
Abstract
As US residency programs are increasingly offering global health electives for their trainees, there is a growing call for these opportunities to include bidirectional exchanges—where residents from both the US and international partner institutions rotate at the other’s site. Curricular, logistical, and funding challenges of hosting residents from an international site may be barriers to developing these programs. In this report, the authors describe an 8-year experience of a US institution hosting residents from a resource-limited international partner and provide a framework for others institutions to develop bidirectional exchanges. They also report the visiting international residents’ perceptions of the impact of the exchange on their clinical practice, teaching, career paths, and their home institution.
Background
To meet the growing demand for global health (GH) education, US residency programs have increasingly developed international opportunities for their learners.1-3 Most of these experiences are global health electives (GHE) where residents from resource-rich settings travel to resource-limited settings to participate in education and clinical care.1,4-8 While benefits for US-based trainees participating in GHE have been shown, there is a body of literature describing the burden they can place on international host institutions and inequitable relationships between partnering institutions.9-17 In 2010, the Working Group on Ethics Guidelines for Global Health Training (WEIGHT) developed best practice recommendations to address these ethical concerns. 18 To support reciprocity between partners, they recommended bidirectional exchanges, which offer trainees from both institutions the opportunity to experience medicine in each other’s environments. The WEIGHT guidelines do not, however, discuss the logistics or solutions to overcoming the challenges of implementing such exchanges. 17
Descriptions of bidirectional exchanges of resident learners are sparse, and when reported have largely focused on the logistics and outcomes from sending learners from the resource-rich to resource-limited setting with little detail provided regarding the logistics of hosting of international residents.19-21 The few published descriptions of hosting international colleagues—notably medical students or junior faculty but not residents—primarily focus on perceptions of the visiting international trainees regarding the value of the experience, but provide little description of curriculum development or how to overcome logistical challenges in hosting international trainees.22,23 Recently, Umoren and colleagues described a bidirectional exchange between Indiana University and Moi University in Kenya. This article addresses many of the logistics necessary for hosting international residents with much of the focus on predeparture preparation, including visa requirements. They also reported immediate gains in residents’ knowledge. 24
The aim of this article is twofold. First, we provide a comprehensive framework for other institutions considering hosting international residents and discuss solutions to challenges that may be encountered in the process. Second, we share the international residents’ perceptions of how participating in the exchange has affected their clinical practice, teaching, career paths, and their home institution. Informed by our 8-year experience with a bidirectional exchange of residents between a resource-rich and resource-limited partner site, we outline the logistics of hosting the residents, describe their role and expectations while visiting, and report their feedback on returning to their home institution.
Program Description and Logistics
The Bugando Medical Centre–Lurie Children’s Partnership
Context
In 2006, a memorandum of understanding was signed between the McGaw Medical Center of Northwestern University’s pediatric residency program based at the Ann & Robert H. Lurie Children’s Hospital of Chicago (formerly Children’s Memorial Hospital) and Bugando Medical Centre (BMC), a consultant, referral, and teaching hospital affiliated with the Catholic University of Health and Allied Sciences located in Tanzania’s second largest city, Mwanza. The memorandum outlined goals of the bidirectional exchange including the opportunity for residents from both institutions to gain educational, clinical, and cultural experiences while rotating for 4 weeks at the other’s site. The opportunity to participate has been offered to all pediatric residents in good standing during the second postgraduate year at BMC and third postgraduate year at Lurie Children’s. From 2006 to 2014, 130 Lurie Children’s residents (46% of those eligible) and 20 BMC residents (59%) have participated.
(Note 2 authors [SB at Lurie Children’s and CM at BMC] oversaw the initial development and implementation of the exchange; MP served as the faculty director of the exchange until 2013).
The BMC Resident Rotation: Logistics and Rotation Experiences
Both institutions provided input in the development of experiences that could be offered to the visiting BMC residents with the goal of providing as equitable an experience as possible. Three common components of the resident experience were identified: clinical, educational, and cultural. These formed the framework for the rotation experiences provided for the visiting residents (Table 1).
Components of Visiting International Residents Curriculum.

Abbreviations: NICU, neonatal intensive care unit; PICU, pediatric intensive care unit; ED, emergency department.
Clinical exposure
Whereas US-based residents may be able to obtain temporary licensure from host governments to participate in patient care during their GHE, there are governmental and often institutional regulatory challenges in doing the same for international residents visiting US institutions. Given these constraints, the BMC resident rotation focuses on clinical shadowing opportunities tailored to residents’ interests. Currently, they spend 1 week on a general pediatric ward team, 1 week shadowing in the intensive care units and emergency department, 1 week in specialty clinics of their choosing (solicited via email prior to their arrival), and 1 week to revisit any areas of interest that emerge.
Educational opportunities
While at Lurie Children’s, BMC residents function as both learners and educators. They are encouraged to participate in all educational conferences. Each BMC resident is required to present a topic of their choosing at a pediatric conference, which parallels the requirement that Lurie residents facilitate an educational session while at BMC. They receive faculty assistance in preparing the presentation and formal feedback afterwards. Residents also receive training from the Lurie Children’s librarian on answering clinical and research questions online.
The BMC residents participate in a simulation curriculum including weekly private sessions where they participate in a medical scenario and spend time in debriefing, discussing teamwork and communication skills. In addition to these sessions, they also join Lurie Children’s residents and medical students in their standing weekly simulation sessions throughout their rotation.
Culture
BMC residents are encouraged to engage in cultural offerings while in Chicago. Lurie Children’s residents and faculty host meals and museum outings and faculty donate tickets to sporting events. In addition, a pediatric GH educator provides opportunities for the residents to debrief challenges and culture shock.
Logistical Arrangements and Funding
Implementation of the exchange has required careful planning and overcoming funding and logistical challenges. A summary of these challenges and our solutions is found below with details in Table 2.
Challenges and Solutions of Hosting Visiting International Residents.

Abbreviations: FTE, full-time equivalent; BMC, Bugando Medical Centre; TB, tuberculosis; CXR, chest x-ray.
Administrative support
Initially, Lurie Children’s chief residents were responsible for coordinating the visiting BMC residents’ experience. After 5 years, Lurie Children’s provided 0.1 full-time equivalent for a faculty member to be the Director of GH Education and oversee the exchange. Funding was provided for this faculty member to travel to BMC annually to maintain relationships, perform needs assessments, obtain feedback, and pilot curricula.
Funding
As part of the effort to offer an equitable exchange, BMC residents have access to the same travel funding offered to the Lurie residents: a grant from the Lurie Children’s Department of Pediatrics, currently $2500 per resident. This funding began as a seed grant from private donors; once the initial funds were exhausted, the Department of Pediatrics began providing the financial support. This funding has been sufficient to cover the cost of the flights from Tanzania, housing, a public transportation card, a preloaded meal card for lunches at the hospital, and a prepaid cell phone.
Housing/meals
Early on, BMC residents stayed in residents’ or faculty members’ homes. This was not sustainable and BMC residents now stay at a youth hostel, which is low cost and includes breakfast and many dinners. BMC residents pay for their own dinners when not provided by the hostel or being hosted by residents or faculty.
Visas/health screening
Lurie Children’s provides a formal letter of invitation for BMC residents to use in their visa applications, which must be granted prior to travel. Prior to their first day of shadowing, occupational health reviews vaccine records supplied by the BMC residents and provides any needed immunizations based on hospital policy (typically influenza vaccine has been deficient and needed on arrival). The residents are also screened for tuberculosis. Occupational health covers the costs for screening and vaccines.
Orientation
In an attempt to provide clear expectations and anticipate any challenges, the Director of GH Education provides an in-depth orientation after picking the visiting residents up at the airport. Based on feedback from the BMC residents, this orientation has evolved to include an overview of their schedule with expected roles, a discussion of cultural differences likely to be encountered, logistical information including a review of interpreting the maps of the surrounding area and how to use public transportation, and an overview of how to make and receive international phone calls. In addition, a written orientation packet containing all orientation information, including contact numbers, is provided.
Evaluation
BMC Resident Perception
To better understand the BMC residents’ perceptions of the impact of participating in the exchange, we administered a survey to participating BMC residents. The survey was designed by 2 authors (MP and SB) and reviewed by a third (SG) as well as a faculty pediatrician from BMC. The survey included questions related to the residents’ perceived impact of participating in the exchange on their clinical practice, teaching, and career path as well as the impact on their home institution. Institutional review board approval was obtained from both institutions, and the survey was sent via email in July 2012 to the 13 BMC residents who had participated in the exchange up to that point. Participation was voluntary and anonymous.
Ten residents (response rate 77%) completed the survey. Responses to questions were not required; therefore, the response rate varied by question. Every respondent reported the experience positively affected their ability to answer clinical questions on return to Tanzania most often commenting on broadening their differential diagnosis. The majority (7/9; 78%) indicated the experience affected their patient management in Tanzania citing examples such as managing viral croup and newborn resuscitation. Most respondents (6/7; 86%) reported improvement in their teaching including changes in their approaches to giving feedback and adapting to their learners. Half of the residents (5/10; 50%) reported that the exchange changed their career path with several indicating interest in fellowships.
Most residents (7/9; 78%) noted changes at BMC they attributed to the exchange with examples including initiation of morning report and sign-out, increased support from faculty in patient management, increased involvement of students in case presentations, and improved communication. Respondents also noted an impact on how they viewed and interacted with US residents including a new understanding of the challenges the US residents face when visiting BMC. Themes from residents’ survey responses with representative quotes are reported in Table 3.
Themes From Survey Responses From BMC Residents on Participation in the Exchange.
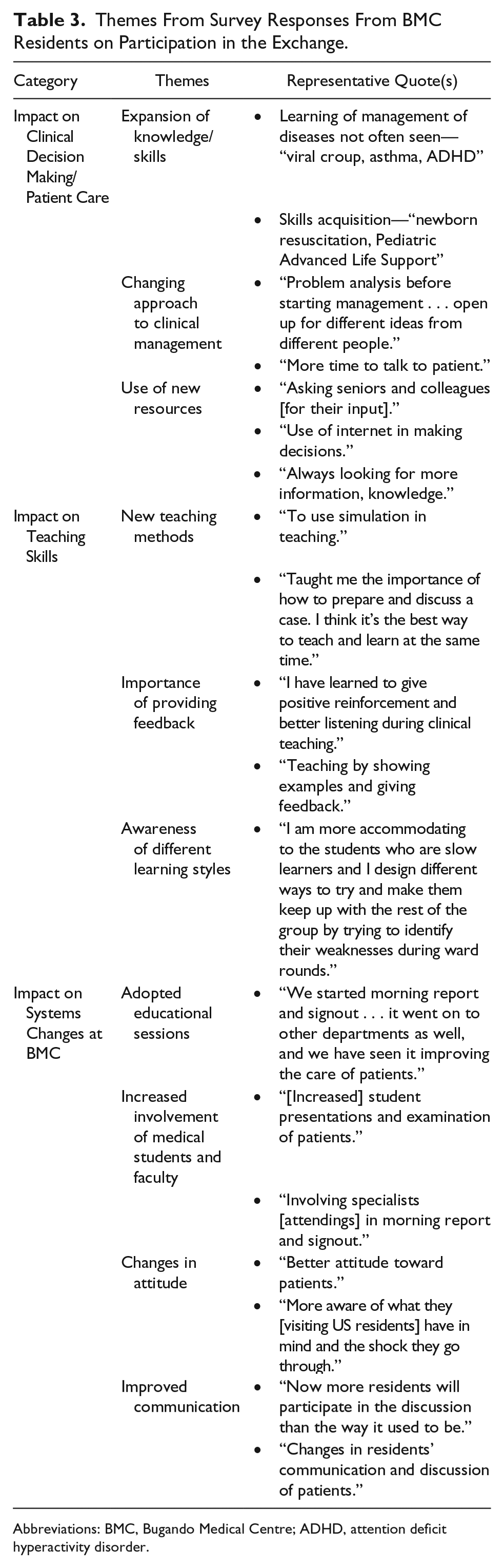
Abbreviations: BMC, Bugando Medical Centre; ADHD, attention deficit hyperactivity disorder.
Lessons Learned
In addition to the BMC residents’ overall positive perceptions of participating in the exchange, we have learned several important lessons about hosting international residents as part of a bidirectional exchange.
Initially, there were concerns it would be difficult to provide a meaningful experience for BMC residents given their observer status as this was a clear area where we were not able to offer an equitable experience to what Lurie residents are offered at BMC. We have learned over the past 8 years, however, that it is possible to meaningfully integrate BMC residents into the clinical and educational environment. Keys to this integration include tailoring the experience to their areas of interest, listening and willingness to respond to their needs, emphasizing their roles as both teachers and learners, and incorporating nonclinical experiences.
We also learned that BMC residents become critical agents of change fostering an exchange of knowledge, skills, and attitudes between Lurie Children’s and BMC. In addition to personal changes to their clinical practice and teaching skills, BMC residents reported changes in their attitudes, with better attitudes toward patients and toward visiting US residents, with several describing being more aware of the culture shock and challenges they encounter when visiting BMC. In addition to the systems changes at BMC reported in the survey such as the implementation of morning report, BMC faculty also report a “trickle up effect” where new knowledge and skills gained by residents have spread through department, such as how to do an induced sputum collection for diagnosis of tuberculosis. Similarly, hosting residents from BMC provides exposure to important GH topics for residents and faculty at Lurie Children’s through the unique and valuable perspective provided by BMC residents who often contribute to differential diagnoses and prompt interesting discussions about how a disease may be managed with fewer resources or different cultural views of medicine.
The exchange has also led to the development of new partnership-based educational programs. Based on BMC residents’ positive feedback about simulation, BMC faculty asked if Lurie Children’s faculty could develop a simulation curriculum for use at BMC. This led to the development of simulation cases using BMC’s management guidelines. Lurie Children’s residents who will rotate at BMC are trained to lead these cases for BMC students using an inflatable mannequin, and have now led sessions for hundreds of BMC students.
We have found that, as with many institutional initiatives, the greatest challenge was getting started. After the first year, much of the logistical work was done and initial challenges overcome. However, the ongoing solicitation of feedback, through systematic collection from BMC residents and having Lurie Children’s Director of GH Education visit BMC annually, as well as a willingness to respond is essential sustaining the exchange. The ongoing support of both institutions’ Departments of Pediatrics is also critical. For BMC, this includes committing to operating without as many as 3 of their 5 second-year residents for a month, and for Lurie Children’s in addition to the commitment to the educational initiatives, there is an ongoing financial commitment that has been essential to overcoming the common financial barrier to many programs implementing bidirectional exchanges.19,23,24 However, even with this financial support, additional fundraising is likely needed to ensure sustainability as BMC residents reported an average out-of-pocket cost of $765 (range of $300-$1120), with 33% (3/9 respondents) indicating this had a negative impact on their finances. This financial burden is reported by other intuitions involved in bidirectional exchanges, and solutions have been suggested to fill the gaps ranging from fundraising by host residents to pursuing grant support.19,23,24
One concern is the possible negative outcome of an increasing desire by residents to pursue future opportunities outside their country contributing to “brain drain.” 25 Recently, Abedini et al reported that 85% (28/33) of Ghanaian medical students who participated in a rotation at the University of Michigan felt more inclined to pursue training outside their home country after the rotation. 22 We have not yet seen this occur with the BMC residents as 18 of the 20 BMC residents who participated in the exchange are currently practicing in Tanzania, with 2 having pursued fellowship. Similarly, Bodnar et al did not find that junior Ugandan faculty who participate in an exchange at Yale were more likely to leave Uganda than their peers. 23 It is possible that the greater inclination of the medical students to pursue training outside of their home institution after participating in an exchange compared to residents or junior faculty reflects the fact that completing residency training outside of the country where one attended medical school is often sufficient to obtain medical licensure in the new country. In the United States, for example, residency completed in a foreign country does not typically count toward licensing requirements.
Limitations to our approach include that it reflects a single exchange and small sample size and reports residents’ perceptions of the impact of participating in the exchange. Follow-up studies are needed to measure actual changes in residents’ clinical practice, teaching, and career paths that may result from participating in the exchange as well as changes at Lurie Children’s and BMC.
Conclusion
Bidirectional exchanges can make an important contribution to reciprocity between international partners. Our experience suggests that challenges related to hosting international residents can be addressed creating the potential to positively influence participating residents’ clinical and teaching skills as well as both partner institutions.
Author Contributions
MBP: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SPG: Contributed to conception and design; contributed to analysis and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CRM: Contributed to conception; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SMB: Contributed to conception and design; contributed to acquisition and analysis; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Acknowledgements
The thank Dr Antke Zuechner, Dr Christian Schmidt, Dr Damas Mwizamholya, and Dr Adolfine Hokorro from the Department of Pediatrics at BMC as well as Dr Sharon Unti and Dr Ellen Chadwick at Lurie Children’s for their ongoing support of the exchange. They also thank Dr Margaret Shane who now oversees the program at Lurie Children’s, as well as all of the residents from both institutions who have participated in the program.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The initial funding to start the program came from donors Gregory Sachs, Jim Harisiades, MPH, and Jon and Lois Mills.