
Abstract
Several studies and the Accreditation Council for Graduate Medical Education recommend integration of medical home (MH) concepts into pediatric resident training. There is a paucity of research depicting the current landscape of pediatric resident MH education. We hypothesized formal MH curricula in pediatric residency education are limited and pediatric residency programs desire incorporating MH education into curricula. A national needs assessment of pediatric residency programs was conducted assessing inclusion of MH concepts in training. Outcomes assessed were perceived importance of including MH concepts, satisfaction of current curriculum, content taught, resources available, and barriers encountered. Fifty-six programs (28%) completed the survey, majority academic programs. Nearly 75% indicated interest in incorporating MH concepts. Fifty-one percent of programs reported faculty knowledgeable in MH concepts/implementation and 11% reported access to readily available resources. Barriers included resident schedules, faculty teaching time, funding, and not faculty priority. Pediatric program directors report interest and need for improved MH training but identify implementation barriers.
Keywords
Introduction
The patient- and family-centered medical home is the standard of care in primary care. 1 Providing this care ensures the needs of patients and families drive care delivery coordinated among providers, partners, systems, and agencies2,3 and improve health care quality and child/family functioning. 4 With its genesis in pediatrics, 5 medical home evolved in pediatric and adult sectors over the past decade.3,6-9 Understanding concepts of the medical home 10 is critical for general and subspecialty pediatricians,11-14 as patient-/family-centered care and care coordination is necessary across all systems. While gaining momentum, many medical home demonstration projects,15,16 certification/recognition programs,17-20 and practice transformation efforts21,22 evolved supporting providers and practices. 23
Incorporating medical home training into pediatric residency programs has been suggested by several authors and studies.24-32 A new resident curriculum training residents to elicit family feedback was found useful, reasonably implemented, and garnered support. 31 The Accreditation Council for Graduate Medical Education (ACGME) requires all pediatric residents receive training on “coordination of care [and] longitudinal management of children/youth with special needs.” 32 However, there is a paucity of research depicting the current landscape of pediatric residency medical home resident education. In response to this gap, a Medical Home Resident Education Initiative Work Group (REIWG) was created via the American Academy of Pediatrics (AAP) National Center for Medical Home Implementation in 2011. The REIWG conducted a needs assessment informing development of a medical home curriculum. Study objectives were the following: understand and identify current state of medical home training in US pediatric training programs, understand pediatric program directors’ perspectives, and identify gaps and barriers. The REIWG hypothesized that (1) formal medical home curriculum experiences in residency education are limited and (2) pediatric residency programs desire incorporating medical home education into curricula.
Methods
The Medical Home Resident Education Initiative Work Group
The purpose of the REIWG was to identify pediatric training needs related to the medical home, care coordination, and family-centered care for all children, with special emphasis on children with special health care needs. REIWG members include representatives from AAP, Academic Pediatric Association (APA), Association of Pediatric Program Directors (APPD), Continuity Research NETwork (CORNET), 33 residency program directors, residents, family members, and medical home content experts. Established in 2011, the group met in person 3 times, convened quarterly via teleconference, and collaborated electronically on developing documents, surveys, and curricula components.
The REIWG developed a survey assessing the current state of medical home training, with topics informed by literature, evidence for medical home in practice, medical home recognition (eg, National Committee for Quality Assurance), and experts in the medical home and residency education fields.17,20 The topics were refined and discussed by REIWG members on multiple calls/webinars. This study was approved by the AAP Institutional Review Board.
Study Design
The resulting cross-sectional survey (22 questions; available online at http://journals.sagepub.com/home/gph) assessed needs related to medical home curricula:
Sociodemographic characteristics (program type, geographic location, respondent role, program size)
Satisfaction with medical home curriculum utilized if any, resources, and perceived importance of medical home principles
How programs currently teach concepts, as organized around key functions: Care Partnership and Support; Care Delivery Management; Clinical Care Information and Management; Resources and Linkages; and Practice Performance Management and Payment and Finance 34
Perceived areas for growth
Perceived barriers
To rank importance of a concept, respondents selected from “Important,” “Somewhat Important,” “Not Important,” or “Do Not Know” for each item listed. For satisfaction-related questions, respondents selected from “Satisfied,” “Somewhat Satisfied,” “Not Satisfied,” and “Do not know” for each item. When assessing barriers, respondents were asked to select all that apply from the following: Providing faculty time to teach; Finding time in resident schedules; Lack of faculty expertise; Lack of funding; Lack of resident interest; Not a priority to some faculty; No barriers identified; Do not know; and Other.
The survey was approved by the APPD for distribution to the national APPD listserv. Two of the authors met with members of the APPD Curriculum Taskforce for formative feedback and expert opinion. The electronic survey was sent to program directors of the 196 Pediatric Residency Training Programs members of the APPD 35 in March 2011 36 via their specific listserv. Inclusion criteria included any pediatric residency program directors whose programs are members of the APPD in the United States.
Only 2 accredited Pediatric Residency Training Programs not members of APPD were not surveyed. 37 Program directors were asked to complete the survey themselves, or have a representative with more expertise complete it. Three reminder emails were sent over 6 months encouraging participation. Emails were sent via the APPD listserv and results were de-identified before tabulated.
Statistical Analysis
Results were analyzed using descriptive statistics, and frequencies and means were calculated utilizing SPSS statistical software (version 20.0). 38 All qualitative comments were collated by the study coordinator and reviewed by the REIWG team for themes and consistency.
Results
Fifty-six program directors (of 198 surveyed) or their designee completed the survey (response rate 28%). Table 1 depicts demographic characteristics of respondents. The majority of respondents were program directors (80%) and from academic programs. Respondents represented pediatric training programs from 30 states with at least one program from each US Census Bureau–defined region. 39 Most programs provided training for 21 to 40 categorical pediatric residents with a range of 0 to 128 (one program was new and participated in meetings before residents were accepted; ignoring this program, the range was 17-128; see Table 1).
Demographics of Residency Programs and Respondents a .
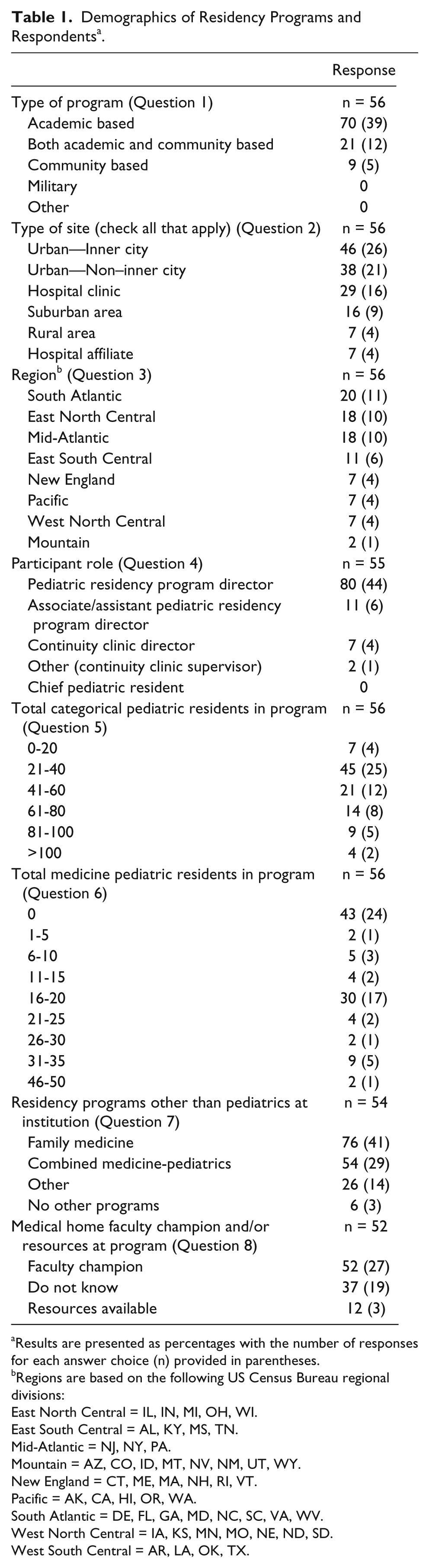
Results are presented as percentages with the number of responses for each answer choice (n) provided in parentheses.
Regions are based on the following US Census Bureau regional divisions:
East North Central = IL, IN, MI, OH, WI.
East South Central = AL, KY, MS, TN.
Mid-Atlantic = NJ, NY, PA.
Mountain = AZ, CO, ID, MT, NV, NM, UT, WY.
New England = CT, ME, MA, NH, RI, VT.
Pacific = AK, CA, HI, OR, WA.
South Atlantic = DE, FL, GA, MD, NC, SC, VA, WV.
West North Central = IA, KS, MN, MO, NE, ND, SD.
West South Central = AR, LA, OK, TX.
Nearly three quarters of respondents indicated interest in incorporating a medical home curriculum. Respondents rated each key function as important with a range of 51% (payment and finance) to 95% (clinical care information). See Figure 1. However, respondents were more often “somewhat satisfied”/“not satisfied” than “satisfied” with their current curricula (Figure 2). The key function of payment and finance was the area with the highest rating of dissatisfaction.

Perceived importance of the building blocks in resident education.

Reported satisfaction of current curricula and/or related learning opportunities for residents related to the building blocks.
Programs reported information on current medical home curricula/content included in resident education (Table 2) and current teaching methodologies (Table 3).
Content Currently Taught in the Building Blocks a .

Results are presented as percentages with the number of responses for each answer choice (n) provided in parentheses.
Respondents were asked to select all that applied for most of their residents.
Other: Do not know.
Methods Used for Resident Education Around Medical Home a .
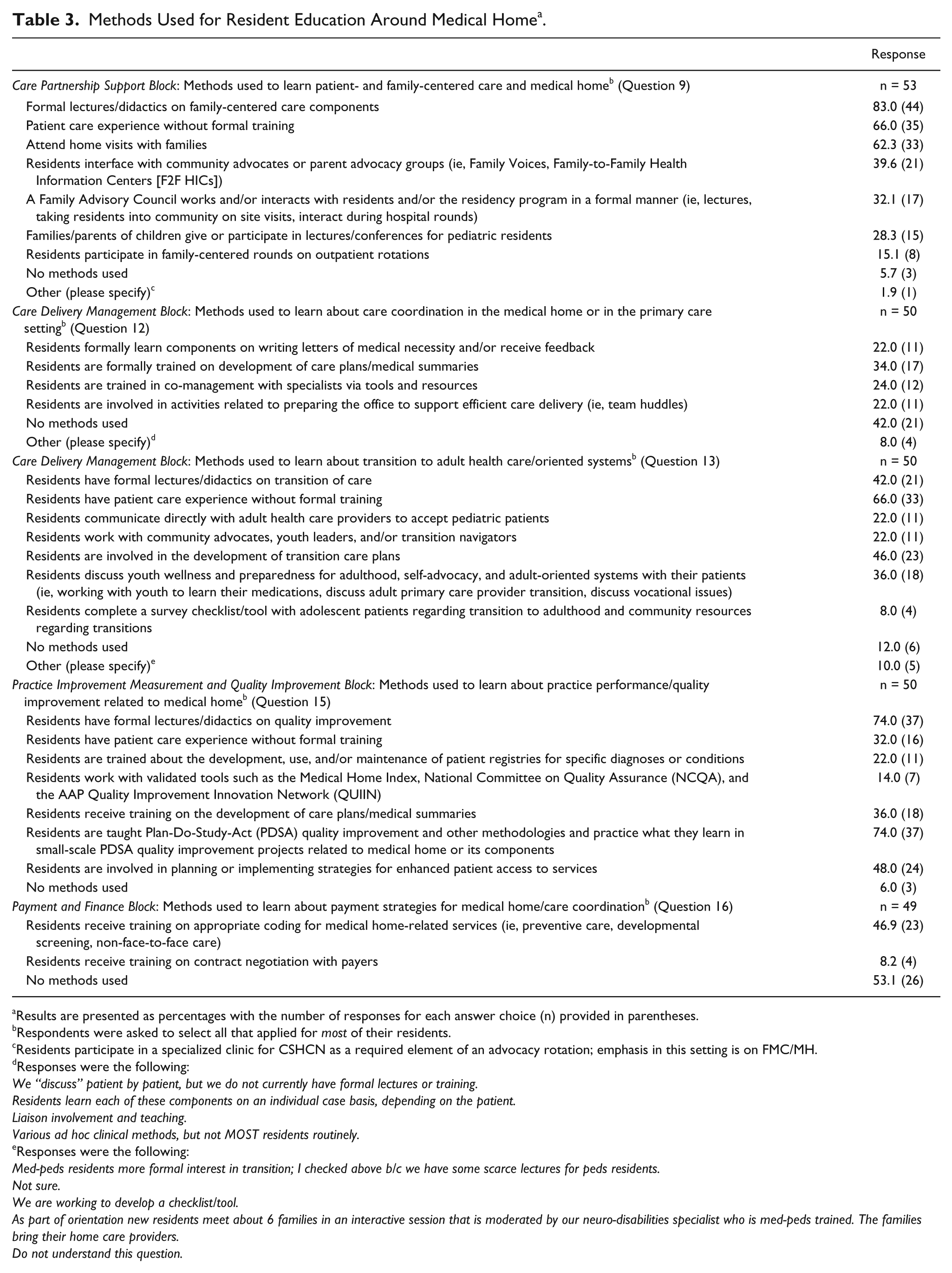
Results are presented as percentages with the number of responses for each answer choice (n) provided in parentheses.
Respondents were asked to select all that applied for most of their residents.
Residents participate in a specialized clinic for CSHCN as a required element of an advocacy rotation; emphasis in this setting is on FMC/MH.
Responses were the following:
We “discuss” patient by patient, but we do not currently have formal lectures or training.
Residents learn each of these components on an individual case basis, depending on the patient.
Liaison involvement and teaching.
Various ad hoc clinical methods, but not MOST residents routinely.
Responses were the following:
Med-peds residents more formal interest in transition; I checked above b/c we have some scarce lectures for peds residents.
Not sure.
We are working to develop a checklist/tool.
As part of orientation new residents meet about 6 families in an interactive session that is moderated by our neuro-disabilities specialist who is med-peds trained. The families bring their home care providers.
Do not understand this question.
Half of programs reported having faculty knowledgeable in medical home concepts and implementation (51%). Only 11% reported access to readily available resources (identified as faculty with access to AAP information, local community-based resources, case managers, electronic medical records, special medical home clinics, and faculty with limited knowledge and commitment). Over one third of programs reported no knowledge of such resources (36%). Furthermore, 60% of programs did not have a care coordinator.
Barriers to implementing a medical home curriculum included the following: finding time in resident schedules (79%), providing faculty time to teach (69%), lack of faculty expertise (53%), lack of funding (46%), not a priority to some faculty (42%), and lack of resident interest (16%). Respondents were asked to select all barriers they felt were relevant. Two respondents did not identify any barriers and 2 selected “don’t know.” Other barriers written in by respondents related to the increased learning demands placed on residents.
Discussion
This study is among the first presenting national data on the state of medical home education in US pediatric residency training programs. The results suggest programs are supportive of teaching medical home concepts but are not satisfied with current curricula. Specific needs include training in key functions of the medical home, specifically Health Care Delivery and Management and Payment and Finance, as supported by the lowest satisfaction scores reported in this study. Programs use mixed methods to teach medical home, such as participating in direct patient care, home visits, formal didactics, training in use of validated tools and QI processes, and family as teacher initiatives (Table 3). Barriers include limited faculty expertise, limited training time, and lack of resources.
Our findings suggest the need for further development and implementation for residency programs teaching patient and family centeredness to residents. Only 59% of respondents reported existing training for residents on eliciting feedback from families and parent partners. Furthermore, approximately a third of programs (38%) incorporate resources teaching about family to family supports and linkages, and few programs have residents work with family advisory councils, community partners, or have family faculty. This focus on family-centered care and community partners in education for residents represents an opportunity for pediatric residency programs to educate on an essential aspect of the medical home.
Effective care coordination/integration and transition to adult oriented systems are also critical aspects of high-quality medical homes for patients and families. 10 This study suggests that few programs are teaching self-care, writing letters of medical necessity, co-management, or care plan development. Less than half of residency programs in this study have formal didactics on transition of care to adulthood or develop transition care plans and less than a quarter of respondents reported residents communicate with adult health care providers, work with transition advocates, or use transition care plan checklists that are accepted as core elements in the transition process for youth.40-43 There are resources available40,44,45 for training pediatric residency programs in these areas as they are relevant to primary care, specialty care and inpatient medicine.
Curricula have been suggested throughout the past decade for incorporating medical home training into residency.25-27,46 Several pilot studies in adult primary care suggest favorable outcomes for integrating team-based care and components of the patient-centered medical home into residency education.47-50 Several medical home pediatric resident training initiatives have been developed and implemented at the local and regional levels.8,51 Outcomes include decreased emergency department utilization, 8 increased resident satisfaction,8,51 improved resident self-efficacy in setting patient-centered treatment goals, 51 a feasible and acceptable curriculum,46,51 and increased family satisfaction. 8 A web-based curriculum was reported to increase resident knowledge, confidence, and utilization of medical home principles.52,53 Training in patient-centered activities such as Family-Centered Rounding and home visiting programs are supported by residents.54,55 A study of the Health Begins at Home initiative demonstrated urban pediatric residents gain an increased understanding of their patients’ community and home environments through participating in home visits and stress home visiting is important and should be incorporated into permanent training curricula. 55 Additional successful strategies include online reflective writing with structured feedback 56 and parent-led curricula 57 to improve resident learning and understanding of family-centered care delivery within the medical home. Some initiatives did not demonstrate significant improvement in outcomes with the new initiatives, possibly due to barriers in implementation. 58 This study shows the importance of implementing medical home curriculum and our curriculum and web-sites can serve as additional resources for training programs (see Next Steps).
Limitations
One limitation of this study is it is a cross-sectional assessment of pediatric residency programs in 2011. The responses reflect the opinion and experiences of the survey respondent and could represent an underestimation of actual medical home activities in the residency program. Due to parsimonious survey length, we were unable to assess activities related to hand offs and transition of care from inpatient to outpatient settings and into other facilities, which is a growing body of resident education experience. Our response rate was 29% and only represents the opinions of respondents. Strengths included surveying through a national organization and representation from all US regions.
Next Steps
The next steps of REIWG were to develop a curriculum addressing limited faculty expertise, time in training, and lack of resources reported by programs. The group used the needs assessment to develop a national-level medical home curriculum based on the key functions of the medical home. This competency-based curriculum is available as 5 self-contained case-based modules focusing on key medical home principles. The modules are available online via the AAP website. 44 The content of the modules addresses ACGME core competencies of Patient Care and Procedural Skills; Medical Knowledge; Practice-Based Learning and Improvement; Interpersonal and Communication Skills; Professionalism; and Systems Based Practice. 59 Further assessment of this curriculum is indicated.
Conclusion
Pediatric residency training programs report the need for improved medical home education and training but are limited by faculty time, expertise, resources, and time in training. Additional efforts and evaluation focused on medical home with faculty development, educational competencies, and curricula warrant consideration.
Author Contributions
RMT: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AN: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
ME: Contributed to conception; contributed to acquisition and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JRS: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Acknowledgements
The authors would like to acknowledge the work and contributions of The Medical Home Resident Education Initiative Work Group (REIWG) for their ideas, support, and development of this work. REIWG members include Molly Cole, Juno Duenas, Michelle Esquivel, Matthew Garber, Garry Gardner, Marcia Jackson, Thomas Klitzner, Jennifer LeComte, Aditee Narayan, Umbereen Nehal, Robyn Nolan, Eugene Rich, Janet Serwint, Scott Shipman, Heather Stob, Angela Tobin, Renee M. Turchi, Dennis Vickers, and Susan Wiley. The REIWG represented members from the American Academy of Pediatrics (AAP), The Academic Pediatric Association (APA), Association of Pediatric Program Directors (APPD), Association of American Medical Colleges (AAMC), parents/caregivers, resident members, and staff. We would like to acknowledge CORNET members for their review and feedback on this work and future modules which has informed the REIWG materials. We would also like to acknowledge Heather Stob, staff at the American Academy of Pediatrics, for her technical assistance in organizing meetings, dissemination of the survey, and compiling of results; Dana Bright, MSW, also staff at the American Academy of Pediatrics, for her technical assistance; and Renee Davis, MD, MPH, Drexel Dornsife School of Public Health, for her assistance in editing the article.
Authors’ Note
The results of needs assessment have been presented at APPD and Pediatric Academic Societies (PAS) meetings in 2012.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.