
Abstract
Introduction
Falls are the second leading cause of death from unintentional injuries worldwide (Roth et al., 2018) and are the main cause of morbidity and disability in the older adults (Tareef, 2011). It has been shown that 30% of people over the age of 65 fall each year (Gillespie et al., 2009), and half of the cases are recurrent falls (Tinetti & Kumar, 2010). It is estimated that falls account for 55% of all accidental injury-related deaths among people over 65 in the US (Kramarow et al., 2015).
Patient falls within hospitals are the most common adverse event leading to severe injury, delayed functional recovery, increased lengths of hospital stay, and medical costs (Najafpour et al., 2019), which should receive public health attention. The guideline from the National Institute of Health and Care Excellence recommends that all hospitalized patients over 65 years of age should be considered as the population with fall risk (Health & Excellence, 2013). Identifying risk factors for falls in hospitalized patients can early identify patients with a higher risk of falls and implement a prevention plan. The commonly identified risk factors for falls in hospitalized patients include patient-related and medication variables, such as advanced age (>85 years), longer length of stay, a recent fall, balance condition, neurocardiovascular instability, and adverse drug reactions (Najafpour et al., 2019; Oliver et al., 2004). While various studies have explored risk factors for falls in older adults, there remains a significant gap in the literature regarding the specific challenges faced by hospitalized older adults patients, particularly in regions like China. While some studies have identified the association between stroke history and fall (El Sayed et al., 2023; Yi et al., 2021), none specifically investigate how stroke history contributes to falls risk in hospitalized settings. Additionally, while gait speed is mentioned in various studies (Adeli et al., 2023; Morrison et al., 2021), none focus on its association with falls specifically in hospitalized older adults. Here, the complexity of existing assessment methods, such as the Johns Hopkins Fall Risk Assessment Scale, poses challenges for widespread implementation, exacerbated by the limited availability of specialized geriatric healthcare professionals. Consequently, there is a pressing need to develop and validate simplified assessment tools or indicators that can effectively screen high-risk patients and facilitate timely fall prevention measures in hospital settings. Therefore, the purpose of this study was to investigate the risk factors for falls in hospitalized older adults patients in China.
Methods
Study Subjects
According to the “Law of the People’s Republic of China on the Protection of the Rights and Interests of the Elderly” (Standing Committee of the National People’s Congress, 1996), enacted in 1996 and revised in 2018, elderly individuals are defined as those aged 60 years and older. Older adults patients hospitalized in the Department of Geriatrics of our hospital from July 2018 to July 2020 were recruited using a convenience sampling method. The inclusion criteria were: (1) patient aged ≥60 years old; (2) able to walk independently to complete the walking test; (3) with certain reading and comprehension skills; and (4) voluntarily participated in this study and provided informed consent. The exclusion criteria were: (1) patient had one of the following diseases: cognitive impairment, speech impairment, hearing impairment, severe organ dysfunction, mental illness; and (2) unable to complete the survey. This study was approved by the institutional review board (IRB) of our hospital (Approval No. [2021]495) and written informed consent was waived by the IRB due to the retrospective nature of this study.
Sample Size Calculation
The minimum sample size was estimated according to a method with a sample size of approximately 5 to 10 times the number of items on the scale. There are seven items in the Johns Hopkins Fall Risk Assessment Scale used in this study, thereby the required sample size should be 35 to 70 people. Considering the sample response rate and the missing rate of the questionnaire, the sample size was increased by 20%. Thus, a sample of 42 to 84 cases was required.
Diagnosis of Sarcopenia
Sarcopenia was diagnosed based on the Asian Working Group for Sarcopenia (AWGS) 2019 consensus criteria: reduction in skeletal muscle mass (bioelectrical impedance analysis, BIA): Male < 7.0 kg/m2, female < 5.7 kg/m2) accompanied with decreased muscle strength (grip strength: male < 28.0 kg, female < 18.0 kg) and or decreased physical function (6-meter pace: <1.0 m/s).
Skeletal Muscle Mass Measurement
The BIA test (Chen et al., 2020) was adopted to measure skeletal muscle mass. Subjects fasted for 2 hr before the measurement. The subjects were asked to empty their urine, rest for an hour, then stand still for 5 min. The subjects then took off the shoes and socks, and a small amount of alcohol was applied to the soles and fingers. The subjects stood with both feet on the electrodes on an InBody 770 body composition analyzer (Biospace Co., Ltd, Seoul, Korea) and held the electrodes with both hands, and separated the arms and the torso at about 30°.
Muscle Strength Measurement
Muscle strength was assessed using grip strength. The instrument utilized for measuring grip strength was the Camry Electronic Hand Dynamometer (Model EH101, Sensun Weighing Apparatus Group Ltd, Guangdong, China). Grip strength was measured using a spring-loaded grip dynamometer in a standing position to extend the elbows. If the older adults cannot stand independently, sitting measurement was adopted. Grip strength was measured at least twice with the dominant hand, using the maximum force for isometric contractions and the maximum value was recorded (Chen et al., 2020).
Physical Function
According to AWGS 2019 (Chen et al., 2020), the time for the subjects to walk a distance of 6 m at a normal speed without deceleration was measured, and the mean result of at least two measurements was taken for analysis. An gait speed <1.0 m/s was defined as reduced physical performance.
Fall Risk Assessment
The Johns Hopkins Fall Risk Assessment scale (Poe et al., 2007) was adopted. The scale consists of two parts. The first part classifies the fall risk according to the patient’s situation: low risk: the patient was in a coma or completely paralyzed; high risk: with a history of >1 fall within 6 months before hospitalization, a history of falls during hospitalization, and the patient was defined as high risk of falls according to the hospital regulation. The patient who did not meet any of the items in the first part of the scale would proceed to the second part of the assessment. The second part consists of seven items, including the patient’s age, history of falls, bowel and bladder excretion, high-risk drugs such as analgesics, anticonvulsants, antihypertensive diuretics, hypnotics, laxatives, sedatives, and psychotropic drugs, the number of tube placement, mobility, cognitive ability. Two items of mobility and cognitive ability were multiple-choice questions, and the rest are single-choice questions. The scores for each item were cumulatively added to produce a total score of 0 to 35 points. The total score of <6 was low risk, 6 to 13 was moderate risk, and >13 was high risk.
Statistical Analysis
Continuous data were indicated with mean ± standard deviation (SD) while categorical data were indicated with number and percentage (%). For comparisons of means among three falling risk grade groups, one-way ANOVA or Kruskal–Wallis test was used according to the normality assumption of each continuous variable. Categorical data were tested using the Chi-square test or Fisher’s exact test (if an expected value ≤5 was found).
Univariate and multivariate linear regression models were used to investigate the factors associated with fall risk. The independent variables which were significant in univariate results were included in a multivariate model, then, the variables which were significant in the multivariate model would be recognized as associated factors. The estimated regression coefficient (B) was reported. Pearson’s correlation coefficient was used to check the linear correlation between continuous variables. If the correlation coefficient was over .7 (criterion of high correlation), in the case of multicollinearity, only one variable could be selected to be entered into a multivariate model among highly correlated variables.
A p < .05 would be recognized as reaching the significance of each test, two-tailed. All above analyses were performed using IBM SPSS Version 25 (SPSS Statistics V25, IBM Corporation, Somers, New York).
Results
Patient’s Clinical Characteristics
A total of 112 elder patients were included (mean age = 76.68 ± 8.65 years male/female = 70/42). According to the Johns Hopkins Fall Risk Assessment, all patients were grouped into the low-(n = 12), medium-(n = 58), and high-(n = 42) (fall) risk groups (Table 1). Among all patients, 49 (43.75%) were with sarcopenia and 22 (19.82%) were on osteoporosis medication. The patient’s clinical characteristics, smoking, alcohol consumption, disease, falling history, osteoporosis medication, mobility, Barthel index, MMSE (Mini-Mental State Examination), and JHFRAT (Johns Hopkins Fall Risk Assessment Scale) score, were listed in Table 1.
Demographic Clinical Characteristics Among Different Fall Risk Groups.

Note. BMI = body mass index; CHD = coronary heart disease; DBP = diastolic blood pressure; HR = heart rate; JHFRAT = Johns Hopkins Fall Risk Assessment Scale; MMSE = mini-mental state examination; SBP = systolic blood pressure.
Comparisons Among Falling Risk Grade Groups
As shown in Table 1, the high-risk group had the oldest age, and the lowest weight, BMI, waist-hip ratio, and phase angle among the three groups (all p < .05). The alcohol consumption rate was highest in the medium-risk group. The stroke history rate was highest in the high-risk group. Patients with a higher fall risk had a higher rate of sarcopenia.
Independent Factors Associated with Falling Risk
To investigate the independent variables associated with fall risk, univariate and multivariate linear regression models were performed. Pearson’s correlation analysis showed that there were highly correlation associations among patients’ weight, fat-free weight, Body Mass Index (BMI), and skeletal muscle index (SMI) (Table 2). Therefore, only SMI was included in the multivariate analysis to prevent multicollinearity.
Pearson’s Correlation Coefficient.
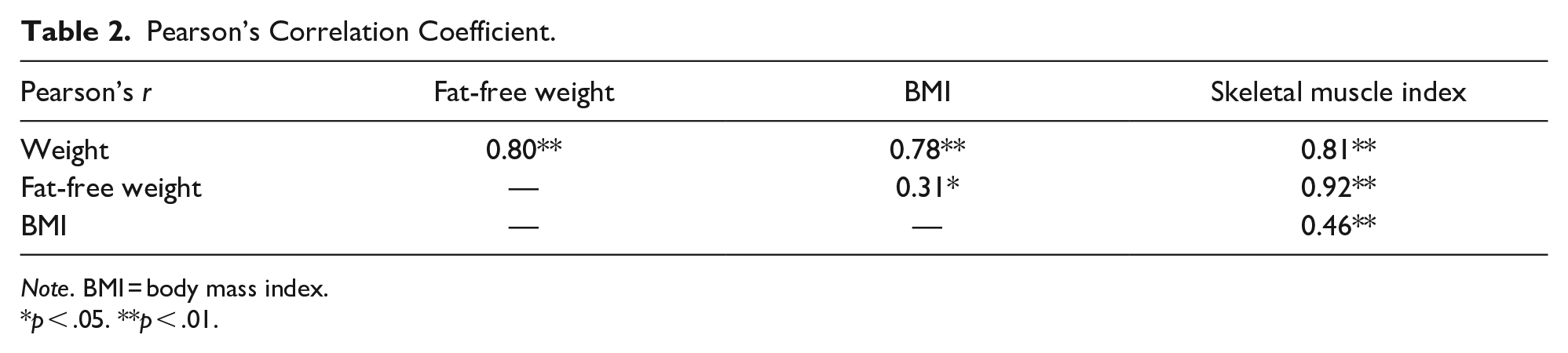
Note. BMI = body mass index.
p < .05. **p < .01.
As indicated in Table 3, the significant factors associated with fall risk in the final multivariate model were stroke history (B = 2.66, 95% CI = [0.43, 4.89]; p = .020) and gait speed (B = −4.78, 95% CI = [−8.74, −0.76]; p = .020). These results suggested that patients with stroke history and poor performance of pace velocity had higher fall risk.
The Linear Regression Results of Independent Variables Associated with Falls Risk.

Note. Weight, BMI, SMI, and FFW were highly correlated, SMI was chosen to use in multivariate model. ADL score and Barthel index were highly correlated, Barthel index was chosen to use in multivariate model. BMI = body mass index; CHD = coronary heart disease; DBP = diastolic blood pressure; HR = heart rate; MMSE = mini-mental state examination; SBP = systolic blood pressure.
Figure 1 shows the scatter plots of two associated factors (stroke history and pace velocity) to the patient’s JHFRAT score and fall risk. It was found that more patients with stroke history had grade 2 and grade 3 risk. The linear trends of pace velocity (of 6 m) were more obvious in both JHFRAT and falling risk grade, the better the speed, the lower the risk of falling. These findings were consistent with the results of multivariate analysis.

The scatter plot of stroke history to JHFRAT (A), falling risk grade (B), and the gait speed to JHFRAT (C), falling risk grade (D). The codes of falling risk grade were low (1), medium (2), and high (3).
Discussion
In this study, we investigated the risk factors for falls in hospitalized older adults patients in China. The results showed that the high-risk group had the oldest age, and the lowest weight, BMI, as well as the highest rate of stroke history and sarcopenia among the three groups. Multivariate linear regression analysis revealed that stroke history (B = 2.66, 95% CI = [0.43, 4.89]; p = .020) and gait speed (B = −4.78, 95% CI = [−8.74, −0.76]; p = .020) were the significant factors associated with fall risk in hospitalized older adults patients.
Accumulating evidence has suggested the association between fall risk and history of stroke (Abbs et al., 2020; Del Brutto et al., 2019, 2020; Grundstrom et al., 2012; Homann et al., 2013; Lukaszyk et al., 2016, 2018; Mackintosh et al., 2005; Paliwal et al., 2017; Yi et al., 2021). It has been shown that people with a history of stroke had an increased fall risk as compared with the age-matched older adults population without stroke (Homann et al., 2013; Lukaszyk et al., 2018; Mackintosh et al., 2005); which is consistent with our findings. Del Brutto et al. (2019) have reported that a history of stroke was associated with the Downton fall risk index (DFRI) which can be used to predict the risk of future falls in rural Community-Dwelling older adults. Abbs et al. (2020) have reported that a history of stroke was associated with an increased risk of falls in older homeless adults. In addition, studies have also revealed that patients with a stroke history had an increased risk of recurrent falls in the older adult population (Graafmans et al., 1996; Paliwal et al., 2017; Yi et al., 2021). Following stroke, the patients generally have physical, cognitive, and psychological impairments, such as decreased muscle strength, poor balance, visual neglect, sensory loss, and fear of falling, which thereby can increase their fall risk (Batchelor et al., 2012; Beatriz Pinto et al., 2014; Mackintosh et al., 2005). Therefore, hospitalized older adults patients with stroke history, particularly need to prevent falls.
It has been shown that gait speed is influenced by various factors such as body weight, height, age, gender, and non-dominant hip abduction strength (Bohannon, 1997). Gait, balance ability, and falls avoidance entail the integration of neuromusculoskeletal, visual, and vestibular systems (Abu Samah et al., 2016). Gait speed plays a vital role in maintaining upper body dynamic stability during movements, thus preventing falls (Alizadehsaravi et al., 2022; Dingwell et al., 2000). Therefore, reduced gait speed might signify impaired balance control, consequently heightening the likelihood of falls, which aligns with our findings in hospitalized older adults. Moreover, age-related reductions in gait speed, lower limb strength, and reaction times might exacerbate the susceptibility of older adults to falls. In line with this observation, Zille de Queiroz et al. (2020) have reported that gait speed was associated with the risk of falls in older women with low back pain. Scott et al. (2015) have found that increasing gait speed was associated with a reduced likelihood of recurrent falls in community-dwelling older women. Interestingly, gait speed itself is also used as a screening tool to assess the risk of falls in community-dwelling older women (Štefan et al., 2020) and adults aged ≥80 years (Magnani et al., 2021). However, the effectiveness of the gait speed test as a tool to identify the fall risk has not been confirmed.
Increasing age is considered to be associated with declines in gait speed, lower limb strength, and slower reaction times, thereby increasing overall fall risk (Morrison et al., 2016). In this study, age was a significant variable in univariate linear regression models, however, it was only marginally significant (p = .056) in multivariate linear regression models. This result may be attributed to the relatively small sample size of this study. In this study, the Asian Working Group for Sarcopenia: 2019 Consensus (AWGS 2019—Chen et al., 2020) was used for the diagnosis of sarcopenia. It was found that the prevalence of sarcopenia in the enrolled hospitalized older adults patients was 43.75%, which was higher than the prevalence of older adults people in the community reported in previous studies. This may be due to different sample sources. The subjects of this study are all inpatients in the Department of Geriatrics of our hospital, who often have more health problems than the older adults in the community. Sarcopenia has been reported to be associated with increased fall risk over 5 years in community-dwelling middle-aged and older adults (Scott et al., 2014). However, our multivariate linear regression analysis showed that sarcopenia is not an independent factor associated with fall risk. This discrepancy may be due to different subjects between studies. The effect of sarcopenia on the risk of falls in hospitalized older adults patients should be further investigated.
This study offers several strengths that distinguish it from previous research and highlight its contribution to understanding fall risk in hospitalized older adults. Firstly, while previous studies have identified stroke history as a fall risk factor, they often focused on community-dwelling older adults (El Sayed et al., 2023) or specific populations like older homeless adults (Abbs et al., 2020). Our study is novel in examining the impact of stroke history on fall risk specifically in hospitalized older adults, a population with different risk profiles and needs compared to those in community settings. Secondly, although gait speed has been mentioned in studies concerning dementia patients (Adeli et al., 2023) and other older populations (Morrison et al., 2021), there has been a lack of focus on its association with falls specifically in hospitalized older adults. Our study addresses this gap by demonstrating that gait speed is a significant factor in fall risk among this group, emphasizing the importance of mobility assessment in hospital settings. Lastly, our study highlights the unique risk factors pertinent to the hospital environment, which can differ significantly from those in community settings. By focusing on hospitalized patients, our findings provide valuable insights into the unique needs of this population and underscore the importance of context-specific fall prevention strategies.
Our findings underscore the need for a simplified and easily implementable assessment method or indicator to screen high-risk patients for falls and promptly initiate fall prevention measures. Given the complexity and impracticality of widely used fall assessment scales, such as the Morse Scale and the Johns Hopkins Fall Risk Assessment Scale, particularly in regions with limited access to specialized geriatric healthcare professionals like China, this is especially crucial. This study’s identification of hospitalized older adults with a history of stroke and low gait speed as having a higher fall risk provides a valuable and straightforward assessment tool for healthcare providers, particularly those working in primary care and community settings, to screen for fall risk in older adults.
There are still some limitations to this study. First, the sample size of this study was relatively small, which may affect the results of the analysis. In addition, this study was a cross-sectional survey, which cannot confirm whether there is a causal relationship between the risk factors and falls. Moreover, the nutritional status, which plays a significant role in this context, was not investigated. In the future, a well-designed large prospective trial should be conducted to validate the findings of this study.
Conclusions
In summary, the results suggested that hospitalized older adults patients with stroke history and low gait speed had a higher fall risk. These findings may be helpful for fall prevention and other comprehensive nursing work for hospitalized older adults patients.
Footnotes
Acknowledgements
We thank all my colleagues in Department of Geriatrics for their excellent data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Science and Technology Program of Guangzhou, China (No. 202002020011).
IRB Approval
This study was approved by IEC for Clinical Research and Animal Trials of the First Affiliated Hospital of Sun Yat-sen University (No. [2021].495). Written informed consent was waived by the IRB due to the retrospective nature of this study.