
Abstract
We tested the independent and combined influence of overweight/obesity and meeting moderate to vigorous physical activity (MVPA) guidelines (≥60 minutes per day) on cardiometabolic risk factors among healthy adolescents. We measured anthropometry, blood pressure, fasting lipids, and activity by accelerometer in 223 adolescents. They were categorized as overweight/obese versus normal weight and meeting the World Health Organization guidelines for MVPA per day. Adolescents were 16.8 years, 41% overweight/obese, 30% met MVPA guidelines, 50% low high-density lipoprotein, 22% high triglycerides, 12% high blood pressure, and 6% high fasting glucose. Controlling for sex, overweight/obese adolescents who did not meet MVPA guidelines had 4.0 and 11.9 increased odds for elevated triglycerides and systolic blood pressure, respectively, compared to normal weight adolescents who met MVPA guidelines. Overweight/obese and normal weight adolescents who met MVPA guidelines did not differ in cardiometabolic risk factors. Among overweight/obese adolescents, being physically active attenuated the likelihood of high triglycerides and systolic blood pressure.
Introduction
Childhood overweight and obesity are associated with cardiometabolic risk factors including elevated systolic blood pressure (SBP), diastolic blood pressure (DBP), triglycerides (TG), fasting glucose, and low high-density lipoprotein (HDL).1-13 In addition, physical activity plays a role in cardiometabolic risk with less physical activity associated with higher risk.14-18 Low levels of physical activity are increasingly common even in childhood,19-22 reaching the level of a global pandemic. 23 The dual risks of overweight/obesity and low levels of physical activity in childhood threaten adult health as developing cardiometabolic risk during childhood increases risk for developing coronary heart disease, diabetes, and stroke in adulthood.2,24-34
Few studies have focused on the combined effects of physical activity and weight status on cardiometabolic risk during childhood and adolescence. Vale et al studied preschool children and found that lower levels of moderate to vigorous physical activity (MVPA) and overweight/obesity increased risk for elevated blood pressure synergistically. 35 Prior research in adolescents has shown that increasing physical activity was associated with lower cardiovascular risk. However, no distinction was made between normal weight and overweight adolescents. 15 Thus, an important question has not been addressed: Does physical activity provide the same protective benefits for children and adolescents already overweight/obese as for normal weight youths?
The primary goal of this study was to evaluate the independent and combined association of weight status and physical activity on cardiometabolic risk in a community-based sample of healthy Chilean adolescents.
Methods
Participants were part of an infancy iron deficiency anemia preventative trial and follow-up study in Santiago, Chile. Detailed descriptions of the original study, including inclusion criteria, have been previously described. 36 Healthy infants from uncomplicated singleton vaginal births at term were recruited at 4 months of age. Inclusion criteria included no iron deficiency anemia, birth weight ≥3 kg, and residence in 1 of 4 low- to middle-socioeconomic neighborhoods in Santiago, Chile. A total of 1657 infants completed the trial in which they received either iron supplementation or usual nutrition between 6 and 12 months.
Participants were subsequently followed-up to evaluate the longitudinal effects of preventing infant iron deficiency anemia at 5 (n = 888) and 10 years (n = 1127). At 16 years, a random sample of the original infancy cohort was invited to participate in a study of cardiovascular risk. A total of 679 adolescents participated, and of those a convenience sample of 300 adolescents was invited to wear an accelerometer on the hip for measurement of physical activity. Our analytic sample (n = 223, 49% female) consisted of adolescents with complete accelerometer data and measurements of blood pressure, anthropometry, and fasting plasma biomarkers including HDL, low-density lipoprotein, TG, and glucose, among others. There were no differences with respect to odds of having abnormal levels of BP, TG, HDL, or glucose in our convenience sample of adolescents with complete data compared to those in the cohort not included in the analysis. The study was approved by the institutional review boards at the University of California, San Diego, and the Institute of Nutrition and Food Technology (INTA), University of Chile, the study site in Chile. All study procedures were carried out in accordance with the Code of Ethics of the World Medical Association, with parents providing written and signed consent and adolescents assent to participate.
Physical Activity
Adolescents were scheduled for a half-day assessment at the INTA, University of Chile. A week before evaluation, study personnel visited each participant to explain research procedures, including placement of the hip-worn accelerometer. Participants were instructed to wear the accelerometer during waking hours on an elastic band worn on top of clothing and to remove the device for showering, swimming, and sleeping. Physical activity data were cleaned and processed to ensure that hip accelerometers were worn for ≥10 hours/day for ≥5 days or ≥3000 minutes during a 4-day period. Evenson cut points were applied to classify the time spent in MVPA. 37 Adolescents were considered as meeting MVPA guidelines if they averaged ≥60 minutes of MVPA per day according to the World Health Organization guidelines. 38
Anthropometric Data
During the half-day evaluation, body mass in kilograms and height in centimeters were measured 3 times by a trained physician at INTA and the average was computed. Body mass index (BMI; kg/m2) was then calculated and participants were categorized into overweight/obese or normal weight if the BMI z-score was >1 or ≤1 (equivalent to BMI 25 kg/m2 at 19 years), respectively, based on the World Health Organization guidelines. 39
Blood Pressure
Average SBP and DBP were measured according to the National Health and Nutrition Examination Survey protocol. 40 Elevated averages of SBP or DBP were defined as values that were ≥90th percentile for age and sex according to Cook’s criteria. 41 High blood pressure (BP) was defined as having either elevated SBP or DBP.
Fasting Plasma Biomarker Concentration
A venipuncture blood sample was collected after an overnight fast. Samples were processed, stored (−80°C), and analyzed at the Micronutrient Laboratory, INTA, following standard procedures for quality assurance and control. Serum TG, cholesterol, and glucose levels were assessed using an enzymatic-colorimetric test (QCA SA, Amposta, Spain). Cardiometabolic risk factors were defined as follows: low HDL (≤40 mg/dL), high TG (≥110 mg/dL), and elevated glucose (≥100 mg/dL). 41
Statistical Analyses
Using SPSS, we described continuous variables with means and standard deviations and categorical variables with percentages. Using logistic regression, we first modeled the independent effect of overweight/obesity on cardiometabolic risk factors: low HDL and elevated TG, SBP, DBP, and glucose. Then we conducted a second series of models, examining the combined association of weight status (overweight/obese vs normal weight) and MVPA guidelines (did not meet guidelines vs met guidelines) on the same cardiometabolic risk factors. Three dummy variables were created to test differences between the reference group (normal weight adolescents who met MVPA guidelines) and (1) normal weight adolescents who did not meet MVPA guidelines, (2) overweight/obese adolescents who met MVPA guidelines, and (3) overweight/obese adolescents who did not meet MVPA guidelines. For both steps, we created separate logistic regression models for each cardiometabolic risk factor and adjusted for sex.
Results
Descriptive statistics of the sample are described in Table 1. The prevalence of overweight/obesity was 41.2%. Approximately 69.1% of the adolescents did not meet the daily MVPA recommendation. Elevated SBP and DBP occurred in 9.0% and 5.4%, respectively. Meeting MVPA guidelines did not significantly differ by overweight/obese status.
Demographics and Prevalence of Cardiovascular Risk Factors Among Chilean Youth (N = 223) a .

Abbreviations: MVPA, moderate to vigorous physical activity; WHO, World Health Organization; BMI, body mass index; WC, waist circumference; HDLc, high-density lipoprotein cholesterol; TG, triglyceride; SBP, systolic blood pressure; DBP, diastolic blood pressure.
Values are either mean ± SD or n (%).
Overweight/obesity was associated with higher odds of all cardiometabolic risk factors tested: low HDL (odds ratio [OR] = 3.0, 95% confidence interval [CI] = 1.7-5.4) and elevated TG (OR = 3.2, 95% CI = 1.6-6.2), SBP (OR = 6.7, 95% CI = 2.1-20.9), DBP (OR = 4.6, 95% CI = 1.2-17.5), and glucose (OR = 4.1, 95% CI = 1.2-13.6).
Table 2 shows logistic regression models for associations between weight status and MVPA group and cardiovascular risk factors, adjusted for sex. Normal weight adolescents who did not meet MVPA guidelines had cardiometabolic risk profiles that did not differ from those of normal weight adolescents who met MVPA guidelines. However, adolescents who were overweight/obese and did not meet MVPA guidelines had 4.0 (1.3-11.7, P < .05) increased odds of having elevated TG and 11.9 (1.3-102.8, P < .05) increased odds of elevated SBP compared to normal weight adolescents who met MVPA guidelines. Overweight/obese adolescents who met MVPA guidelines, however, did not have increased odds of elevated TG or SBP, compared to the reference group of normal weight adolescents who met MVPA guidelines. We found a similar trend for elevated glucose, with overweight/obese adolescents who did not meet MVPA guidelines with increased odds of elevated BG (OR = 4.1, 95% CI = 0.7-23.0, P = .10), compared to the reference group. Both overweight/obese groups (those who met and did not meet MVPA guidelines) had increased odds of low HDL, compared to the reference group. Weight status and meeting MVPA guideline did not relate to elevated DBP (data not shown).
Associations Between Weight Status and Physical Activity Group on Cardiovascular Risk Factors, Adjusted for Sexa.
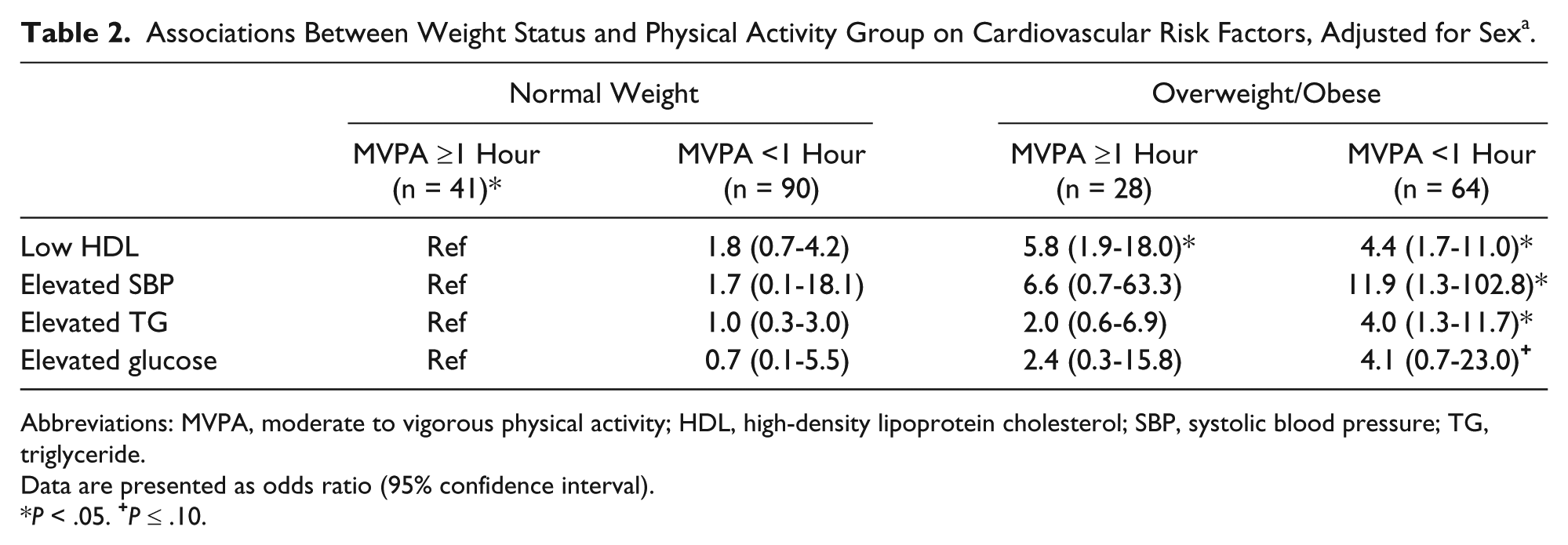
Abbreviations: MVPA, moderate to vigorous physical activity; HDL, high-density lipoprotein cholesterol; SBP, systolic blood pressure; TG, triglyceride.
Data are presented as odds ratio (95% confidence interval).
P < .05.
Discussion
Considerable research now exists supporting the association between overweight/obesity in childhood and cardiovascular disease in adulthood.1,4 Physical activity is one potential modifiable health behavior, and meeting MVPA guidelines has been shown to decrease cardiovascular risk in adolescents. The primary goal of our study was to investigate the independent and combined effects of weight status and physical activity level on cardiometabolic risk factors in a community-based sample in Santiago, Chile. In overweight/obese adolescents, we found that meeting MVPA guidelines attenuated cardiovascular risk. Among overweight/obese adolescents, those who met MVPA guidelines did not differ from the reference group (normal weight/met MVPA guidelines) in likelihood of elevated blood pressure or abnormal lipid levels. On the other hand, overweight/obese adolescents who did not meet MVPA guidelines had higher likelihood of elevated SBP and TG compared to the reference group.
The evidence that early life cardiovascular risk factors are likely to persist into adulthood increasing morbidity and mortality has propelled the idea that efforts during childhood could prevent cardiovascular disease in adulthood.2,3,5-13 While there is little question about the association between childhood overweight/obesity and later cardiovascular disease, treatment of overweight/obesity in childhood has proven to be difficult and prevention is not yet achievable. 42 These findings could inform important public health and clinical research testing implementation of 60 minutes/day of physical activity in overweight/obese adolescents. The behavior change message is straightforward but allows individual choice in timing and type of daily physical activity. Prior research has shown that physical activity is equally effective whether achieved in bouts (≥5 consecutive minutes) or bursts (<5 consecutive minutes). 43 For some 60 minutes of physical activity achieved throughout the day may be easier than scheduling a 60-minute period of activity. Implementation of 60 minutes per day of MVPA may be acceptable and feasible for many and could provide considerable motivation and hope for better health for overweight/obese adolescents. The simplicity of this recommendation, without requiring micromanagement of physical activity, could empower and motivate adolescents and families to meet MVPA guidelines. It is encouraging that decreasing cardiometabolic risk may be possible for overweight/obese adolescents without weight loss, as weight loss is a daunting task for many. Instead, meeting MVPA guidelines may be enough to provide health benefits that, if maintained, may lead to improved adult health outcomes.
Strengths of this study include physical activity measured by accelerometers worn on the trunk, fasting laboratory studies, anthropometry, and blood pressure measured using standardized procedures at a nutrition research institute. In addition, our study has several limitations. The small sample size limits our ability to detect small differences. Furthermore, the cross-sectional design does not allow us to infer temporal precedence or causality. Future studies should evaluate the influence of meeting MVPA guidelines in adolescents with cardiovascular health in adulthood.
Author Contributions
HW: Contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
EB: Contributed to analysis and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CA: Contributed to conception and design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
PP: Contributed to conception and design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
RB: Contributed to conception and design; contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
MR: Contributed to acquisition; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
DW: Contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JGG: Contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SG: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Acknowledgements
The authors would like to thank the study participants and their families for their ongoing commitment to the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Institutes of Health, Heart, Lung, and Blood Institute (HL088530, PI: Gahagan) and the National Institute of Child Health and Human Development (HD14122 and HD33487, PI: Lozoff).