
Abstract
This study examines relationships between adverse childhood experiences (ACEs) and adolescent health indicators among a sample of 8th, 9th, and 11th graders participating in the 2016 Minnesota Student Survey. Logistic regression was used to determine whether 10 types of ACEs were associated with health indicators that may link to health in adulthood, including self-rated health, body mass index (BMI), sleep duration, and dietary and physical activity participation after adjustment for demographic covariates. Individual and cumulative ACEs measures were significantly associated with adverse health indicators, including poorer self-rated health, increased odds of BMI ≥85% and frequent fast food intake, and reduced odds of adequate sleep duration, daily fruit intake, and physical activity participation on most days of the week. Findings advocate screening for ACEs as a means to inform anticipatory guidance strategies and to support development of care models that are relevant and responsive to youth and family needs.
Keywords
Introduction
Evidence continues to mount linking experiences of adversity in childhood to poor health in adulthood. In the original Adverse Childhood Experiences Study, Felitti and colleagues correlated retrospective reports of childhood abuse, neglect, and household dysfunction to the leading causes of morbidity and mortality for US adults, including heart disease, cerebrovascular disease, chronic lung disease, and cancer. 1 A strong and graded relationship is observed between adverse childhood experiences (ACEs) and chronic conditions in adulthood,2-4 and major risk factors for chronic disease, including smoking, substance use, and obesity.5-8 Using data from the original ACEs Study, Brown and colleagues found that people exposed to multiple types of ACEs, 6 or more, died nearly 20 years earlier than participants not exposed to ACEs. 9
Early initiation of risk behaviors as a means of coping with stress is proposed as an important factor linking ACEs to poor health in adulthood.1,5,6,10 Beyond physical and emotional threat posed by involvement in risk behaviors, research now links ongoing and unmitigated childhood adversity to permanent alterations in brain architecture, gene expression, immune status, and cardiometabolic function.11-14
Despite the growing literature documenting links between ACEs and adult health, few large and population-based studies have examined the more proximate link between ACEs and health in adolescence, as an intermediate point in the progression from child context to later adult health. Of the studies available where youth are interviewed, abuse, neglect, household dysfunction, and violence exposure are linked to cigarette, alcohol and other substance use, symptoms of depressed mood, self-injury and suicidality, elevated body mass index (BMI), and poor self-perceptions of health.15-17
The growing evidence of an enduring link between childhood adversity and poor health later in life has prompted recommendations to screen for ACEs in pediatric clinical settings as a means to aid intervention and circumvent the impact of toxic stress on healthy youth development. 18 Despite recommendations to screen for ACEs, results from a recent national survey of pediatricians suggest that almost one third of providers are usually not asking about ACEs. 19 Reasons for differences in ACEs screening practices in the clinical setting are likely many; however, work demonstrating relationships between ACEs and a broader range of health outcomes in adolescence may assist in establishing ACEs screening as critical to providing relevant anticipatory guidance and necessary support to youth and families. Link of experiences of adversity in childhood to adolescent health indicators and potential markers for future health may provide additional evidence marking a path by which ACEs relate to adult health via diverse mechanisms, and garner support for the development of care models that incorporate screening for ACEs as part of routine practice.
The purpose of this study was to examine relationships between ACEs and current health measures in a large, population-based survey of youth. Health measures, including self-rated health, BMI, sleep duration, dietary intake, and physical activity, are representative of indicators that if unhealthy early in life and persistent in poor quality portend worse health for individuals in adulthood. We sought to answer 2 questions: (1) How do ACEs relate to current adolescent health as measured by self-rated health, BMI, meeting minimum recommended sleep time, past week fruit and fast food consumption, and past week physical activity participation? (2) Are there specific types of ACEs that differentially correlate with adolescent health indicators measured in this study? We hypothesized that ACEs, using individual and cumulative analytic approaches, would be linked to outcomes reflecting worse current health and risk for poor future health, and that food insecurity would demonstrate especially strong links to health indicators for youth.20-22
Methods
Study Design and Population
The current study is a secondary data analysis using survey responses from 8th, 9th, and 11th grade students participating in the 2016 Minnesota Student Survey (MSS), N = 126 868. The MSS is an anonymous, population-based study of youth behaviors, perceptions, school climate, and home and community experiences for students attending regular public schools, charter schools, tribal schools, and nonpublic schools throughout the state of Minnesota. Survey design and administration is a collaboration between local schools and 4 state agencies, the Minnesota Departments of Education, Health, Human Services, and Public Safety. The survey is delivered in the school setting during 1 class period every 3 years; schools determine the method of administration, paper and pencil or computer.
School district and student participation in the MSS is voluntary. In 2016, 85.5% of school districts participated, which included 73% of all 8th graders, 71% of all 9th graders, and 61% of all 11th graders. For participating districts, parents are notified of their right to examine survey content and to decline to have their child participate prior to survey administration. Students provide assent for participation. Additional information concerning survey methodology and data management are provided elsewhere.23,24
The research was conducted in accord with prevailing ethical principles. The present study was deemed exempt from review by the overseeing university Human Subjects Institutional Review Board. Data were made available through the Minnesota Center for Health Statistics, Minnesota Department of Health, after completion of a data user agreement and request form.
Measures
Findings from the Adverse Childhood Experiences Study1,25 and evidence-based guidelines provided by the American Academy of Pediatrics (AAP)26,27 informed the identification of 10 questions from the MSS as representative of types of ACEs. The 10 questions were organized into 2 major categories (household dysfunction, 4 questions; and abuse, 4 questions), with 2 questions designed to represent types of economic hardship, food insecurity, and housing instability or homelessness 28 (Table 1). Adverse experiences were dichotomized to reflect any exposure versus no exposure. Adverse experiences scores were created based on category count and a summary count to indicate the range of exposures students reported (score range 0 [no exposures] to 10 [exposed to all forms of adversity]; Table 1).
Questions for Adverse Childhood Experiences.

Health outcomes included in the analysis reflect thoughtful review of public health and medical literatures, including clinical and technical reports and recommendations from the AAP, and available MSS questionnaire content. Outcomes representing indicators of future morbidity and mortality in adulthood include self-rated health and BMI. Self-rated health is an ordinal measure of student perceived health from poor to excellent; it is a valid measure in adolescent populations 29 and is linked to morbidity and mortality in adulthood.30-32 In the current study, self-rated health is dichotomized to excellent, very good, and good versus fair and poor.15,17 BMI is a dichotomous measure corresponding to BMI ≥85% versus not. Risk factors for disordered metabolism with implications for future health (outside of BMI) include sleep duration, fruit intake (excluding fruit juice), physical activity, and fast food intake. Sleep duration is a dichotomous variable based on respondent report of how many hours of sleep he/she gets in a typical school night, dichotomized to reflect ≥8 hours of sleep (recommended for the participant age groups) versus <8 hours. 33 Fruit intake is a dichotomous variable based on recall of number of times fruit was eaten in the past 7 days, dichotomized to ≥2 servings of fruit/day (minimum amount recommended for teens to be combined with vegetable intake) versus <2 servings/day. 34 Physical activity is based on student report of the number of days he/she was physically active for at least 60 minutes during the last 7 days, dichotomized to 5 to 7 days (corresponding to most days of the week) versus <5 days. Fast food intake is measured in 2 ways: (1) number of times fast food was eaten in the last 7 days, dichotomized to ≥3 times versus < 3 times; and (2) fast food intake at least daily versus less than daily in the last 7 days.
Demographic variables included as covariates in multivariate analyses were age, grade (potentially reflecting differential physical activity opportunities during the school day), biological sex, race/ethnicity, family structure, receipt of free or reduced-price lunch (proxy for income; representing family income <185% of the poverty level), 28 and region (potentially representing regional differences in access to food and activity outlets). Age is a continuous variable. Grade is defined as 8th, 9th, or 11th grade. Biological sex is students’ self-identification as male or female. Race/ethnic categories reflect students’ identification based on available categories in the MSS: American Indian non-Hispanic, Asian American non-Hispanic, black non-Hispanic, Pacific Islander non-Hispanic, white non-Hispanic, multiple races non-Hispanic, and Hispanic. Family structure describes youth living with 2 biological or adoptive parents versus all other types of family units. Youth reported “yes” or “no” as to whether or not they received free or reduced-price lunch. Region represents the 7-county Twin Cities metro area versus greater Minnesota.
Data Analysis
Frequency calculations were used to identify characteristics of the sample, including assessment of demographic descriptors and occurrence of ACEs and health outcomes. Correlations (phi coefficient) and percent overlap between food insecurity, housing instability, and receipt of free or reduced-price lunch were calculated to ensure measurement of separate constructs (correlation = 0.12-0.14; % overlap 8.1% to 8.8%). Multivariate logistic regression was conducted to determine if the occurrence of each type of ACE was significantly associated with student health outcomes after adjustment for covariates. To assess the potential for cumulative impact of multiple adverse experiences,1,25 the number of adverse experiences as a single ordinal variable (0, 1, 2, 3, or ≥4) was entered into separate logistic regression models for each health outcome, adjusting for covariates. In addition, adverse experiences scores, by category and total, were entered into logistic regression models with adjustment for covariates to test for a dose-response relationship between each adverse experience score and each health outcome.1,25,35 All analyses were performed using Stata 12 SE (Stata Corp, College Station, TX).
Results
Characteristics of the Study Sample
The mean age of participating youth was 14.8 years (range 12-19 years). Equal proportions of youth were in the 8th and 9th grades (~35%), with just under 30% of the sample in the 11th grade (28.8%). Half of the sample was female (49.6%). Most youth self-identified as white, non-Hispanic (69.2%); smaller proportions of youth self-identified as Hispanic (9.6%), multiple races, non-Hispanic (7.5%), black, non-Hispanic (6.4%), Asian American, non-Hispanic (6.0%), American Indian, non-Hispanic (1.2%), and Pacific Islander, non-Hispanic (0.2%). The majority of students lived with 2 biological or 2 adoptive parents (70.1%). More than a quarter of youth received free or reduced-price lunch (28.5%). Just under half of youth lived outside of the Twin Cities metro area (46.4%).
Experiences of adversity were reported by more than one third of 8th, 9th, and 11th grade participants, as defined by the categories for this study (38.5%). Nearly 1 in 5 students reported 1 ACE (19.5%); 9.0% reported 2 ACEs; and close to equal proportions reported 3 and ≥4 ACEs (4.9% and 5.1%, respectively). Having a parent/guardian who had ever been in jail/prison was the most frequently reported ACE (16.5%), followed by verbal/emotional abuse (13.6%), physical abuse (11.8%), and living with someone who drinks too much alcohol (9.8%). Witness of violence by adults (6.5%), housing instability (5.5%), living with someone who uses illegal drugs or abuses prescription drugs (4.6%), and food insecurity (4.6%) were reported by smaller proportions of youth.
Multiple covariates were significantly associated with experience of adversity. Compared to youth self-identifying as white, youth self-identifying as American Indian (odds ratio [OR]: 1.84, 95% confidence interval [CI]: 1.63-2.08), Asian American (OR: 1.11, 95% CI: 1.05-1.18), Pacific Islander (OR: 1.87, 95% CI: 1.35-2.59), of multiple races (OR: 1.79, 95% CI: 1.71-1.89), and Hispanic (OR: 1.26, 95% CI: 1.21-1.32) had greater odds of reporting any history of ACE. Greater odds of reporting any history of ACE was also associated with receipt of free or reduced-price lunch (OR: 2.04, 95% CI: 1.97-2.10). Living with 2 biological or adoptive parents (OR: 0.39, 95% CI: 0.38-0.41) and living in the Twin Cities metro area (OR: 0.87, 95% CI: 0.85-0.90) were associated with reduced odds of reporting any history of ACE.
Most participants reported good or better health (90.7%). About 1 in 4 youth had a BMI ≥85% (24.1%). Less than half of youth got the recommended number of hours of sleep on a typical school night (37.7%). Less than one third of youth consumed at least 2 servings of fruit/day in the last week (29.2%). Just over half of youth participated in at least 60 minutes of physical activity on 5 to 7 days in the last week (51.3%). One in 8 youth ate fast food on 3 or more days in the last week (12.5%), with fewer youth consuming fast food at least daily in the last week (5.7%).
Youth Self-Rated Health and Body Mass Index, Relationships With ACEs
Experience of adversity was significantly associated with 2 potential markers for morbidity in adulthood, youth self-rated health and BMI. Individual ACEs were linked to 41% (OR: 0.59, 95% CI: 0.56-0.62) to 63% (OR: 0.37, 95% CI: 0.35-0.39) reduced odds of youth reporting good or better self-rated health (Table 2). The relationship between food insecurity and youth reduced odds of reporting at least good self-rated health was similar in magnitude to youth experiences of types of abuse. For each additional ACE identified (range 0-10), the odds of youth reporting at least good self-rated health was reduced by 27% (OR: 0.73, 95% CI: 0.72-0.74). All experiences of adversity were associated with increased odds of youth having a BMI ≥85%, individually and cumulatively (Table 2). Compared to youth reporting no ACEs, experience of ≥4 ACEs was associated with 60% increased odds of having a BMI ≥85% (OR: 1.60, 95% CI: 1.50-1.70). For each additional ACE identified (range 0-10), the odds of youth having a BMI ≥85% increased by just over 10% (OR: 1.11, 95% CI: 1.10-1.13).
Self-Rated Health, Body Mass Index, and Sleep Duration According to Adverse Childhood Experiences*.

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Respondent reports at least good self-rated health.
Respondent has body mass index ≥85%.
Respondent reports getting ≥8 hours of sleep during a typical school night.
Odds ratios adjusted for age, sex, grade, race/ethnicity, family structure, receipt of free or reduced-price lunch, and region.
Abuse score (range 0-4).
Household dysfunction score (range 0-4).
Food insecurity–Housing instability score (range 0-2).
Total adverse childhood experiences score (range 0-10).
All P values <.001.
Sleep, Dietary Intake, and Physical Activity, Relationship With ACEs
Individual ACEs were linked to 14% (OR: 0.86, 95% CI: 0.81-0.91) to 54% (OR: 0.46, 95% CI: 0.43-0.49) reduced odds of youth reporting at least 8 hours of sleep on a typical school night (Table 2). Food insecurity had the strongest relationship with reduced sleep compared to other ACEs, including all experiences of abuse and household dysfunction. For each additional ACE identified (range 0-10), the odds of youth getting recommended sleep was reduced by 22% (OR: 0.78, 95% CI: 0.77-0.79).
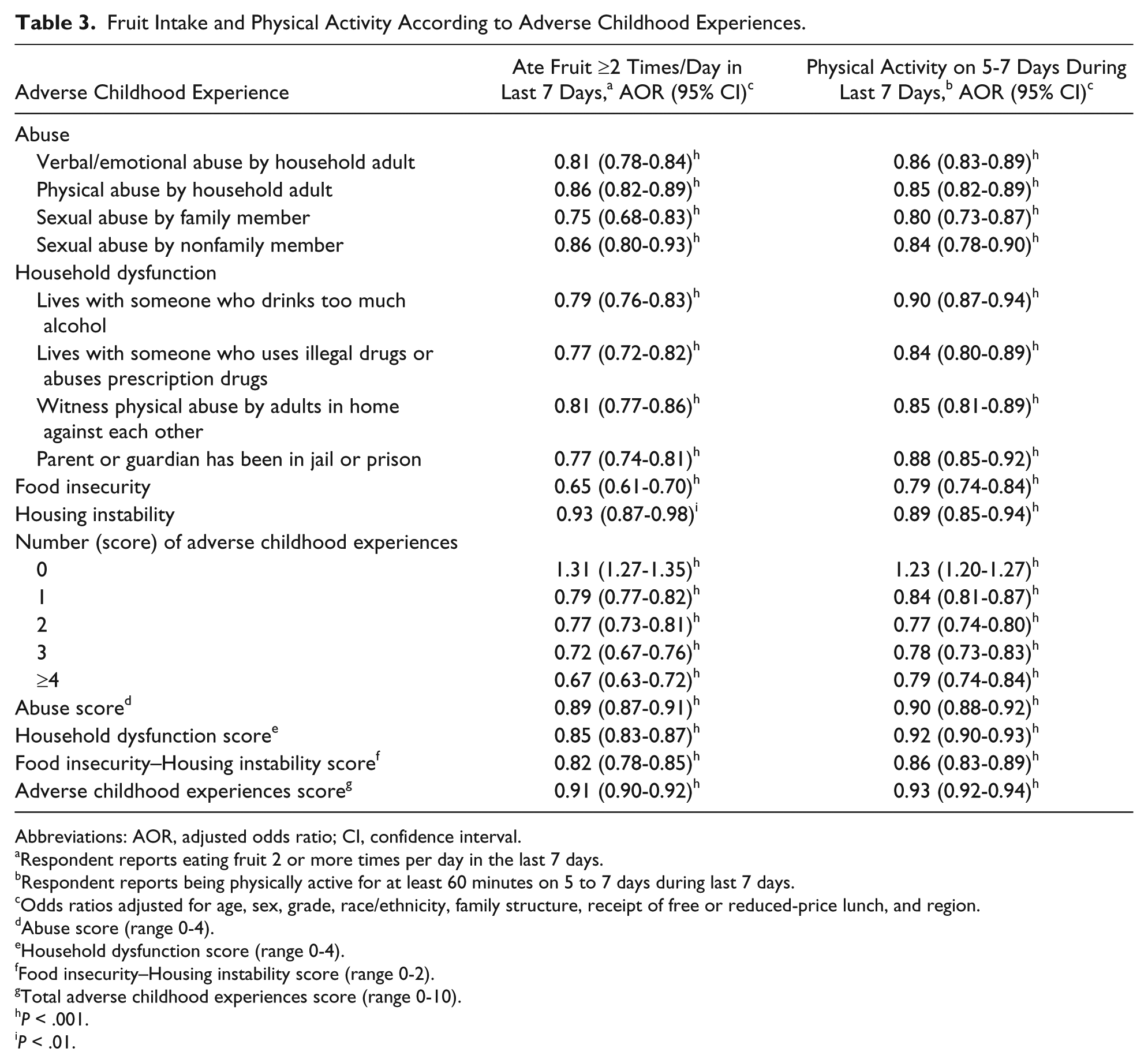
Youth experiences of adversity were associated with reduced odds of participating in healthy behaviors such as consuming fruits daily in the last week and being physically active in the last week (Table 3). Relationships between food insecurity and reduced odds of consuming fruit ≥2 times/day in the last week (OR: 0.65, 95% CI: 0.61-0.70), and reduced odds of being physically active on 5 to 7 days in the last week (OR: 0.79, 95% CI: 0.74-0.84) were of similar or greater degree than experiences of abuse and household dysfunction and reduced odds of participating in these healthy behaviors. For each 1 point increase in the total ACE score (range 0-10), the odds of consuming fruit ≥2 times/day in the last week (OR: 0.91, 95% CI: 0.90-0.92) and being physically active on 5 to 7 days in the last week (OR: 0.93, 95% CI: 0.92-0.94) was reduced by 7% to 9%.
Fruit Intake and Physical Activity According to Adverse Childhood Experiences.
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Respondent reports eating fruit 2 or more times per day in the last 7 days.
Respondent reports being physically active for at least 60 minutes on 5 to 7 days during last 7 days.
cOdds ratios adjusted for age, sex, grade, race/ethnicity, family structure, receipt of free or reduced-price lunch, and region.
Abuse score (range 0-4).
Household dysfunction score (range 0-4).
Food insecurity–Housing instability score (range 0-2).
Total adverse childhood experiences score (range 0-10).
P < .001.
P < .01.
All experiences of adversity were associated with increased odds of youth fast food consumption, individually and cumulatively (Table 4). The adjusted odds ratios were highest for the association of food insecurity (≥3 times in the last 7 days OR: 1.89, 95% CI: 1.76-2.02; at least daily in the last 7 days OR: 1.81, 95% CI: 1.70-1.93) and housing instability (≥3 times in the last 7 days OR: 1.83, 95% CI: 1.67-2.00; at least daily in the last 7 days OR: 2.01, 95% CI: 1.85-2.19) with both measures for fast food intake as compared to all other ACEs. Compared to youth reporting no ACEs, experience of ≥4 ACEs was associated with more than double the odds of fast food intake in the last week (≥3 times in the last 7 days OR: 2.28, 95% CI: 2.13-2.45; at least daily in last 7 days OR: 2.23, 95% CI: 2.03-2.45).
Fast Food Intake According to Adverse Childhood Experiences*.

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Respondent reports eating from fast food restaurant, including carry-out or delivery.
Odds ratios adjusted for age, sex, grade, race/ethnicity, family structure, receipt of free or reduced-price lunch, and region.
Abuse score (range 0-4).
Household dysfunction score (range 0-4).
Food insecurity–Housing instability score (range 0-2).
Total adverse childhood experiences score (range 0-10).
All P values <.001.
Discussion
Summary of Study Findings
The current study provides more evidence for a significant relationship between ACEs exposure and adolescent health and shows examples of potential intermediate steps in the progression from ACEs to adult health. ACEs are significantly related to indicators for poor adolescent health via self-perceptions of health, abnormal BMI, chronic inadequate sleep duration, and health behaviors beyond risk behaviors, including dietary intake (limited daily intake of fruit and frequent fast food consumption), and low physical activity. In all examples, ACEs exhibited a graded and cumulative association with indicators for adverse adolescent health.
Notably, in most analytic models the magnitude of the relationship between food insecurity and adolescent health indicators was similar or greater than the magnitude of the relationship between experiences of neglect and abuse and youth health. Food insecurity has been linked to adverse youth and adult outcomes among low-income populations.21,22 Current findings suggest connections between food insecurity and adverse youth health indicators even with adjustment for demographic characteristics, including a proxy measure for household low-income. In addition, a significant association between experience of household food insecurity and youth weight status was noted, adding to a literature that has inconsistently shown a relationship between food status and youth weight outcomes.36-41 Adolescents reporting experience of having to skip meals in the last 30 days due to their family not having enough money to buy food had just over one third increased odds (34%) of having a BMI ≥85%. In contrast to some of the literature examining relationships between household food condition and youth weight status focused on low-income populations and/or comparing low-income to higher-income families,37,40,42 the positive relationship between food insecurity and adolescents’ odds of having a BMI ≥85% was found with adjustment using a proxy measure for limited household financial resource. This finding suggests the relevance of food insecurity for unhealthy weight status among youth, notwithstanding meeting income guidelines for some supplemental assistance programming.
Study Findings in Broader Context
Looking across available research evaluating relationships between ACEs exposure and youth health outcomes, study findings are congruent with research focused on urban and other targeted groups. For example, in studies of youth who are the focus of investigative reports or youth deemed at risk for maltreatment, child maltreatment is linked to increased risk of any health complaint and illness requiring medical care.43-45 In an urban, clinic population of youth, when compared to an ACE score = 0, youth with an ACE score ≥4 had a 2-fold increase in the odds of having a BMI ≥85%. 46 On a larger scale, among parent respondents in the 2011-2012 National Survey of Children’s Health, parent report of ACEs is linked to parent perception of child poor health and emotional well-being, as well as diagnoses of chronic health conditions, such as obesity.47-49
The health outcomes examined in this study may be particularly sobering when considering the future health of young people. Self-reported health is an established marker for morbidity and mortality in adults,30-32 and it is considered a stable construct during adolescence that is significantly associated with chronic health conditions, emotional problems, deterioration in health, and health risk behaviors.29,50 BMI ≥85% in adolescence (metabolic disruptor) 51 is associated with significantly increased odds of obesity in adulthood and risk for a range of chronic conditions in adulthood, including hypertension, heart disease, kidney disease, diabetes, and cancer.52-56 Chronic inadequate sleep duration (metabolic disruptor) 57 likely also has impact on chronic disease development. A recent study identifies an inverse association between sleep duration and type 2 diabetes risk markers in children. 58 Poor-quality nutrient intake in adolescence tracks into adulthood and risk for future chronic disease.59,60 Since patterns of behavior initiated in adolescence, such as physical activity participation and fast food intake, are likely to be carried into adulthood, adult-onset disease is often due to the cumulative effect of ongoing unhealthy behavior beginning early in the life course.61,62
Implications for Practice
Study findings make a strong argument for incorporation of ACEs screening into routine pediatric and adolescent practice as a means to identify youth and family needs, and to intervene to provide connections to available resources. Beyond significant relationships identified between ACEs and odds of adolescents having a BMI ≥85%, 3 health indicators placing adolescents as risk for future obesity and diabetes are linked to individual and cumulative measures for ACEs: inadequate sleep duration, poor dietary intake, and insufficient participation in physical activity.51,57 It is important to note that processes evident in adolescence do not predetermine youths’ potential to achieve health and well-being in adulthood; yet it is necessary for steps to be put in place to facilitate reversal of circumstances placing one at risk for future disease and disability.
Screening for ACEs has the potential to render anticipatory guidance strategies more relevant and responsive to youth and family context. For example, knowledge of challenges to access of fresh, high-quality food has implications for the type of counseling and necessary intervention likely to be supportive and effectual in helping youth make progress toward achieving a healthy weight goal. Cautions about the dangers of not getting enough sleep or regular exercise may ring hollow for families struggling to find consistent and safe housing.
Tools are available to providers and clinic staff to assist with the process of incorporating ACEs screening as part of routine and on-going health care. The AAP offers guidance and a training toolkit to support health professionals in the development of models for addressing ACEs and supporting youth and family resilience in the medical home environment.18,63 The Center for Youth Wellness is also a resource for examples of ACEs screens available to clinics with registration. 64
Identification and integration of therapeutic responses to screening results are critical. Care contexts that include partnerships with community-based organizations offer promise in helping to connect youth and families to resources in support of health and well-being. Emerging research suggests that systematic screening for social determinants of health, including types of adverse experiences, results in families receiving more community resources. 65 Similarly, addressing basic needs during the delivery of pediatric primary care, via screening and in-person resource service navigation or provider referral with clinic staff follow-up on resource contact, has been shown to be feasible and effective, resulting in connecting families to more resources and improving mother’s perceptions of child health.65,66 Design strategies and tools for successful integration of social needs screening and intervention into clinic workflow are available. 67 Expansion of the medical home to include full partnerships with community organizations may facilitate the goal of creating health neighborhoods; 68 here the clinic context becomes part of a larger framework in support of individual, family, and public health. Having a multidisciplinary and team-based approach to address ACEs in the clinic environment, inclusive of nursing and home visiting outreach, behavioral and mental health services, and integrative health therapies, may better facilitate success in mitigating and preventing development of new experiences of adversity. 64
More work remains in the development of ACEs screening and intervention efforts. Identification of reimbursement structures to support investment in screening is needed. 69 Collaboration with family and community partners to identify acceptable ways of asking about adversity and modeling relevant responses to a range of screening results is essential.70,71
Study Strengths and Limitations
This study has some strengths and limitations. Findings are drawn from a large, population-based sample of youth. Measures for ACEs include conventional concepts, such as examples of abuse, neglect, and household dysfunction, as well as experiences signifying dimensions of extreme socioeconomic hardship, namely, food insecurity and housing instability. Study findings demonstrate relationships between ACEs and health indicators in adolescence, beyond risk behaviors, that if persistent, foretell future morbidity and potentially early mortality in adulthood.
Survey data are cross-sectional and located within a large Midwestern state. As such, causality cannot be established and findings may not be generalizable to populations of youth living in other regions of the United States. Even with the range of questions used to address ACEs (10 representative questions), in some cases, survey length restrictions necessitated usage of a single question to measure a type of ACE. Because of limited specificity used in the question asking about vegetable intake, the full relationship between ACEs and adolescent fruit and vegetable intake (often linked) could not be explored. Due to the survey structure, determination of length of exposure to ACEs cannot be made, and by extension, the potential relationships between exposure duration and adolescent health outcomes cannot be elucidated with this study. ACEs exposures are based on youth self-report and cannot be verified by administrative record; however, the anonymous nature of the MSS may facilitate more accurate estimation of sensitive topics such as ACEs. Youth self-report of adverse experiences has been found to be reliable and valid in other settings. 72 Measures for the food and activity outcomes are based on 7-day recall, and thus may not represent a typical week; however, giving a limited time frame such as reporting on events “in the last 7 days” may aid more accurate account.
Conclusions
Adverse childhood experiences are related to health indicators in adolescence that if persistent portend increased risk for poor health in adulthood. In particular, the relationship between food insecurity and adverse health outcomes among youth was similar or greater in magnitude to relationships between experiences of abuse and household dysfunction and youth poor health. Study findings provide more evidence for the importance of pediatric providers, support staff, and community resource organizations working together to create care models that identify the best ways to screen for and intervene on ACEs as part of a routine, standard of care.
Footnotes
Acknowledgements
The authors wish to thank the Minnesota Department of Health, Center for Health Statistics, for access to the MSS data. The research reported in this article is solely the responsibility of the authors and does not necessarily reflect the official views of the Minnesota Departments of Education, Health, Human Services, and Public Safety.
Author Contributions
NND: conceptualized the secondary data analysis project, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript.
IWB: informed the analytic design of the research project, and reviewed and revised the manuscript.
All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.