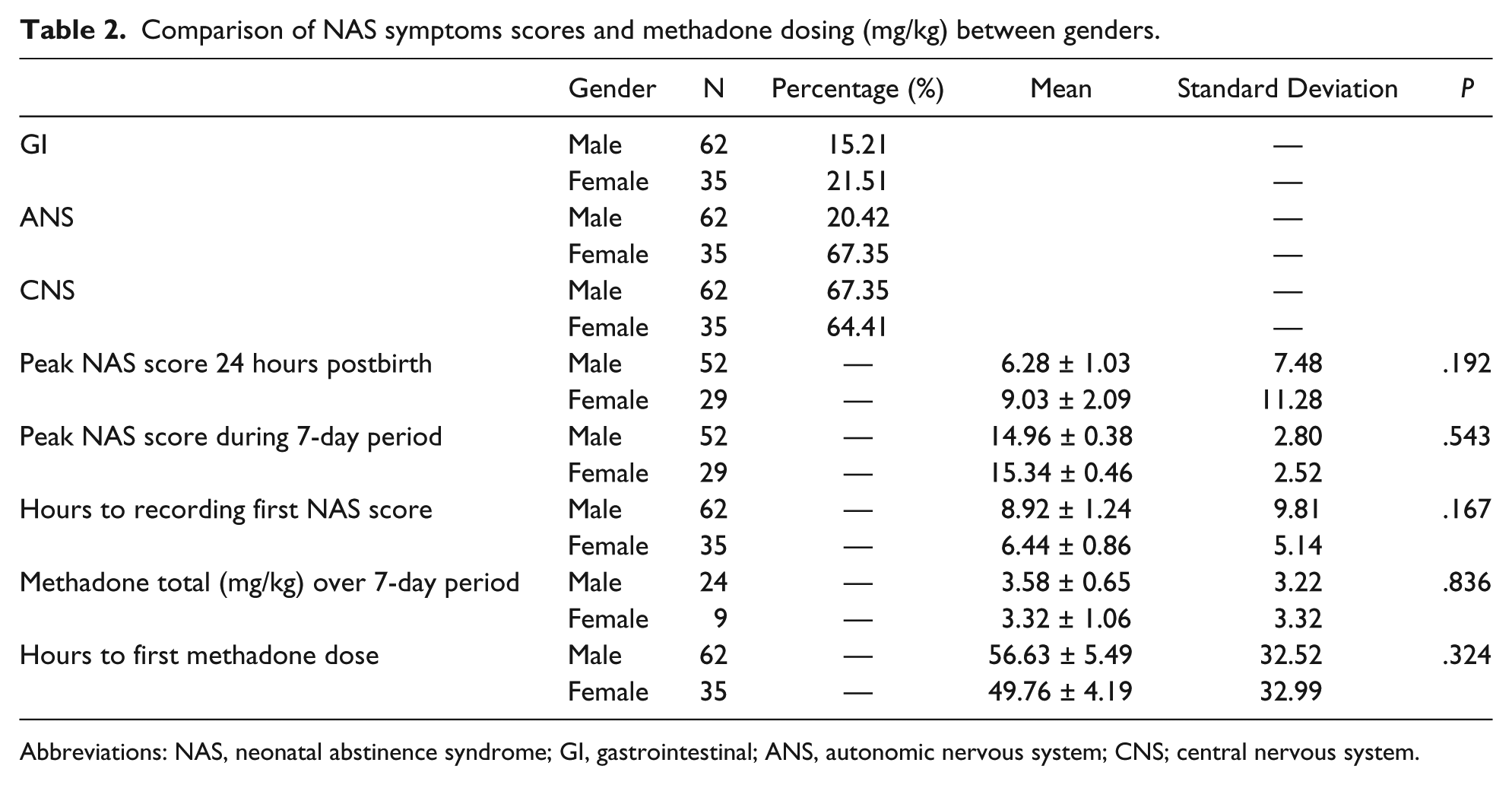
Abbreviations: NAS, neonatal abstinence syndrome; GI, gastrointestinal; ANS, autonomic nervous system; CNS; central nervous system.
Results
Patient Characteristics and Methadone Initiation and Dosing
Ninety-seven infants met the inclusion criteria for this study. Therefore, we recorded data from 62 male and 35 female infants diagnosed with NAS; however, for some of the parameters, we could only collect data from less patients as some data points were missing. There were no differences in the baseline characteristics between male and female infants. For example, birth weight, length, gestational age and total duration of treatment were not significantly different between genders. There were no differences in the mean NAS score throughout treatment for oral methadone between male and female infants (data not reported). However, there were differences in the percentage of scores recorded for specific individual NAS symptoms used to record Finnegan scores. We found that female infants suffered from diarrhea, excessive sucking, tremors when disturbed, sleep disturbances, and crying significantly greater than male infants. However, male infants had significantly greater hyperactive Moro reflex and nasal stuffiness compared with female infants.
We found that female (N = 9) infants had less total methadone administered at 3.32 mg/kg compared with male (N = 29) infants at 3.35 mg/kg during the 7-day postbirth period assessed. This difference in total methadone administered (mg/kg) may indicate that male infants may have needed greater methadone before NAS scores reduced, and thus methadone levels adjusted accordingly. Another important parameter we analyzed was the number of hours before the first dose of methadone was administered. We have found that it took an average 56.63 ± 5.49 hours before male infants received their first dose of methadone following diagnosis with NAS. For female infants, it took 49.76 ± 4.19 hours before they received their first dose of methadone. Head circumferance (HC) (cm) at birth and discharge was significantly different; at birth, the HC was greater in female infants compared with male infants (P = .003), but at discharge, the HC of the male infants was greater when compared with the female infants (P = .035).
Discussion
Our retrospective review of 97 (62 males and 35 females) infants did not show differences in weight gain, length, and HC between genders. Differences were detected in the percentage of scores recorded for specific individual NAS symptoms. We found that female infants suffered from diarrhea, excessive sucking, tremors when disturbed, sleep disturbances, and crying greater than male infants. We also found differences for methadone initiation time (hours) and duration (days) of methadone between genders. Male infants had a greater methadone initiation time compared with female infants, but this time was comparably the same for both genders before the first dose of methadone was administered. Female infants also received less methadone (mg/kg) than male infants during the 7-day treatment period assessed.
A significant limitation of this study is the small sample size, as it may limit the generalization of the findings. Another limitation is that the oral methadone with its long plasma half-life of 16 to 25 hours in neonates (gestational age 34-43 weeks) may have limited the initial control of NAS symptoms and thus delayed weaning. 11 However, conflicting results have been reported that show that the mean elimination half-life of 41 hours, which indicates that neonates have slower plasma clearance of methadone. 12 Both studies, however, were complicated by unreported maternal ingestion of methadone, exposure to other drugs of abuse during pregnancy, and variable intervals between the last dose of methadone and delivery. The greatest difference between male and female genders was in the type of NAS symptoms experienced over the 7-day period of this study. The differences in NAS symptoms could be due to several factors. For example, the difference in sample size, the type of drugs being taken by the mothers during pregnancy, and at what stage of pregnancy could all affect the symptoms experienced by the infants. The most interesting finding regarding differences in NAS symptoms was that the female infants had 67.35% of their symptoms associated with the autonomic nervous system compared with 20.42% for the male infants. For example, we found that the female infants had greater excessive sucking, tremors when disturbed, sleep disturbances, and crying. Furthermore, detailed studies are warranted to elucidate the impact of polysubstance abuse on symptoms associated with NAS as well as the impact of currently Food and Drug Administration–approved treatments used to treat pregnant females with substance abuse disorders such as Suboxone on NAS symptoms.
Conclusion
More studies are needed to assess the short- and long-term effects of antenatal drug abuse. Future studies would include developmental follow-up assessments of the child at different ages and compare these records with the type of opioid (eg, methadone vs morphine vs buprenorphine) administered to the child to control their NAS symptoms at birth. A more detailed understanding of the short-term (<5 years old) and long-term (5-18 years old) developmental effects of NAS are much needed; however, we also need to consider the effects of treatment on these children.
Footnotes
Acknowledgements
We would like to thank all the students who contributed to this project and staff at the neonatal intensive care unit and neonatal therapeutics unit at the Cabell Huntington Hospital in Huntington, West Virginia.
Authors’ Note
Any underlying research materials used to collect these data can be accessed through email to the corresponding author.
Author Contributions
SS: Contributed to conception and design; contributed to analysis; drafted the manuscript; critically revised the manuscript; gave final approval.
TF: Contributed to conception and design; contributed to analysis; drafted the manuscript.
KH: Contributed to analysis.
CT: Contributed to conception and design; contributed to analysis.
JC: Contributed to analysis.
SM: Contributed to conception and design; contributed to analysis; drafted the manuscript; critically revised the manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.