
Abstract
The need for evidence-based services that help older adults thrive in the community aligns with the economic need to lower costs while achieving better outcomes. Some hospitals with global budgets have started paying for community-based care to decrease hospitalizations. We evaluated health, utilization, and cost outcomes associated with CAPABLE, a time-limited intervention to improve daily function, among 205 participants. The Johns Hopkins Hospital has paid for CAPABLE because it may decrease avoidable hospitalizations while improving outcomes. We used a difference-in-difference approach to compare outcomes for participants and non-participants. Avoidable charges were significantly less for CAPABLE participants compared to non-participants (p = 0.02) between 2016 and 2022. While not achieving statistical significance, participants experienced fewer avoidable hospitals stays and readmissions. Participants had significant improvements in functional outcomes and decreased depression scores. Implementing CAPABLE has potential to yield cost-saving and health improving benefits for hospitals with global budgets and insurers by reducing preventable hospitalizations.
• Expands upon previous CAPABLE research by evaluating implementation within a value-based healthcare system, which has shown significant improvements in functional outcomes and reductions in hospital-based outcomes such as avoidable hospital charges and stays. • Provides evidence of CAPABLE’s contribution to reduced charges for hospitals with global budgets and demonstrates a possible link between community-based interventions that target risk factors for hospitalization and reduction in financial costs for the healthcare system.
• Shows that the integration of community-based interventions such as CAPABLE can improve older adult outcomes and avoidable hospitalizations, while also providing a mechanism for insurers and hospitals to invest in similar programs that not only improve health but also lower cost. • Highlights the need that future gerontological research to explore the impacts of home-based interventions, the pathways linking improved functional outcomes to reduced acute care needs, and the opportunities for scalability of such evidence-based programs for older adults.What This Paper Adds
Applications of Study Findings
Introduction
The US medical system is shifting towards a total cost of care population-based model (Li et al., 2021; Zimlichman et al., 2021). In this model, insurers pay providers for the overall well-being of the population, whereas historically the medical system has been focused on the acute care of individuals (Cohen et al., 2014; Shahzad et al., 2019; Zimlichman et al., 2021). With rising prevalence of chronic illness, an aging population, and high rates of functional limitation that drive acute care utilization, preventing hospitalization and re-admissions has become a key goal for improving outcomes and efficiency. Estimates suggest this could represent $33 billion and $26 billion in potential annual cost savings, respectively (McDermott, 2020; Panagiotou et al., 2019). However, these projections are based on the current healthcare delivery structure and don’t account for potential system redesigns that could further change costs and care pathways.
Functional limitations (i.e., difficulty with daily tasks such as bathing or dress) are a key driver of preventable hospitalizations. Older adults living with functional limitations are three times more expensive to the healthcare system than those without. Improving function may initiate overall improvements that healthcare systems have often overlooked in the past (Bennett et al., 2017; Gruneir et al., 2011; Khavjou et al., 2020; Malani, 2009; Wahl et al., 2009).
In this context, Maryland as a state is ahead of this prevention curve with a Medicare waiver from the Federal government to implement a global budget for hospitals. In this model, unlike a traditional prospective payment system where hospitals receive revenue for each hospitalization of Medicare beneficiaries, hospitals receive a fixed budget for the following year. The goal of this total cost of care model is to shift focus from treating acute care episodes to improving overall health at a population level, emphasizing preventing unnecessary hospitalizations and reducing healthcare charges. This model allows hospitals to understand their revenue from payers in advance and incentivizes providers to support community-based outcomes that may reduce unnecessary hospitalizations, though the long-term impact of such models may also depend on complementary changes in outpatient and community-based care systems (Centers for Medicare & Medicaid Services; Sharfstein et al., 2015). As a result, Johns Hopkins Hospital (JHH) has financed the implementation of The Community Aging in Place, Advancing Better Living for Elders (CAPABLE) program, an evidence-based program for older adults, with the goal of assisting them to maintain their well-being and independence in the community and minimize avoidable hospitalizations.
CAPABLE is a time-limited program that provides home-based occupational therapy, nursing, and handy worker services to older adults who have functional difficulties. CAPABLE is client-directed, meaning that the older adults decide what functional areas to address including safety, functional ability, and well-being of the older adult within their home environment (Washington et al., 2023). Numerous studies have shown that CAPABLE results in improved function (Szanton et al., 2021). A few studies have shown it decreases hospitalizations and nursing home admissions (Ruiz et al., 2017; Szanton et al., 2018), but these studies have been conducted in research settings without sustained real-world implementation.
The aim of this paper is to assess the impact of a CAPABLE program embedded within a healthcare system on preventable hospital utilization, recognizing that such analyses reflect the current landscape and may not capture the full scope of potential savings under other healthcare delivery models.
Methods
Setting and Intervention
The 4-month program supports older adults through up to six visits from an occupational therapist (OT), up to four visits from a registered nurse (RN), and two visits from a handy worker for minor home modifications or repairs as it relates to home safety and client goals. Together, they set goals fully determined by the older adult, brainstorm strategies, and develop action plans that change behaviors to improve health, independence, and safety. OT target areas include home safety, activities of daily living (ADLs; bathing, dressing, grooming, eating, sleeping, intimacy), instrumental activities of daily living (IADLs; such as meal prep, household chores, and grocery shopping), and functional mobility (reaching, bending, functional transfers, balance, walking, step climbing). The RN assesses medication simplification, mood, incontinence, mobility, nutrition, sexual health, healthcare advocacy, and pain management. Participants learn new skills such as fall prevention exercises and how to work with provided supplies and durable medical equipment. CAPABLE emphasizes prevention and problem-solving, while building skills that participants can use in the future. The use of OTs, RNs, and handyworkers and their associated tasks aligns with the CAPABLE model and is described in detail further elsewhere. Handyworkers follow CAPABLE-suggested guidelines and training materials (Szanton et al., 2014).
Goal Achievement
Participants select six goals (three with the OT and three with the RN). The clinicians assist participants in formulating their goals into actionable target areas. The OT and RN then work with participants to identify barriers in achieving their goals. The clinician sessions focus on brainstorming strategies together with the participant to implement between visits to attain desired goals. At the end of the 4 months, each participant assesses their own level of achievement with each goal set.
Sample
To be eligible for CAPABLE, participants (1) were 50 years old or older, (2) had a recent (within 12 months from the date of referral) inpatient or outpatient encounter at Johns Hopkins Health System, (3) reported some difficulty with at least one everyday activity, (4) were cognitively intact, and (5) lived in Baltimore City. Exclusion criteria included 4 or more hospitalizations in the previous 12 months, a diagnosis of Alzheimer’s or dementia, terminal illness, or experiencing active cancer treatment. These exclusions were made based on the clinical design of CAPABLE, which is intended to reach people consistently at home over a 4-month period. Participants were recruited and screened through the case management programs at Johns Hopkins and further confirmed eligibility through a telephone-based screening. Johns Hopkins School of Nursing provided an 8-hour online training for RNs and OTs (CAPABLE, community aging in place, better living for CAPABLE community aging in place better living for elders, 2023), manuals of instruction, and on-going support through bi-monthly office hours with an experienced CAPABLE clinician.
Analytic Sample Construction
In total, there were 3,056 hospital stays made by 469 older adults. Because we allowed the same patient to be a CAPABLE program participant and non-participant at different periods of time (n = 17), this represented 452 unique individuals over the course of 6 years (mean of 8.2, range of 2 to 64). We eliminated 174 older adults from the analysis for the following reasons: 7 observational stays that did not result in an inpatient hospitalization, 154 older adults who were observed only in the pre- or post-program period (only older adults with available data in both the pre- and post-program periods were included to allow for a paired sample), 8 older adults who were coded as non-participants after they finished the program in previous years (n = 151 hospital stays)—these were excluded to avoid skewing the estimated program effects—4 older adults who had presumed skilled nursing facility (SNF) stays based on American Hospital Association (AHA) Survey service code; and 1 older adult who was first a non-participant and later a participant but was excluded due to a presumed SNF stay. Although 295 individuals remained after the exclusionary criteria, an additional eight were excluded due to insufficient post-program outcome data, resulting in a final analytic sample of 287 participants. Figure 1 depicts the sample selection process that resulted in the final analytic sample of 287 participants (114 CAPABLE participants and 173 non-participants), representing 279 unique older adults with 2,294 hospital stays. This resulted in an average of 8.2 hospital stays per older adult over the 24-month observation period. For analyses comparing outcomes, three non-participants were dropped as they were observed only in pre-program period and did not have any information on the outcomes resulting in a comparison group of 170 non-participants. Determination of study analytic sample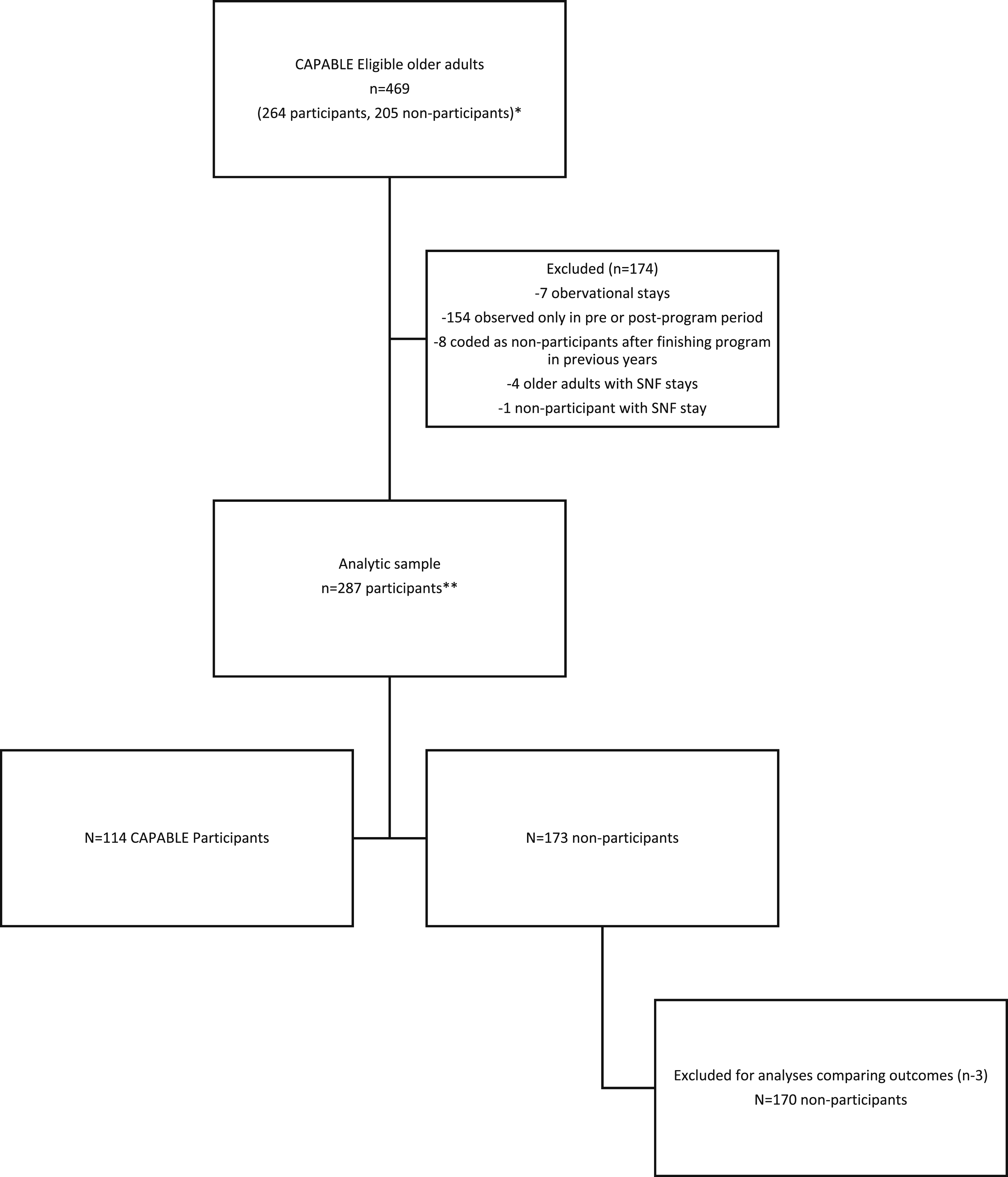
Measures
The following data about JHH older adults who were eligible for CAPABLE were collected.
Demographics
Socio-demographic data (sex, race, age, ethnicity, ADI percentile, Medicare, and Medicaid beneficiary status) were supplied by the EHR-Epic.
Area Deprivation Index (ADI) Percentile: It was measured on a 1–10 scale using 17 socioeconomic indicators in income, education, employment, and housing and identifies areas of deprivation and affluence at the census block level by zip-code, with higher scores indicating greater socioeconomic disadvantage linked to health outcomes like 30-day readmission rates (Kind & Buckingham, 2018). For the purpose of this paper, census data from 2018 was used and ADI census block percentile rankings for 2018 were applied to EPIC-sourced patient demographic data (home address and zip code) to obtain the ADI.
Functional Outcomes
The OT assessed participants at baseline and 4 months later at program completion for CAPABLE participants.
Functional Difficulty: It was measured by using the 8-item Katz Activities of Daily Living (ADL) scale and the 8-item Lawton and Brody Instrumental Activities of Daily Living (IADL) scale, which reflected a client’s rating of functional limitations in both ADLs and IADLS. Clients rated their ability to perform ADLs such as walking, bathing, dressing, eating, toileting, grooming, and transferring in and out of bed, and their ability to engage in independent living skills such as using a telephone, shopping, preparing food, light housekeeping, washing laundry, traveling independently, taking medications independently, and managing financing independently (Katz et al., 1963; Lawton & Brody, 1969). Both were rated on a 3-point scale (0 = no difficulty and don’t need help, 1 = yes difficult, but don’t need help, and 2 = need help regardless of difficulty). The points were totaled and resulted in a range between 0 and 16, with higher scores indicating more functional difficulty.
Activity measure: the Activity Measure for Post-Acute Care (AM-PAC) Home Care Short Form score. It assessed a client’s ability in three areas of function or domains: Basic Mobility Items (7 items), Daily Activities Items (8 items), and Applied Cognitive Items (5 items). The mobility short form is scored on a range from 7 to 28. Higher scores indicate higher function (Jette et al., 2014).
Depressive symptoms: They were measured by using the Patient Health Questionnaire (PHQ-8). Clients rate eight statements with how often in the last 2 weeks they experienced symptoms. A PHQ-8 score of 5–9 indicated minimal depressive symptoms; 10–14 indicated mild depression; a score of 15–19 indicated major depression, moderately severe; and a score >20 indicated major depression, severe (Kroenke et al., 2009). Severity scores ranged from 0 to 24.
Hospital-Based Outcomes
Statewide hospital utilization data was sourced from the State of Maryland’s health information exchange—the Chesapeake Regional Information System for our Patients (CRISP). CRISP has 100% participation real-time clinical data from all 48 hospitals in Maryland (Chesapeake Regional Information System for our Patients, 2024; Gaskin et al., 2018; Horrocks et al., 2016; Kharrazi et al., 2023). Potentially avoidable admissions are hospitalizations from ambulatory-care sensitive conditions that may be preventable through effective primary care and care coordination. Avoidable admissions were identified using Agency for Healthcare Research (AHRQ) Preventable Quality Indicator (PQI) software (Agency for Healthcare Research and Quality, 2022). Maryland measures PQIs on inpatient and observation stays greater than 24 hours. AHRQ specifications are limited to inpatient AHRQ methodology. Hospital-based outcomes listed below are measured in the 24 months surrounding CAPABLE enrollment (12 months prior and 12 months post-baseline).
Potentially Avoidable Utilization (PAU) charges, length of stay, and stays referred to the total potentially avoidable charges in USD, days spent on potentially avoidable hospital stays, and total potentially avoidable stays, respectively. Emergency Department (ED) stays, total charges, hospital length of stay, total hospital stays, and readmissions denote the number of ED stays, total hospital charges in USD for all stays, total days in hospital (admission to discharge plus 1), total stays (inpatient, ED, preventable, re-admission), and number of re-admission stays.
Statistical Approach
First, we descriptively analyzed the demographic characteristics and baseline function scores (ADL, IADL, AM-PAC, and PHQ) among CAPABLE participants and those who were eligible but declined enrollment (non-participants) using two-tail non-paired Student t-tests. To investigate differences in hospital-based outcomes within 12 months after program enrollment, we compared the average and variability of the number of hospital stays, charges, and length of stay in each outcome (as described in the previous section) based on enrollment status. Additionally, we described dynamic changes in hospital-based outcomes by plotting the total count of hospital stays, charges, and hospital days among all the participants and non-participants at 12, 6, 3, and 1 month before and after the program enrollment date, categorized by enrollment status.
Given the non-randomized nature of CAPABLE program participation and the panel structure of the data, we used quasi-experimental methods to estimate program effects on hospital-based outcomes. Our analytic focus was on totals across the 12-month period before and after the intervention. We used a difference-in-difference (two-way fixed effects regression model) design that elicits the program’s average treatment effect by comparing hospital outcomes for CAPABLE program participants 12 months before and 12 months after program enrollment to changes in hospital outcomes among CAPABLE non-participants, both 12 months before and after their refused-to-enroll date. All models were run with linear regression. We applied log transformations for costs outcomes. In order to assess the validity of the difference-in-difference underlying assumption of parallel trends (Roth et al., 2023), we ran several placebo tests (see Supplemental Material 1 for more information). There are no functional outcomes measured for the people who did not participate in CAPABLE. The unit of analysis was the person-period (hospital stay), and standard errors were clustered at the participant level to account for repeated observations.
The statistical analysis was conducted using RStudio programming software R version 4.2.2.
Results
Sample
Among eligible individuals, the sample size was 469 participants (205 CAPABLE participants and 264 non-participants) from 2016 to 2022 with the earliest hospital admission date of August 03, 2016 and the latest admission date of December 26, 2022. This sample equaled the case load of 1 RN and 1 OT for the program. Note for program participants, the 12-month post-program period includes 4 months during which they were receiving CAPABLE visits. Individuals who were eligible but declined CAPABLE did so at the time of outreach or eligibility confirmation, before any intervention visits occurred. The refusal date shows a comparable clinical context to the enrollment date among participants and was used as the index date for non-participants.
Distribution of CAPABLE Participants and Non-Participants’ Demographic Characteristics and Baseline Scores by Enrollment Status
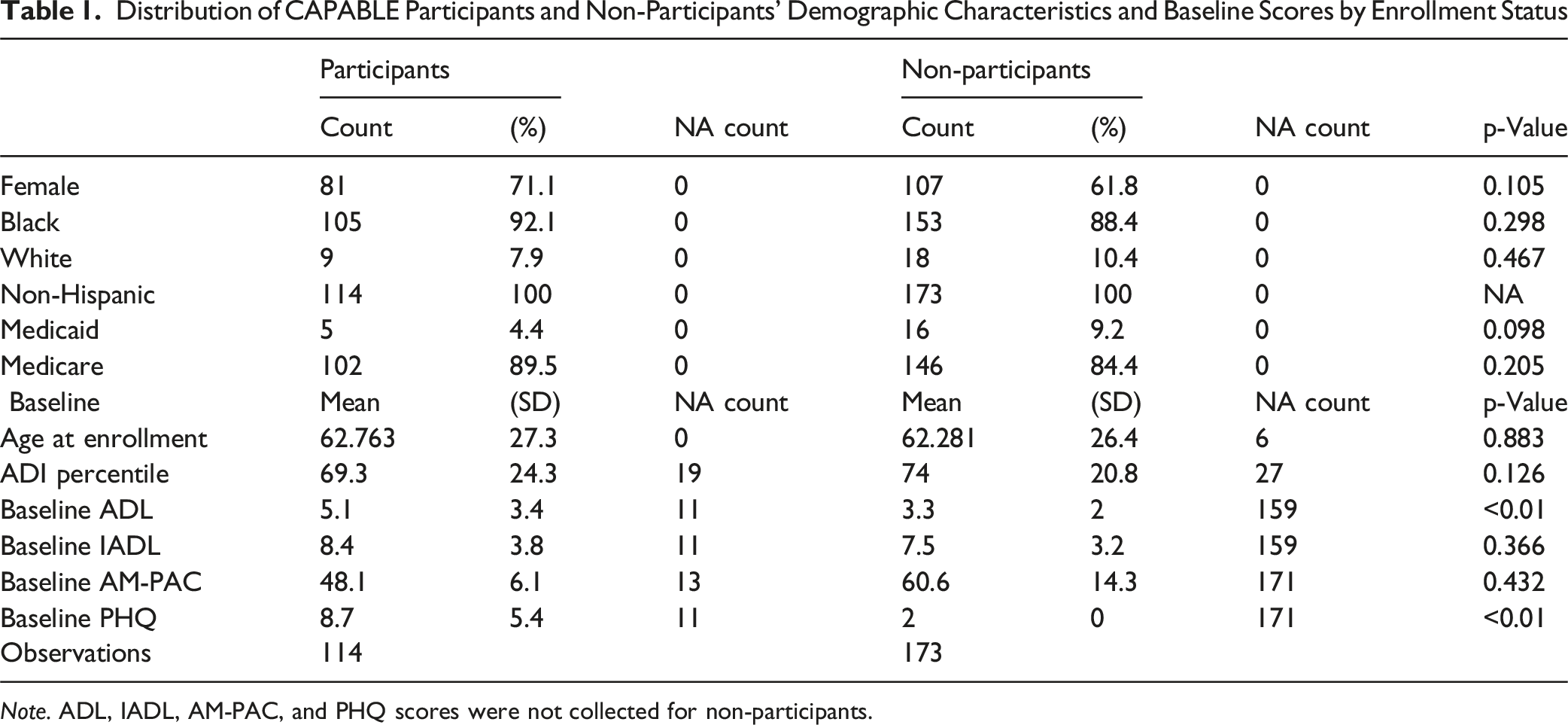
Note. ADL, IADL, AM-PAC, and PHQ scores were not collected for non-participants.
Results
Descriptive Findings
For CAPABLE participants, all measures of function improved after program completion. These descriptive results are summarized in the text below and not shown in a table. ADLs and IADLs significantly improved (p < 0.001) by a mean total score of 2 points out of 16 after program completion, PHQ-8 scores significantly improved (p < 0.001) by a mean total score of 2.9 points out of 24, and AM-PAC scores significantly improved (p < 0.001) by a mean total score of 4 points out of 28.
Figure 2 illustrates sum of all costs, hospital stays, and length of stay in days across time for all patients by participation status in CAPABLE before and after the intervention (note: data is descriptive and unadjusted). As shown in the upper panel of Figure 2, sum of all hospital charges were higher for non-participants compared to participants at 1, 3, 6, and 12 months before and after program enrollment. The cumulative avoidable charges follow a similar pattern, with a notable exception: for participants, cumulative avoidable charges after the program enrollment date remain consistently lower than before the program at every point in time. The cumulative avoidable length of stay, avoidable stays, and re-admissions were all lower before and after program enrollment for CAPABLE participants compared to non-participants. Total number of hospital stays, amount of charges, and days of stay by stay type at 12, 6, 3, and 1 months before and after CAPABLE program (non-)enrollment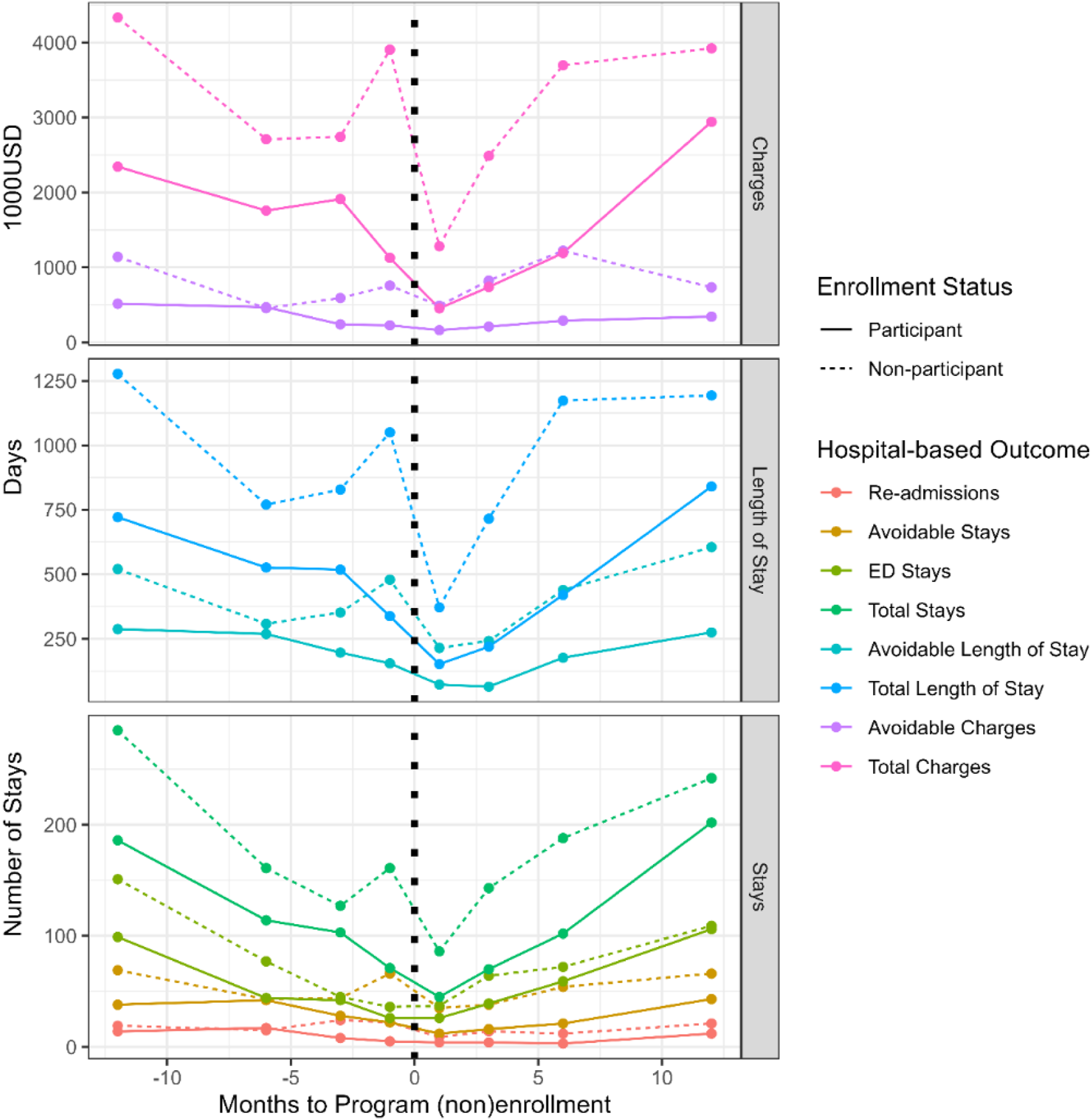
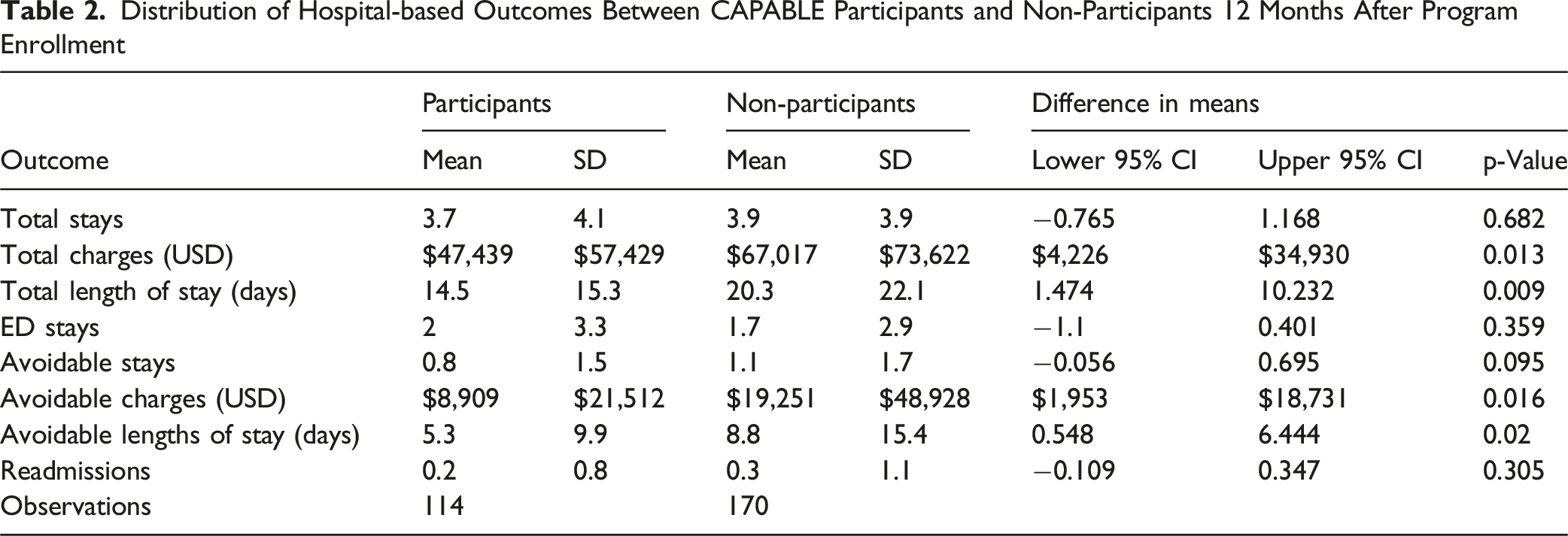
Distribution of Hospital-based Outcomes Between CAPABLE Participants and Non-Participants 12 Months After Program Enrollment
Regression Estimation Results
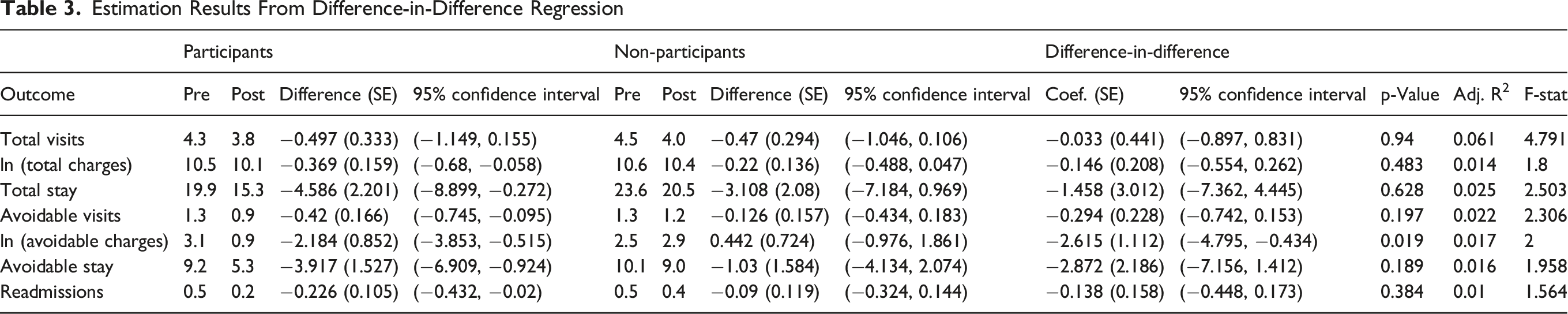
Estimation Results From Difference-in-Difference Regression
Discussion
This study adds to the evidence supporting CAPABLE within a value-based healthcare system, beyond the research setting. CAPABLE participants had significant improvements in all self-reported functional outcomes (ADLs, IADLs, PHQ-8, and AM-PAC scores) and significantly lower hospital charges, shorter overall and avoidable length of stay, and fewer avoidable hospital charges in the year after program completion, compared to non-participants. CAPABLE participation was not associated with significant differences in the average number of hospital stays, ED visits, or readmissions compared to non-participants.
CAPABLE is one of the several home-based care interventions that can reduce avoidable hospitalizations and ED visits among older adults (Brian Cassel et al., 2016; Chang & Chou, 2015; Levine et al., 2012; Mattke et al., 2015). One Medicare-focused home visit program found a reduction in hospital and nursing home admissions, promoting aging in place and preventing high-cost healthcare utilization (Mattke et al., 2015). Meeting individuals at home could help alleviate avoidable healthcare charges and burden, though the wider impact will ultimately depend on the surrounding healthcare infrastructure.
This paper extends the literature supporting CAPABLE’s cost-saving potential, regarding avoidable inpatient charges, avoidable hospital stays, and readmissions, compared to non-participants. Although only avoidable inpatient charges reached statistical significance, the descriptive results suggest a consistent trend toward reduced hospital-related utilization among participants. These results align with an earlier cost analysis on a matched cohort trial of CAPABLE (Ruiz et al., 2017). Program costs average $3,500–$5,000 per client over 4 months. Compared to the average costs to provide CAPABLE for each participant, hospitals with a global prospective budget have the potential to save money by offering CAPABLE to people living in their neighboring zip codes.
CAPABLE participants had shorter total hospital stays compared to non-participants (14.5 vs 20.3 days). Although these are descriptive findings, this represents a nearly 1-week (approximately 30%) reduction in length of hospital stays among CAPABLE participants, which is meaningful given the risk of functional decline and other complications during prolonged hospitalization. These findings suggest that CAPABLE may contribute to reducing healthcare utilization and supporting recovery and independence in older adults. They are consistent with a study conducted in Sweden, which demonstrates the severity and complexity of health needs associated with older adult populations and underscores the high level of clinical care needed among similar groups within the US healthcare system (Lundgren et al., 2024).
As in other studies, CAPABLE participants experienced significant functional improvement (ADLs, IADLs, and AM-PAC) post-program completion and a reduction in PHQ-8 scores (Szanton et al., 2016). While improvements in functional outcomes may support older adults’ overall health and aging in place, they do not directly explain reductions in hospitalizations or healthcare spending (Alecxih, 2010). A cohort study testing CAPABLE among Medicaid beneficiaries in Michigan had similar findings with fewer hospitalizations and improved physical function before and after the intervention (Spoelstra et al., 2019). Improving functional outcomes may provide a mechanism for older adults seeking to age at home and out of the hospital and nursing home. The broader economic impact may depend on how care systems evolve to support these goals.
Interventions that specifically target enhancing functional abilities, such as addressing difficulties with ADLs and IADLs, appear to significantly improve home safety, promote aging in place, and reduce unplanned hospitalizations (Courtney et al., 2012; Green, 2013; Lin et al., 2022; Schiltz et al., 2020). Tailored interventions such as those including exercise and home-based strategies have shown to improve function and reduce avoidable hospital readmissions (Courtney et al., 2012; Lyhne et al., 2022). Programs like CAPABLE, which focus on these aspects, have shown some improvements in participants’ functional status which coincided with observed reductions in hospital charges and utilization. Further research might examine whether there is variation in benefit across sub-populations.
This study used rigorous statistical methods to address an important health policy question with accurate hospitalization outcomes with robust health information exchange data. Policymakers should consider the economic implications of health interventions that target preventative measures and its impact on not only an individual-level through promoting better health outcomes but also the healthcare system as a whole.
There are a few limitations to note. This real-world implementation of CAPABLE did not utilize a randomized control group, so findings could be influenced by unmeasured confounders. To address this, we used a difference-in-difference regression to obtain a causal effect using observational data. Functional outcomes were not measured for individuals who did not participate in CAPABLE so they could not be compared to participants. Participant functional outcomes were self-reported and may reflect recall or social-desirability bias. However, the improvements are similar with other CAPABLE studies measured by staff masked to treatment group.
Although we evaluated hospital-related outcomes, such as hospital stays and readmissions, a full economic analysis including non-hospital costs (e.g., outpatient care, long-term services, and social supports) and the cost implications if the program were scaled to all eligible individuals was beyond the scope of this analysis. This study estimated potential cost avoidance based on reduction in hospital charges, rather than realized net savings.
It is important to note that these results reflect the Maryland global budget model and a predominately Black, low-income, urban population. While this is a strength for equity-focused research, findings may not generalize to other states, systems, or populations without similar financial incentives. Additionally, this study did not account for the influence of broader social determinants or environmental factors, or the COVID pandemic which occurred during this implementation, and may differ between groups and could affect both costs and outcomes.
The practical implications of these findings center on the feasibility of scaling evidence-based, home-based interventions within existing healthcare systems. Because this was not a randomized trial, causality cannot be established. However, the observed patterns suggest that investments in functional improvement programs may align with broader healthcare transformation goals, particularly in systems that bear financial risk for population health outcomes. Policymakers and healthcare leaders should consider how payment structures, workforce availability, and community partnerships can be leveraged to support similar interventions. As more insurers move towards value-based care, there will be more programs developed to prevent hospitalization. Programs that target risk factors for hospitalization and re-admission like CAPABLE can help reduce incurred avoidable healthcare charges while improving the daily lives of older adults.
Supplemental Material
Supplemental material - Saving Healthcare Costs in the Real-World: Implementation of CAPABLE in Population-Based Care
Supplemental material for Saving Healthcare Costs in the Real-World: Implementation of CAPABLE in Population-Based Care by Samantha Curriero, Hanna Charankevich, Katherine A. Ornstein, Diane Lepley, Allyson Evelyn-Gustave, Bruce Leff, Melissa Richardson, Olga Yakusheva, Eric P. Slade, and Sarah Szanton in Journal of Applied Gerontology.
Footnotes
Acknowledgments
The authors would like to thank business intelligence developer, Kevin Johnson, for his data reporting and analysis support.
Ethical Considerations
Ethical approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The work is supported by the funds from the Rita and Alex Hillman Foundation, and CAPABLE was subsidized from Health and Human Services - Community Funding Project (grant # 90CFPC0018-01-01).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sarah Szanton and Laura Gitlin are inventors of the CAPABLE training program, for which they, Johns Hopkins University, and Thomas Jefferson University are entitled to fees. This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.