
Abstract
This is a prospective quality improvement project for patients with cystic fibrosis who are 5 years of age and older who were admitted for intravenous antibiotic administration as part of treatment of cystic fibrosis exacerbation. The goal of this project was to compare the pharmacokinetics of once-daily versus thrice-daily aminoglycoside use when treating cystic fibrosis exacerbation in different age groups. Of the total of 119 patient encounters, 82.4% were started on once-daily dosing, and the remainder were started on thrice-daily dosing. Patients with pharmacokinetics allowing the continuation of once-daily dosing differed from patients who required a switch to thrice-daily dosing in terms of baseline forced expiratory volume in 1 second, forced expiratory flow from 25% to 75% of vital capacity, age, and body mass index (BMI) but were similar in BMI percentiles. The once-daily dosing group had higher mean 18-hour level, higher mean half-life, higher mean area under the curve, and lower mean elimination constant. This study showed that aminoglycoside clearance is higher in younger children.
Introduction
Cystic fibrosis (CF) is the most common autosomal recessive life-shortening disease in Caucasians, with an incidence of approximately 1 in 3200 live births. 1 Patients with CF have impaired mucous clearance in several organs, especially the lungs. This leads to a vicious cycle of bacterial infection, inflammation, and airway obstruction, leading to progressive loss of pulmonary function. 2
Hence, pulmonary disease remains the leading cause of morbidity and mortality, 2 and the airways of CF patients become colonized with different microorganisms. 3 Early infections are most frequently caused by Staphylococcus aureus, Haemophilus influenzae, and later on Pseudomonas aeruginosa. 4 In early adulthood, approximately 80% of CF patients are colonized with P aeruginosa, which is a common cause of recurrent CF exacerbations and progressive pulmonary deterioration. 2
An expert panel convened by the Cystic Fibrosis Foundation continues to recommend treating acute pulmonary exacerbations caused by P aeruginosa with 2 antipseudomonal antibiotics with different mechanisms of action. 2 Typically, an aminoglycoside, such as tobramycin, is used in addition to another antipseudomonal antibiotic, mostly a β-lactam. 2 The use of extended-interval dosing (EID) of aminoglycosides was found to be equally effective and potentially safer than traditional thrice-daily dosing in both adults and children.5,6
The pharmacokinetics of the aminoglycosides has been extensively studied in patients with CF and was found to be different compared to the non-CF population. Patients with CF have a larger volume of distribution and faster renal clearance of aminoglycosides, requiring higher doses to achieve appropriate peak serum concentrations.7-10 This is specifically true for children who have higher clearance rates of antibiotics, including aminoglycosides, compared with adults. 11 Aminoglycosides exhibit concentration-dependent bacterial killing, which can be predicted by the Cmax:MIC ratio, 6 where Cmax refers to the maximum or peak drug concentration and MIC refers to the minimal inhibitory concentration of an antibiotic that inhibits growth of bacteria.
According to a recent national survey in the United States, 84.3% of CF centers reported using once-daily EID in their pediatric CF population. 12 Many CF centers adopted the standard use of EID when treating CF exacerbation, with pharmacokinetic studies aiming to avoid toxicity and ensuring adequate levels by monitoring aminoglycoside half-life (t½) and other pharmacokinetic parameters. So far, there have been no studies looking into the effect of different dosing regimens on the aminoglycoside t½ and elimination rates and how that reflects on microbial resistance and clinical outcomes. In our center, we use EID in patients who are 15 years old and older. We use the t½ to guide the use of aminoglycosides in our patients, and we adjust accordingly.
This is a 2-year-prospective quality improvement project to evaluate the difference in aminoglycoside pharmacokinetics in CF patients admitted to our institution for treatment of CF pulmonary exacerbation, with the use of the EID in patients 5 to 21 years of age. In this project, assessment of the relationship between aminoglycoside t½, age of the patient, and patient’s body mass index (BMI) percentile were done. The goal of this project was to determine the age at which EID regimen can achieve therapeutic drug levels to ensure adequate bacterial killing while avoiding toxicity and, possibly, the development of bacterial resistance.
Patients and Methods
This is a prospective study from January 2013 to December 2014 for CF patients admitted to University of Michigan Mott’s Children Hospital. Criteria for enrollment were a diagnosis of CF pulmonary exacerbation requiring intravenous antibiotics, including aminoglycosides, and age of 5 to 21 years. Exclusion criteria were patients with known history of hypersensitivity reaction to aminoglycosides or severe renal dysfunction/failure, which was defined as the need for dialysis, a creatinine level that was more than 1.5 times the patient’s baseline level, or a urine output of <0.5 mL/kg/h. Most antibiotic therapy included a β-lactam in addition to an aminoglycoside. The antibiotic selection was determined by the primary pulmonologist and was based on the most recent sputum or throat culture and sensitivity results for each patient.
Tobramycin was used in the majority of patients and amikacin or gentamicin was used occasionally. Once-daily aminoglycoside was started first and was adjusted, if needed, based on the calculated peak concentration and half-life. Patients younger than 5 years old were treated with thrice-daily dosing and were not included in the quality improvement project. The aminoglycoside was administered over 30 to 60 minutes. If patients were started for the first time on once-daily aminoglycoside dosing, 10 mg/kg/d was used for tobramycin and gentamicin, and for amikacin, the dosing was started at 30 mg/kg/d. Adjustment was made as needed. Patients with history of once-daily dosing of aminoglycoside were started on a similar weight-based dose from the previous hospital admission.
Serum samples were drawn via peripheral venipuncture to assess aminoglycoside concentrations. Serum levels were drawn at least 60 minutes after the end of the infusion and 10 hours postinfusion.
The pharmacokinetic goals for both tobramycin and gentamicin were a peak concentration of 20 to 30 mg/dL and a trough of ≤0.05 mg/dL. For amikacin, the 1-hour peak goal was 40 to 60 µg/mL and trough <8 µg/mL, with the same monitoring strategy as tobramycin/gentamicin. Half-life was calculated using the elimination constant calculated from the 2 levels obtained. If a dose adjustment was required, the same monitoring process was repeated after the changes were made. For patients on once-daily dosing with half-life less than 2 hours, the interval was changed to thrice daily, whereas those who had a drug half-life of 2 hours or more remained on once-daily dosing. A 2-hour half-life was chosen as a surrogate marker of a drug-free interval, which is estimated to be 6 to 8 hours.
After ensuring that drug levels were within the pharmacokinetic goals, 18-hour concentrations for patients on daily dosing were repeated once weekly till the end of the antibiotics course. Patient serum creatinine and blood urea nitrogen (BUN) values were measured at baseline and were monitored weekly while receiving aminoglycoside therapy.
The project was reviewed by the University of Michigan Institutional Review Board (IRB) and was deemed exempt by the IRB.
Statistical Analysis
We used 2 independent-samples t tests and the χ2 test to characterize samples and detect differences in the baseline characteristics and the pharmacokinetic parameters for the once-daily dosing group and the group that required a shift from once to thrice daily. A mixed model, with clustering by patient, was used to detect associations between patient characteristics and drug half-life. Logistic regression was then used, with clustering by patient, to determine which patient characteristics could specifically predict the likelihood of achieving a drug half-life of 2 hours or more (the key determinant for dosage switching).
A 2-tailed α level of ≤.05 was considered statistically significant. All analysis was done using SAS 9.4 (SAS Institute Inc, Cary, NC).
Results
A total of 119 patient encounters for 52 patients were included in the study; 40% of patients had more than 1 encounter (mean = 1.9 encounters; SD = 1.80; range = 1-12). Of the 119 encounters, 98 (82.4%) started with once-daily dosing. The remainder were started on thrice-daily dosing because of family or primary pulmonologist preference. The most commonly used aminoglycoside antibiotic was tobramycin (89.8%) followed by amikacin and gentamicin (used in 6.1% and 4.1%, respectively). Patients who were able to maintain once-daily dosing differed from patients who required a switch from once-daily to thrice-daily dosing in some baseline measures as well as in pharmacokinetic parameters. Table 1 illustrates the demographics of the patient population. The table shows the 2 groups according to their ability to stay on the EID or having to switch to the thrice-daily dosing. The 2 groups differed in terms of baseline forced expiratory volume in 1 s (66.5% vs 80.1%, P = .01) and FEF 25-75 (46.9% vs 76.2%, P = .02). In addition, the once-daily dosing group was older (mean age = 15.7 years vs 8.6 years, P < .0001) and had higher BMI (19.0 kg/m2 vs 16.5 kg/m2, P < .0001).
Patients’ Characteristics.

Abbreviations: BMI, body mass index; FEV1, forced expiratory volume in 1 s; FEF 25-75, forced expiratory flow from 25% to 75% of vital capacity.
Table 2 shows the pharmacokinetic parameters for the 2 groups. The once-daily dosing group had higher mean 18-hour level (0.16 vs 0.06 µg/mL, P = .003), higher mean half-life (2.2 vs 1.9 hours, P = .02), higher mean area under the curve (AUC; 105.7 vs 77.6 mg h/L, P = .01), and lower mean elimination constant (0.33 vs 0.36 hour-1, P = .01). They differed (approaching significance) in mean maximum drug concentration (Cmax) at 1 hour after infusion (29.6 vs 23.7 µg/mL, P = .06) and mean AUC:MIC ratio (79.8 vs 59.8, P = .07). No statistically significant difference was found between the 2 groups in mean Cmax:MIC ratio (22.3 vs 18.8, P = .21).
Pharmacokinetic Parameters.
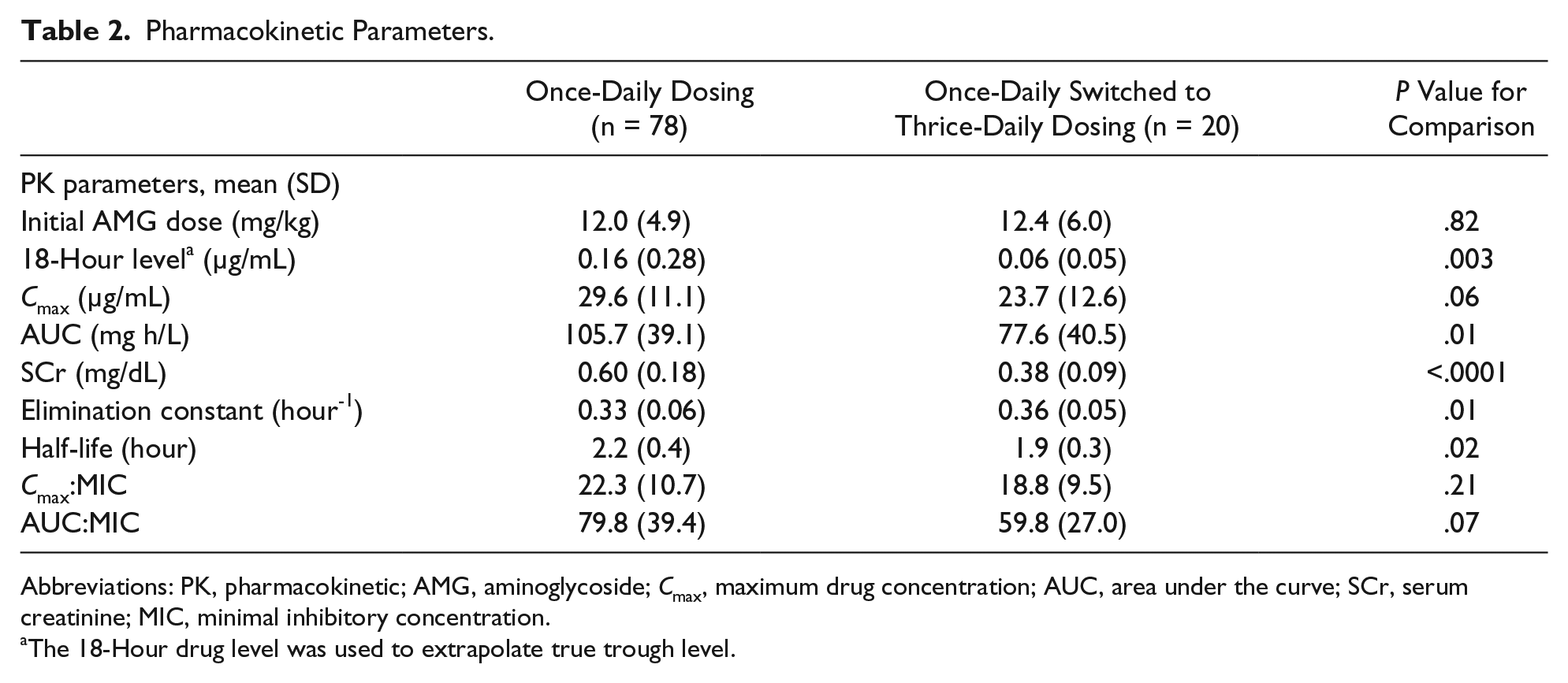
Abbreviations: PK, pharmacokinetic; AMG, aminoglycoside; Cmax, maximum drug concentration; AUC, area under the curve; SCr, serum creatinine; MIC, minimal inhibitory concentration.
The 18-Hour drug level was used to extrapolate true trough level.
Mixed-model analysis using SAS PROC MIXED with random effects was used to account for the correlation between measures from different encounters for the patients who were admitted more than once to evaluate whether patient’s sex, age on admission, or BMI percentile were significant predictors of drug half-life. Results are shown in Table 3. Patient’s age on admission was the only significant predictor of drug half-life. Older age was associated with a longer drug half-life (P = .05).
Results of Mixed Model Analysis for Predicting Drug Half-life for Repeat Admissions.
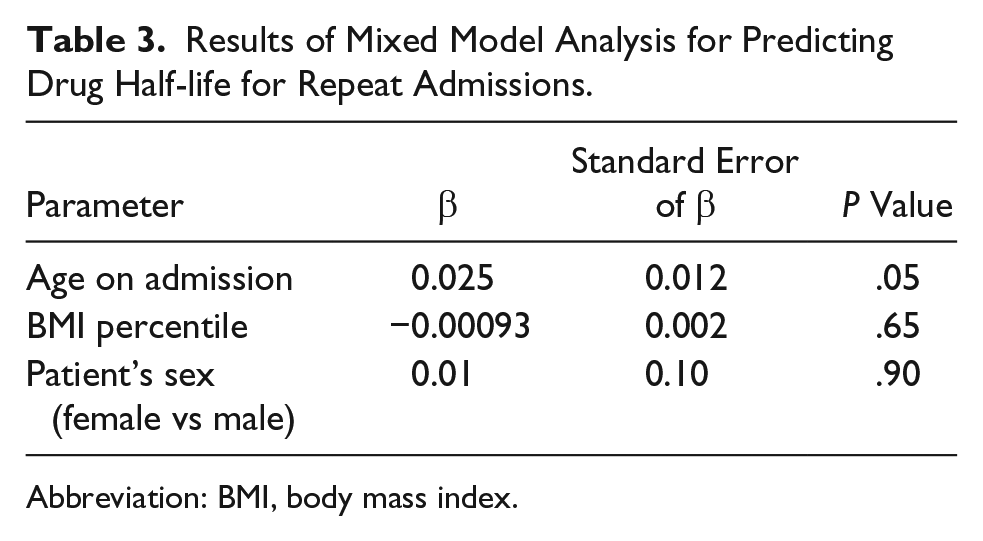
Abbreviation: BMI, body mass index.
Expansion on the mixed-model analysis was done to establish an age threshold for using once-daily dosing. SAS PROC GENMOD was used to conduct logistic regression to model the likelihood of achieving a drug half-life of 2 hours. We used repeated measures to account for clustering of multiple admissions for some of the patients. Instead of using a continuous measure of age, we used an age cutoff variable as a predictor, along with patient’s BMI percentile and sex. The model was repeated using different age threshold variables (eg, ≥6 vs <6 years of age) until the threshold that indicated a statistically significant increase in the odds of having a half-life at 2 hours or higher was detected. Model results are shown in Table 4. It shows that patient’s age was the only predictor of having a drug half-life of 2 hours or higher.
Results of the Logistic Regression Model for Predicting Odds of Having a Half-life of 2 Hours or More.

Abbreviation: BMI, body mass index.
Discussion
Earlier studies have shown that once-daily aminoglycoside dosing is as effective and potentially safer compared with conventional thrice-daily dosing.6,13 Prescott and Nagel 6 reviewed once-daily aminoglycoside pharmacokinetic studies in both children and adults. They concluded that tobramycin pharmacokinetic parameters for once-daily dosing are relatively similar in children and adults. However, it was noted that pediatric CF patients generally have increased clearance and decreased AUC, compared with adults with CF.6,9,10,14-21 These findings were similar to ours, which showed that older patients had statistically significantly higher Cmax and AUC. They also had slower clearance of tobramycin, as demonstrated by lower elimination constant and longer half-life.
Pharmacokinetic studies suggest that a Cmax:MIC ratio of 8 to 10 is an optimal target to enhance bacterial killing and maximize the postantibiotic effect (PAE).6,22-25 PAE indicates the persistent suppression of bacterial growth that occurs after the drug has been cleared. The use of once-daily aminoglycoside enhances the probability that optimal Cmax:MIC ratio is achieved. 6 On the other hand, it may result in a longer drug-free interval, or the time for which the antibiotic concentration is below the MIC. If the drug-free interval significantly exceeds the PAE, there is a concern for bacterial regrowth and, potentially, the development of resistance.13,26 In this project, a half-life of 2 hours was utilized as a surrogate marker of a drug-free interval of approximately 6 to 8 hours.
This project demonstrated that the recommended target Cmax:MIC ratio was achieved in all patients treated with a once-daily regimen regardless of age. However, of the 98 encounters that were started on EID, 20% were changed to thrice-daily dosing based on the short half-life. Of these patients, 75% were younger than 10 years of age, suggesting that the younger the child, the more likely he or she is to have a longer drug-free interval. Additionally, early pharmacokinetic studies suggested an AUC:MIC ratio of 80 to 110. 6 In our project, that was achieved only in patients older than 14 years. The AUC:MIC ratio was lower in patients 5 to 14 years old, with 59% of patients in this age range failing to achieve an AUC:MIC ratio of 80 to 110, which may suggest that younger patients have a drug-free interval that may exceed the optimal PAE.
Once-daily dosing may promote less bacterial resistance, given that Cmax:MIC ratios are achieved.6,27 In CF patients with rapid renal elimination, there could be a prolonged drug-free interval, which is a potential disadvantage given the possibility of development of bacterial resistance.
Burkhardt et al 13 reported an increase in tobramycin MIC for P aeruginosa between the start and end (day 14) of therapy in 33 adult patients treated for CF exacerbation with a β-lactam antibiotic in combination with tobramycin 10 mg/kg once daily (17 patients) or 3.3 mg/kg thrice daily (16 patients). 13 The mean tobramycin MIC in the once-daily group increased by 6.8 mg/L (P = .034), whereas it increased by 0.6 mg/L (P > .05) in the thrice-daily group. Furthermore, the percentage of patients with tobramycin MIC ≥16 mg/L, which indicates bacterial resistance, increased from 5.9% to 29.4% in the once-daily group, compared with an increase from 12.5% to 18.8% in the thrice-daily group. Master et al 26 reported similar findings in 44 adult and pediatric CF patients treated for CF exacerbations over a 2-year period, which included multiple admissions; 23 patients were treated with tobramycin monotherapy, and 21 patients were treated with ceftazidime plus traditional thrice-daily dosing of tobramycin. The mean number of intravenous antibiotic courses was similar between the 2 groups: 3.0 and 3.1 courses in the once-daily and thrice-daily dosing groups, respectively. The tobramycin MIC increase was more significant for the once-daily tobramycin monotherapy group (11.5 to 19.4 mg/L, P = .014) compared with the conventional dosing group (13.2 to 18.4 mg/L, P = .076).
CF patients are at risk for developing nephrotoxicity and ototoxicity, given the need for repeated aminoglycoside use.6,28,29 Because the overall survival of CF patients has been improving significantly over the past few decades, the risk of such toxicities may be even higher because of more aminoglycoside exposure.
It was reported that the use of EID may be less nephrotoxic in the long term for CF patients.28,30 This is because aminoglycoside uptake by the kidney (specifically the proximal tubules) is saturable, 30 and the renal cortical accumulation is expected to be lower with EID compared with thrice-daily dosing. 28
Many studies have evaluated the risk of auditory and vestibular ototoxicity related to aminoglycoside use in CF patients.9,31-36 Overall, no significant difference was noted in the risk of ototoxicity among CF patients treated with EID versus thrice-daily dosing. However, Mulheran et al 37 reported a trend favoring EID treatment, with less ototoxicity as indicated by high-frequency audiometry in both adults and pediatric patients.
In conclusion, this project revealed that aminoglycoside clearance is higher in younger patients, and therefore, it may be challenging to achieve desirable aminoglycoside half-life with a once-daily dosing regimen in younger children. On the other hand, higher aminoglycoside clearance may indicate a lower risk of antibiotic accumulation and toxicity. In addition, a prolonged drug-free interval may have the potential disadvantage of contributing to antimicrobial resistance. In our institution, this study resulted in changing the cutoff age of starting EID to 5 years of age when treating acute CF exacerbations to ensure achieving adequate therapeutic levels while avoiding toxicity and the potential disadvantage of bacterial resistance emergence.
One limitation of this study is that the project was not designed with the rigors of a pharmacokinetic study; therefore, data collection may be affected by sampling and timing errors, which in turn can affect calculation of pharmacokinetic parameters. Large-size studies are needed to further evaluate aminoglycoside pharmacokinetics in different age groups and to evaluate the emergence of resistance with EID of aminoglycosides.
Author Contributions
KHS, the primary author, contributed to the conception and design; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JMD contributed to the conception and design; contributed to acquisition and interpretation of data; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
JS contributed to the conception and design; contributed to analysis of data; drafted the manuscript (statistical part); critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SZN contributed to the conception and design; contributed to acquisition, analysis, and interpretation of data; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.