
Abstract
Background. Acute bronchiolitis infection during infancy is associated with an increased risk of asthma later in life. The objective of this study was to determine if inhaled steroids are effective in preventing the development of recurrent wheeze or asthma following acute bronchiolitis. Methods. Multiple databases and bibliographies of selected references were searched. Inclusion required (a) a randomized controlled trial of inhaled steroids and control group, (b) at least 2 weeks duration of therapy started during the acute phase of disease, and (c) identification of the rate of recurrent wheeze or asthma at least 6 months after therapy. Results. Of 1410 studies reviewed, 8 reports were included in this meta-analysis (748 patients). The overall odds ratio for developing recurrent wheeze or asthma with treatment versus without treatment was 1.02 (95% confidence interval = 0.58-1.81). Conclusions. A course of inhaled steroids after acute bronchiolitis is not effective in preventing recurrent wheeze or asthma.
Introduction
Acute bronchiolitis, a viral respiratory infection of infancy, is the most common cause of hospitalization for infants <23 months of age. 1 A longitudinal birth cohort study in the United Kingdom found that 38% of children with respiratory syncytial virus (RSV) bronchiolitis developed asthma. 2 While the association between bronchiolitis and recurrent wheeze or asthma is well documented, the pathophysiology of this relationship remains unclear. It has been suggested that early infection with RSV or other respiratory viruses produces chronic inflammatory changes and increased airway hyperresponsiveness. 3
The role for inhaled corticosteroid therapy in acute bronchiolitis is controversial. Inhaled corticosteroid therapy has not been shown to be effective in the treatment of acute bronchiolitis and is not currently recommended for this indication. 4 The efficacy of inhaled corticosteroids to prevent recurrent wheeze or asthma after acute bronchiolitis is unclear. 1 The results of multiple studies have not been consistent. A Cochrane review from 2007 failed to make a definitive recommendation regarding inhaled corticosteroids and recurrent wheeze due to small study sizes and inability to pool all data. 5 This review included 5 studies with follow-up data for 358 infants; however, only pooled data from 3 studies (119 infants) were used to examine the impact on recurrent wheeze. 5 Several randomized, controlled trials were excluded from the 2007 Cochrane review because control patients did not receive a placebo and were largely unblinded. 5
Since that review, a large, randomized, placebo-controlled trial examining the efficacy of inhaled corticosteroids on subsequent recurrent wheeze after bronchiolitis has been published. 6 The present systematic review and meta-analysis includes data published since the 2007 Cochrane review as well as the randomized, controlled trials without placebo control previously identified.5-9
Objective
The purpose of this systematic review and meta-analysis is to determine if inhaled corticosteroid therapy administered to infants after acute bronchiolitis reduces the rate of subsequent recurrent wheeze or asthma.
Methods
Protocol
This study followed the guidelines described in the Preferred Reporting Items for Systemic Reviews and Meta-Analyses (PRISMA). 10
Eligibility
To be included in this review, studies needed to meet the following criteria: (a) subjects less than 24 months of age with clinically diagnosed, acute bronchiolitis and without existing cardiopulmonary disease; (b) a randomized, controlled design where the experimental group received inhaled corticosteroid therapy and a contemporary control group was identified; placebo administration was not required; (c) therapy started during the acute phase of the infection and was administered for at least 2 weeks; and (d) final outcome assessment was a minimum of 6 months after the completion of treatment.
Sources
The following databases were searched: PubMed (1966 to January 2015), Cochrane Central Register of Clinical Trials, Cochrane Database of Systematic Reviews, EMBASE, and ProQuest COS Conference Papers Index. Bibliographies of selected studies were also reviewed. Contact with the author of one study was attempted for additional clarification. 11
Search
The search terms used were “bronchiolitis,” “inhaled budesonide,” “inhaled steroid,” and “inhaled corticosteroid.” No language filters were used, but an English abstract was required to be included for review.
Study Selection
Reports were assessed by 2 authors using the eligibility criteria detailed previously. When articles appeared to report the same patient sample, the report with the follow-up period most similar to the other included studies was selected. Disagreements about study eligibility were determined by a third author.
Data Extraction
Data extracted from each report included number of patients, inclusion and exclusion criteria for patients, patient ages, corticosteroid used and dosage, treatment length, follow-up period, and country of origin. The primary outcome was asthma diagnosis and/or recurrent episodes of wheeze subsequent to the acute episode of bronchiolitis as diagnosed by a physician or as recorded in a symptom diary evaluated by a study investigator. Data were extracted independently by one author and verified by a second author.
Risk of Bias in Individual Studies
To decrease the risk of bias in individual studies, only studies that were randomized and controlled were included in this meta-analysis.
Summary Measures
The primary outcome measure was the odds ratio of developing recurrent wheeze or asthma after bronchiolitis with or without treatment using inhaled corticosteroids.
Synthesis of Results
The number of subjects experiencing asthma or remote wheeze and the total number of subjects reported in each group for each study were recorded. The odds ratio for each study was calculated and the overall odds ratio was determined using the DerSimonian-Laird estimator for random effects. 12 Residual heterogeneity among studies was estimated by τ2 and tested by Cochrane’s Q test. 13 P values <.05 were considered significant. Interstudy heterogeneity was estimated by I2. 14 To determine the impact of individual studies on the overall outcome, composite odds ratios were reiteratively calculated following the stepwise exclusion of each study. Publication bias was estimated by the method of Galbraith. 15 All analyses were performed in R using the “metaphor” package. 16
Risk of Bias Across Studies
There was variability in the reporting of outcomes in each study, which may be a source of bias when outcomes are combined. The outcomes ranged from physician-diagnosed asthma to respiratory symptoms as noted in parental diary.
Results
Study Selection
The literature search is summarized in Figure 1. A total 1410 references were found by searching PubMed, Cochrane Central Register of Clinical Trials, Cochrane Database of Systematic Reviews, EMBASE, and ProQuest COS Conference Papers Index. Two additional studies were found by searching the bibliographies of selected studies. After studies were screened by title and abstract, 16 reports remained for full text screening. Eight of these reports were excluded. Four reports duplicated the subject sample and reported follow-up periods outside of inclusion criteria.17-20 Two studies included subjects with recurrent wheeze who were treated after the acute phase of an episode of bronchiolitis.21,22 The treatment period failed to meet inclusion criteria in 1 study. 23 One study was excluded after communications with the author clarified that the study was not randomized. 11 The remaining 8 reports form the basis for this review.6-9,24-27

Literature search.
Study Characteristics and Outcomes
The characteristics of each study are shown in Table 1. The total sample included 748 children, ranging in age from 0 to 24 months. For therapy, 5 studies used budesonide,7,9,25-27 2 used beclomethasone,6,8 and 1 used fluticasone propionate. 24 The duration of therapy ranged from 2 weeks to 3 months, and follow-up periods ranged from 6 months to 3 years.
Characteristics of Included Studies.

Treatment was started at admission and ended 2 weeks postdischarge up to maximum of 21 days.
Study outcomes are summarized in Table 2. In 3 studies symptom diaries kept by parents were used to determine subsequent episodes of wheezing or asthma.6,25,27 In 3 studies subsequent wheeze or asthma was identified when the patient sought 24 or received8,26 medical intervention. In 2 studies the outcome was determined by physician diagnosis 9 of asthma or current asthma medication. 7
Outcome of Recurrent Wheeze or Asthma by Study.

Data Synthesis
The individual and overall odds ratios are summarized in Figure 2 and Table 3; odds ratios greater than 1 support the use of inhaled steroids. Heterogeneity was not statistically significant (Q = 13.6, P = .06) and less than half of the variability seen among the 8 studies was attributable to interstudy variability (τ2 = .29 ± .35; I2 = 48.4%). When all of the studies were considered, the overall odds ratio was 1.02 (95% confidence interval = 0.58-1.81). By sensitivity analysis, the overall odds ratio ranged from 0.86 to 1.19; in all cases, the 95% confidence intervals included 1. The radial plot for publication bias is shown in Figure 3. The effect size to study size is within the expected range, suggesting that publication bias is unlikely.
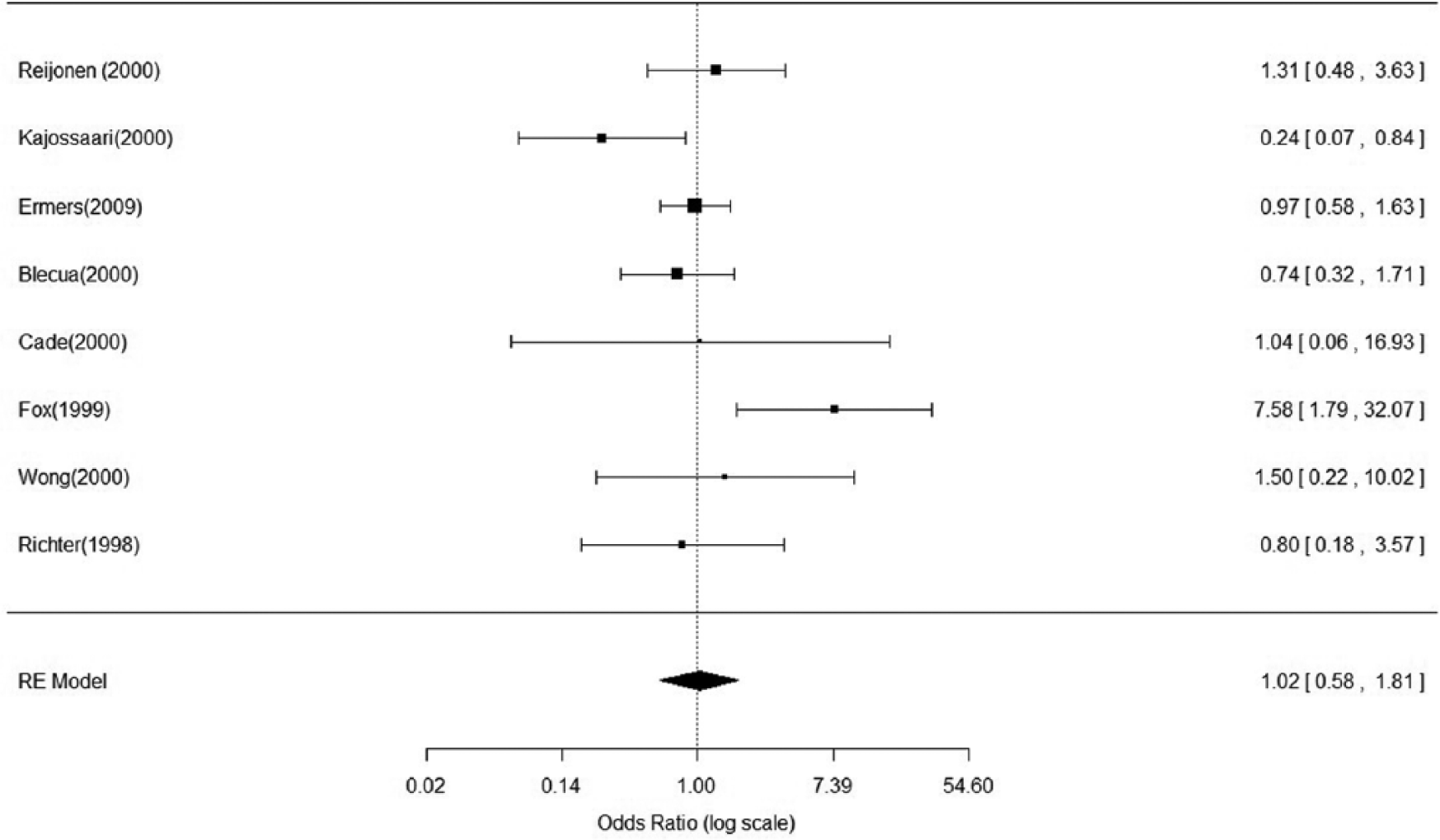
Forest plot.
Sensitivity Analysis: Overall Odds Ratio With One Study Removed.

Abbreviations: OR, odds ratio; LCL, lower confidence limit; UCL, upper confidence limit.

Galbraith plot.
Discussion
Summary of Evidence
The present systematic review and meta-analysis demonstrates that a course of inhaled steroids after acute bronchiolitis is not effective in preventing recurrent wheeze or asthma. Although a Cochrane review in 2007 came to a similar conclusion, it was unable to make a strong clinical recommendation due to the small number of subjects included in the review. 5
Limitations
There are a number of limitations to the conclusions drawn by this study. First, the type of inhaled steroid and the length of treatment were not uniform across all studies and whether one regimen was more effective than another was not analyzed. Second, the inclusion and exclusion criteria for patients across studies were not the same. For example, some studies included patients on mechanical ventilation 6 or who previously wheezed. 9 Other studies did not explicitly exclude preterm infants,6,8,26,27 a recognized risk factor for respiratory disease, particularly asthma. 28 Third, the measurement of the primary outcome varied from study to study. In some studies asthma or recurrent wheeze was based on a physician diagnosis while in other studies it was based on symptom diaries kept by parents. Fourth, the follow-up period varied from study to study. Six of the 8 trials had a follow-up period of 1 year or less producing a study population less than 4 years of age and possibly underestimating the endpoint incidence.6,8,24-27 Conversely, 2 population-based studies demonstrated that persistence of asthma into adulthood was associated with onset of wheezing at a young age. 29 Last, as opposed to the Cochrane review, several studies were included that did not use placebo for the control group.5,7-9 Due to the lack of placebo control, there is a risk for induction of bias in these studies. Two of these studies showed no differences between the treatment and nontreatment groups.8,9 One of the 3 studies did show treatment was effective. 7 However, based on the sensitivity analysis the inclusion of these studies did not significantly affect the overall outcome.
Conclusions
The evidence from the present meta-analysis does not support the use of inhaled corticosteroids for the prevention of recurrent wheeze or asthma after acute infantile bronchiolitis. Given the size of the analysis, a strong recommendation can be made against the use of such interventions.
Footnotes
Acknowledgements
Thank you to Karen Burstein for help in performing the database searches. Thank you to B. Hesselmar for responding our inquiries about their study.
Author Contributions
PG performed the database searches, carried out the initial data extraction, drafted the initial manuscript and approved the final manuscript. SCA performed the statistical analysis, reviewed and revised the initial manuscript and approved the final manuscript as submitted. MD conceptualized and designed the study, did a secondary database search, reviewed all abstracted data, reviewed and revised initial manuscript, approved the final manuscript, and submitted the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.