
Abstract
Objectives. We sought to evaluate the admission and hospital risk factors for death in children with diarrhea requiring mechanical ventilation (MV). Methods. This was a retrospective study. We enrolled children aged 0 to 59 months admitted with diarrhea to the intensive care unit of the Dhaka Hospital of International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) between August 2009 and July 2013 and required MV. To evaluate the risk factors for death in MV, we compared the clinical and laboratory characteristics of the children requiring MV. We matched up to the clinical characteristics presented on admission and subsequently developed before MV during hospital stay with the survivors and deaths of children having MV. Results. Among 73 enrolled children, 58 (80%) died. Incidence of death in MV was higher among children having hyperkalemia (P ≤ .001), hypoglycemia (P ≤ .001), and metabolic acidosis (P = .06) on admission and lower in children having tracheal isolates (P ≤ .001) during hospitalization. After adjusting for covariates by using multivariate robust Poisson regression, children with hyperkalemia (incidence ratio = 1.34; P = .03; confidence interval = 1.02-1.76) on admission was the only independent risk factor for death of children with MV. Conclusion. Children with hyperkalemia on admission and subsequently requiring MV were more likely to die compared with those without hyperkalemia.
Introduction
Diarrheal disease is still one of the major causes of death among children under 5 years in lower-middle income countries, despite a 57% decline from 1.2 million deaths in 2000 to 0.5 million in 2015 globally. 1 The burden of death from diarrheal disease is 9% among 5.9 million under-5 deaths globally. 2 In Bangladesh, diarrheal disease accounted for a total of 6% deaths among 119 000 under-5 deaths in 2015. 2
Child death from diarrhea is largely preventable through implementing different strategies—even one death should be considered as too many. 1 Faster progress in preventing diarrhea-related deaths is critical in achieving the Sustainable Development Goal 3. 1 In lower-middle income countries like Bangladesh, children with diarrhea, with or without comorbidities, often develop life-threatening complications that require hospital admission in the intensive care unit (ICU).3,4 A number of children requiring admission in ICU often require mechanical ventilation (MV) mainly because of respiratory failure.5,6 MV is a frequently used and essential life-supporting invasive technology that imitates respiratory physiological function at the time of impending or acute respiratory failure or acute neurological illness.7,8 Although benefits of MV are indisputable in industrialized countries, the invasiveness and the nature of the procedure of MV in developing country setups are often associated with hospital-acquired infections, airway lesions, ventilator-associated pneumonia (VAP), and so on.9,10 Based on different factors, mortality caused by MV may be around 40%.11-13 Patients requiring MV support in the ICU had substantially higher mortality rates when compared with patients without MV support.5,14 We need to understand the risk factors for death in children requiring MV to provide useful guidance in appropriately managing at-risk patients in order to reduce mortality associated with MV. Although a number of studies have reported risk factors for mortality in children requiring MV,11,15,16 to our knowledge there are no published data on the risk factors of death in children also having diarrhea and requiring MV.
The Dhaka Hospital of the International Centre for Diarrheal Disease Research, Bangladesh (icddr,b) treats a number of patients with diarrhea and associated complications. 6 The patients seen in this facility often require admission to the ICU and may necessitate MV with fatal outcome. 6 A recent study in Dhaka Hospital identified 29/91 (32%) deaths among children under 5 years while admitted in the ICU with diarrhea and respiratory distress; among them 18/91 (20%) required MV and 13/18 (72%) died while under MV. 4 Another study in same hospital setting reported 80% of patients who were admitted to the ICU with diarrhea and associated complications and used MV died; this percentage of deaths from MV was higher than those reported in other studies,5,11 although overall under-5 deaths in the same ICU was 11%. 17 To prevent such deaths from MV, it is imperative to initiate prompt treatment through the identification of patients at risk of death while on MV. Thus, we aimed to evaluate the clinical predictors for death in children requiring MV in the ICU.
Materials and Methods
Study Site
We collected data from the ICU of Dhaka Hospital of icddr,b, which is the largest diarrheal disease hospital in the world treating around 150 000 patients annually. Each year, the ICU of this hospital manages around 1000 children under 5 years of age. The comprehensive description of the study site has been described elsewhere. 6
Study Design
This is a retrospective observational cohort study. In this study, we enrolled children aged 0 to 59 months admitted with diarrhea to the ICU of Dhaka Hospital of icddr,b between August 2009 and July 2013 and required MV. To evaluate the risk factors for death of children with diarrhea while under MV, we compared the clinical and laboratory characteristics of the children requiring MV. We match up to the clinical characteristics presented on admission and subsequently developed before MV during hospital stay with the survivors and deaths while under MV.
Patient Management
Children under MV in the ICU received pressure-synchronized intermittent mandatory ventilation with a fraction of inspired oxygen of 100%, with a subsequent gradual titration from 30% to 40%. 5 The other pediatric ventilator support was adequate and other treatment support the study children received while under MV in the ICU has been described elsewhere. 6
Measurements
To obtain the relevant study information, we developed the case report form, pretested and finalized. We included the following characteristics: demographic information on admission age, sex, vaccination, and breastfeeding history from the neonatal period; the clinical features of dehydration in different severity (no, some, or severe) defined by the World Health Organization method. 18 Severe malnutrition was defined as the child having severe underweight (weight for age Z score < −3 of median of the World Health Organization growth standard), or nutritional edema. 19 Other analyzed characteristics were urinary tract infection, stool isolates on admission, pneumonia, septic shock, hypoglycemia (random blood sugar <3.0 mmol/L), bacteremia (bacterial isolate from a single blood sample culture), hypokalemia (serum potassium <3.5 mmol/L), hyperkalemia (serum potassium >5.5 mmol/L), hyponatremia (serum sodium <130.0 mmol/L), hypernatremia (serum sodium >150.0 mmol/L), increased serum creatinine level (>65.0 µmol/L), and metabolic acidosis (pH <7.2 and bicarbonate <15.0 mmol/L in arterial blood gas analysis) both on admission and during hospitalization, respiratory acidosis (pH <7.2 and partial pressure of carbon dioxide >45.0 mm mercury in arterial blood gas analysis), and tracheal isolates (bacterial isolate from a tracheal aspirate sample culture) during hospitalization. 5 Acute kidney injury (AKI) was defined following age-specific decreased glomerular filtration rate using the Schwartz formula.20,21 Septic shock was defined as severe sepsis unresponsive to fluid resuscitation. Severe sepsis was defined as tachycardia plus hypothermia (≤35.0°C) or hyperthermia (≥38.5°C) or an abnormal white blood cell count plus the presence of infection with poor peripheral perfusion (mean arterial pressure ≤50 mm Hg and/or absent peripheral pulses or capillary refilling time >3 seconds) in the absence of dehydration.5,6
Data Analysis
We calculated the incidence of death during follow-up while under MV among children under 5 years of age admitted in the ICU with diarrhea. To identify the risk factors of death while under MV in children, we calculated the incidence ratio (IR) of deaths with 95% confidence intervals (CIs) and P value by using robust Poisson regression for each variable and then multivariate Poisson regression was used to adjust the effect of other covariates, which was significantly associated (P < .05) with death incidence to calculate the adjusted IR of death. All data were entered into SPSS for Windows version 20.0 (SPSS Inc, Chicago, IL), and data process and analysis was performed with STATA version 13.
Ethics Statement
The data used in this study were retrieved from the case records of patients of the Dhaka Hospital and entered in an anonymized and de-identified manner prior to analysis. The aim was to improve the hospital patients’ quality of care. The study did not involve any interviews with patients or their caregivers. No authors had any access to patient-identifying information. An ethical approval waiver was completed for publication by the Ethical Review Committee of Dhaka Hospital.
Results
Our personal database identified a total of 73 children under 5 years of age with diarrhea requiring MV during the study period and among them 58 (80%) died. The incidence of death while under MV among children who had hyperkalemia on admission was 33% higher than the children who had no hyperkalemia (IR = 1.33; 95% CI = 1.15-1.55; P ≤ .001; Table 1). Hyperkalemia on admission was 65% higher among children having AKI on admission compared with those who did not have AKI (IR = 1.65; P = .09; 95% CI = 0.92-2.97).
Admission Characteristics and Incidence of Death in Children Aged 0 to 59 Months With Diarrhea While Under Mechanical Ventilation (N = 73).
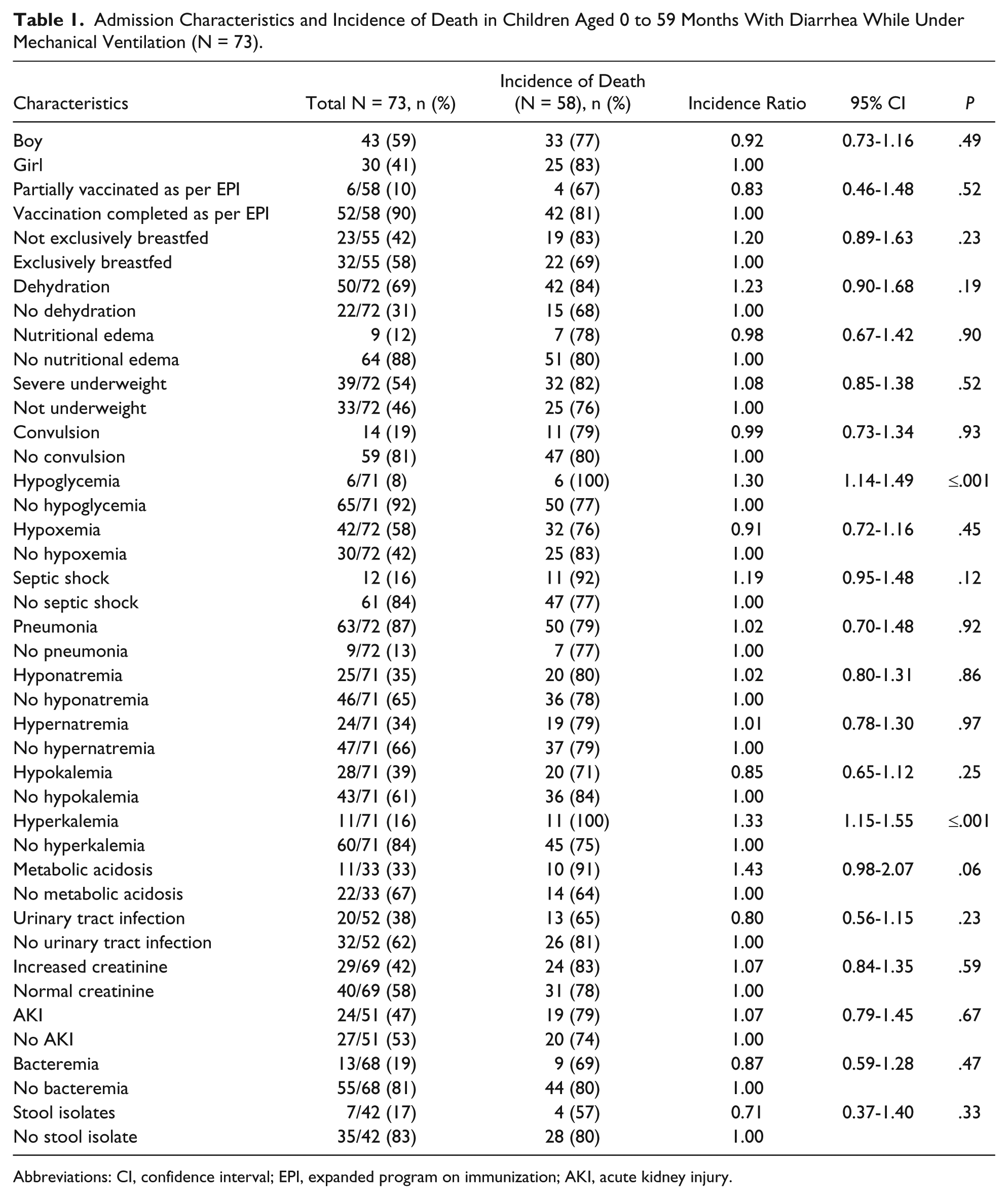
Abbreviations: CI, confidence interval; EPI, expanded program on immunization; AKI, acute kidney injury.
In univariate analysis, death while under MV was higher in hypoglycemia (IR = 1.30; 95% CI = 1.14-1.49; P ≤ .001) and metabolic acidosis (IR = 1.43; 95% CI = 1.15-1.55; P ≤ .06) on admission (Table 1). On the contrary, incidence of death while under MV was 32% lower in children who had tracheal isolates (IR = 0.68; 95% CI = 0.53-0.86; P ≤ .001; Table 2). After adjusting for potential other covariates by using multivariate robust Poisson regression, children with hyperkalemia (IR = 1.34; CI = 1.02-1.76; P ≤ .03) on admission remained as the only independent risk factor for death while under MV (Table 3).
Characteristics During Hospitalization and Incidence of Death in Children Aged 0 to 59 Months With Diarrhea While Under Mechanical Ventilation (N = 73).
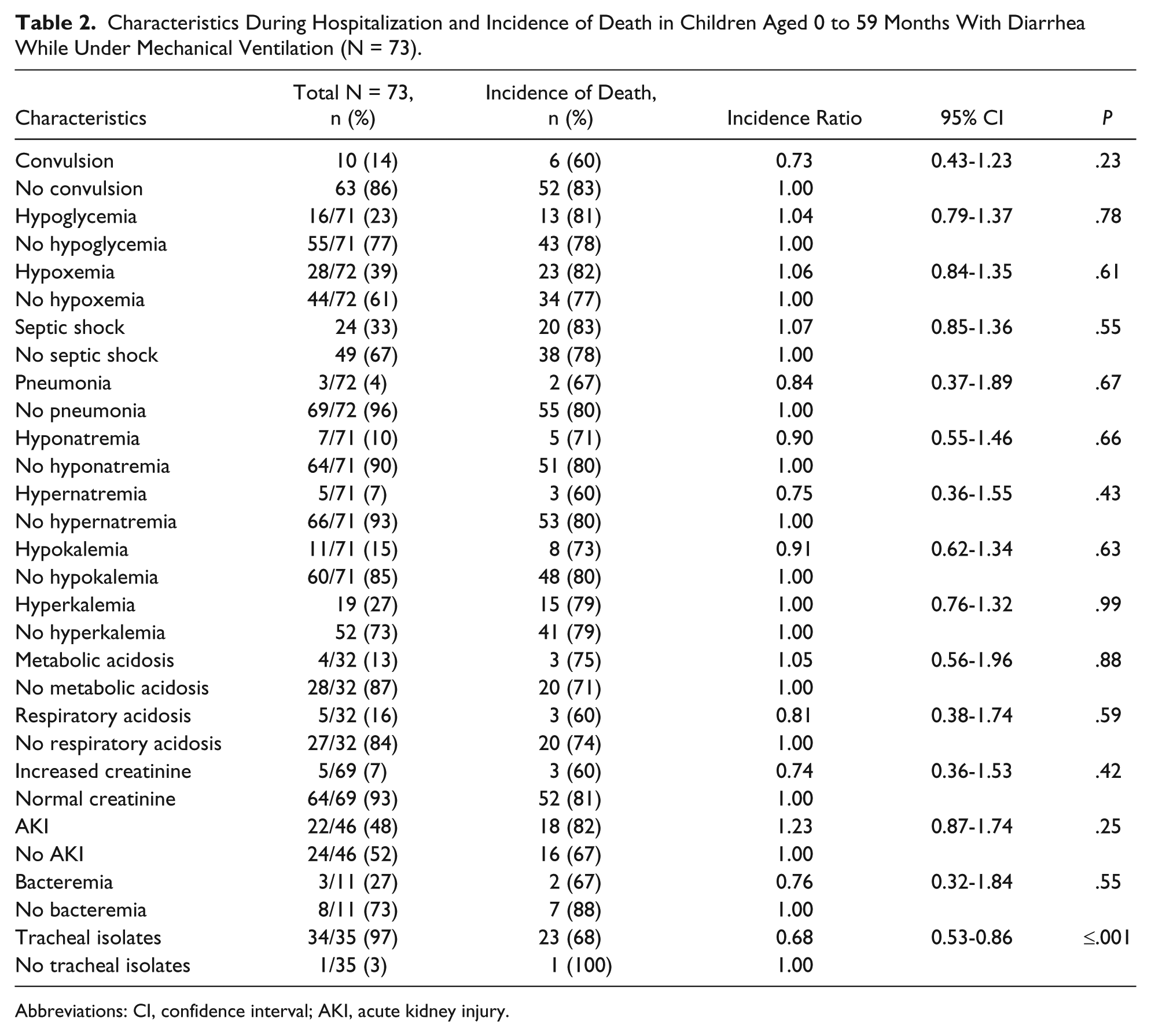
Abbreviations: CI, confidence interval; AKI, acute kidney injury.
Results of Poisson Regression to Explore the Independent Risk Factor of Death While Under Mechanical Ventilation in Children Aged 0 to 59 Months With Diarrhea on Admission.

Discussion
To our knowledge this is the only study that evaluated the risk factors for death in children also having diarrhea and who required MV in the ICU in a developing country. Our study identified hyperkalemia on admission as an independent risk factor for death in children under 5 years of age hospitalized for diarrhea and subsequently required MV in the ICU. In our study, death while under MV was more among children having both hyperkalemia and AKI compared with those without AKI and the findings are in accordance with previous observations. 22 Potentially higher incidence of metabolic acidosis in mechanically ventilated children who died had an impact on our observation of hyperkalemia as an independent risk factor for deaths in our study children. Hyperkalemia may lead to ventricular fibrillation followed by rapid death 23 even under ventricular support. Therefore, avoiding the wasting of golden time in getting the serum electrolytes report from the clinical laboratory; initiation of prompt treatment of hyperkalemia by treating clinicians through a combination of history, physical examination, and electrocardiography findings; or alternatively beside rapid electrolyte measurement is critically important. 23 Up to 10% of hospitalized children may have hyperkalemia23,24 while our study reported 16% children with diarrhea while under MV had hyperkalemia on admission and all of them died while under MV despite receiving protocolized management of hyperkalemia. 25 This might be because of the fact that the detection of hyperkalemia in these children was late as we had to wait a few hours for receiving the serum electrolytes report, whereas treatment of hyperkalemia demands medical emergency. Thus, we need to underscore the importance of measurement of serum electrolytes in ICU children for early detection of hyperkalemia especially those who requiring MV in order to initiate prompt treatment of hyperkalemia that may help prevent potentially life-threatening ventricular fibrillation and neuromuscular disturbances through shifting potassium into cells, eliminating excess potassium, and thus resolving the underlying disturbance and decrease the risk of death. 23
In univariate analysis, hypoglycemia and metabolic acidosis on admission were observed to have association with death among children while under MV compared with those who did not have hypoglycemia or metabolic acidosis. But these predictors were not found to be significant in Poisson regression analysis after adjusting for hyperkalemia and this might be because of the small sample size. Nevertheless, earlier studies have reported association of hypoglycemia4,26-28 and metabolic acidosis3,28 with death at ICU.
However, tracheal isolates were observed to have protective association for death in children while under MV. This might be due to the impact of treatment of the children while under MV with specific antibiotics based on isolation of bacteria in tracheal aspirates. Although previous study has shown that trachea may be colonized by potential pulmonary pathogens within hours of intubation without causing VAP, 29 another study reported 70% patients with VAP had an isolation of identical bacteria both in tracheal aspirates and lower respiratory tract. 30
Our study limitation was the small sample size with retrospective and missing data, which might have an impact of having our limited clinical predictors of death in children while under MV. Moreover, data generated from a single ICU setting may not be representative of the entire population of hospitalized children under 5 years of age with diarrhea. Due to the lack of documentation in the patients’ chart, we were able to evaluate a small proportion of children for metabolic acidosis, increased creatinine, urinary tract infections, stool isolates, and bacteremia on admission (Table 1), and metabolic acidosis, respiratory acidosis, increased creatinine, bacteremia, and tracheal isolates during hospitalization (Table 2).
Conclusion
In conclusion, the results of our study suggest that hyperkalemia on admission might be an independent risk factor for death among children under 5 years of age hospitalized for diarrhea and requiring MV. Thus, early detection and prompt treatment of hyperkalemia is imperative to mitigate death in children with diarrhea requiring MV in the ICU. Future prospective study in a larger scale and different setting should be conducted to consolidate our study observation.
Footnotes
Acknowledgements
We would like to express our sincere thanks to all physicians, clinical fellows, nurses, members of the feeding team, and cleaners of the hospital for their invaluable support and contribution for patient care and data collection. We would also like to express our gratitude to caregivers/mothers of the study participants for their consent to enroll their children in the study.
Author Contributions
FC: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
PKG: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
KMS: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ASMSBS: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LS: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MS: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
S: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
FA: Contributed to design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MJC: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b) gratefully acknowledges the following donors who provided unrestricted support: Government of the People’s Republic of Bangladesh, Global Affairs Canada, Swedish International Development Cooperation Agency, and the Department for International Development.