
Abstract
Foreign body aspiration (FBA) is a common and lethal accident in the pediatric age group. It requires early recognition and treatment by rigid bronchoscopy to avoid fatal outcomes. Objective. The aim of this study was to study the pattern of FBA in the tracheobronchial tree as well as the success rate of rigid bronchoscopy in children admitted to a single center and to analyze the relationship of the type of foreign body (FB) with patients’ age, presentation, and complications. Methods. A retrospective cross-sectional study of FBA was conducted in children in the Sulaimani/Kurdistan region, Iraq, admitted to the emergency teaching hospital of the University of Sulaimani from January 2014 to March 2016. Result. Data of 83 patients between 6 months and 15 years old were studied. The most affected was the 1- to 5-year-old group. There was a slight female predominance (male to female ratio 0.93:1). The most common FB was sunflower seed (49.4%). History of choking was present in 92.8% of patients; 55.4% had normal air entry, and 37.3% had no added sound on chest auscultation. Normal chest X-ray (CXR) was found in 40% of patients. The most common site was the right bronchial tree (39.8%). Two patients needed mechanical ventilation; both of them died. There was a significant relationship between the type of FB (P = .013, .000, respectively). Conclusion. Medical history is the most important factor for reaching the diagnosis; bronchoscopy is mandatory if choking was witnessed, even if examination and CXR are normal. Organic material causes more local reaction than nonorganic material.
Introduction
Foreign body aspiration (FBA) is a common problem in the pediatric age group and is a potentially life-threatening condition requiring prompt recognition and early management to minimize fatal consequences. 1 It is the fourth most common cause of accidental death for those less than 3 years old. 2 It occurs more commonly among male children with a ratio of 1.5:1 to 2.4:1. 3 Commonly aspirated foreign bodies (FBs) in children include peanuts, seeds, food particles, hardware, and pieces of toys. 4 Nonfood items (eg, coins, paper clips, pins, pen caps) are more commonly aspirated by older children. 5 Sudden onset of coughing and choking are the most common presenting symptoms. 6 The presentation of FBA depends on the degree of airway blockage and the location of the objects as well as the age of the child, the type of object, and the time elapsed since the event. 7 The classic triad of cough, wheeze, and diminished breath sounds is not universally present. 4 The presence of the triad has high specificity (96% to 98%) for the diagnosis of FBA, but the sensitivity is low (27% to 43%). 8 Although it may impact anywhere, more often, these FBs get lodged in the right main bronchus (RMB). This is because the RMB is more in line with the trachea, thereby creating a relatively straight path from the larynx to the bronchus. 9 Chest radiographs are helpful in confirming the presence of airway FBs but cannot be used to exclude the diagnosis because plain chest radiographs are normal in >50% of tracheal FBs and one-fourth of bronchial FBs. More than 75% of airway FBs in children <3 years of age are radiolucent. Indirect radiological signs of radiolucent airway FBs include unilateral hyperinflation, atelectasis, consolidation, and bronchiectasis in delayed presentation. 6 A computed tomography (CT) scan is a possible diagnostic option for patients who are asymptomatic, or symptomatic but stable, and who have normal or inconclusive plain radiographs but an ongoing clinical suspicion of FB aspiration. 6 The sensitivity of CT scans for FBA is almost 100% and specificity is 66.7% to100%. Unlike plain radiography, CT scans can usually detect radiolucent FBs such as vegetables. A clinically suspected FBA should ultimately be ruled out by bronchoscopy regardless of radiographic findings. 6 Although a flexible bronchoscopy might help in diagnosis, removal of most FBs using the currently available flexible bronchoscopes is difficult. Regarding management of FBA in the pediatric age group, rigid bronchoscopy is the procedure of choice for both diagnosis and treatment. 10
The aim of this study was to study the pattern of foreign-body aspiration in the tracheobronchial tree as well as the success rate of rigid bronchoscopy in children admitted to a single center and to analyze the relationship of the type of FB with patients’ age, presentation, and complications.
Patients and Methods
This was a retrospective, single-center, cross-sectional study conducted from June 2014 to November 2016. The data were collected from the medical records. Infants less than 6 months of age and adolescents more than 15 years of age were excluded from the study. Also, children with suspected FBA but negative bronchoscopy were excluded. Rigid bronchoscopy (Karl Storz Endoskope system caliber 3.5-4.5 mm) was used under general anesthesia for all patients. One patient underwent flexible bronchoscopy (Olympus CV-180 CLV-180 Evis Exera II Endoscopy System) after failed rigid bronchoscopy. Another underwent thoracotomy after failed rigid bronchoscopy. Informed consent was taken from all parents before performing the procedures. Data extracted for the study included age, gender, ethnicity, history of choking, sign and symptoms, radiological finding, time interval between clinical presentation and diagnosis, types and location of the FBs in the airways, and any complication from the procedures. The data were analyzed, using IBM SPSS software, version 21. A P value ≤.05 was considered significant.
Results
A total of 83 patients were included in the study. The patient’s age ranged from 6 months to 15 years, with a mean age of 2.5 years. In all, 43 patients (51.8%) were female, and 40 (48.2%) were male; 44 patients (53.0%) came from rural areas, and 39 patients (47%) were from urban regions. In 68 patients (81.9%), the FBs were organic; others (15, 18.1%) were inorganic. Table 1 shows the types of FBs with their frequency of occurrence.
Types of Foreign Bodies in Detail.

History of choking was positive in 77 patients (92.8%) and cough in 73 (88%). The most common sign was cyanosis (36 patients, 43.4%) followed by stridor (32 patients, 38.6%). Table 2 shows the signs and symptoms of patients with FBA.
Signs and Symptoms of Foreign Body Aspiration in 83 Patients.

The duration of the complaint ranged from half an hour to 1 year, with a mean time of 12 hours. Chest X-ray (CXR) was normal in 33 patients (40%). CT scan of the chest was done for 2 patients who presented with repeated attacks of chest infection for 9 and 10 months, respectively. Image findings and sites of FB impaction are presented in Table 3.
Shows Image Findings and Sites of Foreign Body Impactions.

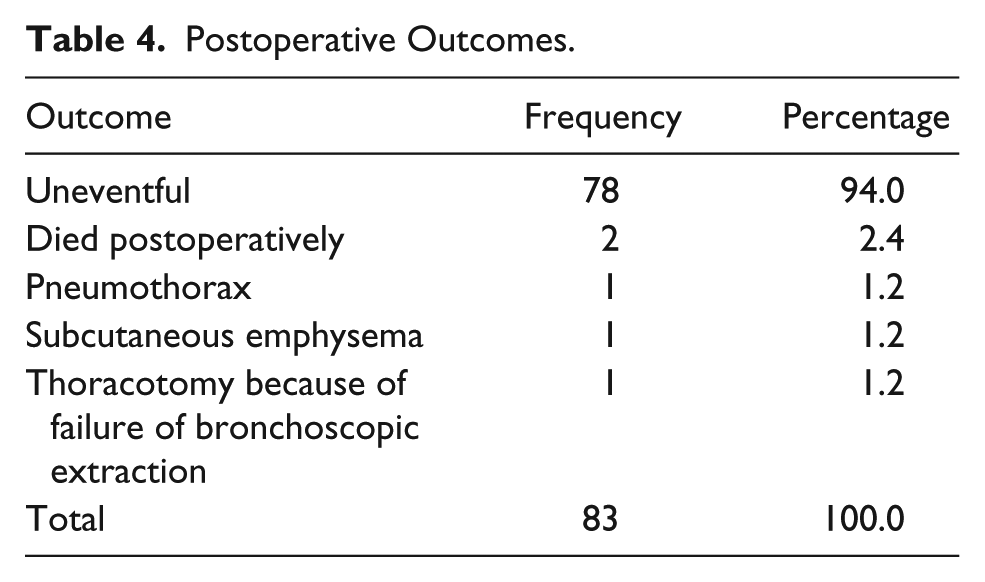
In 1 patient (1.2%), the FB was removed by flexible bronchoscopy under local anesthesia and in 81 patients (97.6%) by rigid bronchoscopy under general anesthesia. The remaining patient (1.2%) underwent left posterolateral thoracotomy for extraction of the FB. The duration of postoperative admission ranged from 4 to 120 hours, with a mean of 22.51 hours (±17.572). Postoperative outcome was uneventful in 72 patients (94%). Table 4 shows the outcomes.
Postoperative Outcomes.
There was a significant relationship between the type of FBs and the outcome (P = .013), with aspiration of sharp objects being more dangerous (Table 5).
Relation of Postoperative Outcome to the Duration of Symptoms, Site, and Type of Foreign Body.

Abbreviations: FB, foreign body; HS, head scarf needle; LBT, left bronchial tree; PM and SC emphysema, pneumomediastinum and subcutaneous emphysema; RBT, right bronchial tree.
Also, the relationship was significant between dyspnea and pneumonia and the type of FBs (P = .009, .034, respectively) among the rest of the clinical findings, which were not significant. Dyspnea and pneumonia were most commonly encountered if organic substances were aspirated, with sunflower seed being the most common, followed by nuts.
Discussion
FBA is most common with children less than 3 years old. 11 In this study, the mean age of presentation was 2.5 years. Curiosity to explore the world via the oral route, failure in the laryngeal closure reflex, inadequate swallowing reflex, and activity while eating are the most common etiological factors. 12 In the current study, the male to female ratio was 0.93:1, which is the opposite of that found in previous studies.13,14 Further studies are necessary to confirm and explain this deviation from the international standard.
FBA has a global variation. Consistent with previous studies done in Pennsylvania, Iran, Brazil, and Lebanon, 81% of FBs aspirated in this study were organic.13-15 Sunflower seed was the most common FB (49%), similar to a study done in Iran, which may be related to close similarities in cultural habits. 15 However, bones were the most commonly aspirated FBs in Southeast Asia and China.16,17 Similarly, seeds of watermelons, sunflowers, and pumpkins are more prevalent in Egypt, Turkey, and Greece, respectively. 18 This is because of differences in food habits, reflecting a cultural impact. 19 Moreover, religion has some role to play; 8 patients (9.6%) in the recent study aspirated scarf pins; 6 of them were female adolescents who were holding the pin between their lips while wearing Hijab. The is the characteristic type of FB recently cited in the literature as Scarf pin–related Hijab syndrome. 20
The key to reaching a definitive diagnosis lies in a detailed history that identifies risk factors, an examination that elicits important signs, and supportive CXR findings. Diagnostic bronchoscopy should be performed when any one of the above modalities is positive. Otherwise, both examination and radiography should be repeated 24 hours apart given a negative history and inconclusive initial examination and imaging in a stable patient. 19 The author decided to do bronchoscopy on this basis because none of our patients was asymptomatic, and 92.8% of patients had a positive history of choking, which is the most important aspect in the history that may lead to a misdiagnosis if missed. The second common symptom was cough followed by dyspnea, very similar to that in studies by Safari and Manesh 15 and Fraga et al. 13
Unlike most of the previous studies that we reviewed,13,21,22 normal chest auscultation (with normal air entry and no added sounds) was the most common finding we encountered; also most of the patients had a normal CXR. Sink et al, 21 Liang et al, 22 and Fraga et al 13 found that the most common chest examination findings are rhonchi (in the former) and decreased breath sounds (in the last two), whereas the most common CXR findings were air trapping, mediastinal shift, and atelectasis, respectively. The high percentage of normal CXRs in this study may be related to the fact that most of our FBs were organic, which are radiolucent; the result could also be improved if CXRs are taken in full expiration and inspiration. CT scan of the chest was conducted for 2 of our patients; the authors avoided routine use of CT scan as a diagnostic tool despite its high sensitivity and specificity, to minimize exposure to ionizing radiation.
As in previous studies, the most common site of impaction was the right bronchial tree (39.8% in our sample); this was mostly because of the position of bronchi (the left bronchus is attached to the trachea with a more acute angle than the right one) and also because of the wider right bronchial diameter in comparison to the left bronchus.13,14,21,22
There was a significant relationship between type of FBs (whether organic or nonorganic) and pneumonia and dyspnea, which may be a result of the fact that organic materials cause more inflammatory reaction in comparison to nonorganic materials. 19
Conclusion
History is considered the most important factor in the accurate diagnosis of FBA. Diagnostic bronchoscopy is mandatory in any suspected case, even if chest examination and CXR are normal. Organic materials cause more inflammation and local reaction with subsequent complications.
Footnotes
Acknowledgements
We would like to acknowledge all our personnel who assisted in serving our patients.
Author Contributions
AB: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
HS: Contributed to design; contributed to interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SS: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
FHK: Contributed to conception and design; contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AMHH: Contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.