
Abstract
Keywords
Introduction
Current cancer chemotherapy regimens involve the use of not only cytotoxic agents, but also molecular targeting agents and immune checkpoint inhibitors, which have been improving the mortality and prognosis of patients with cancer (Hirano & Kato, 2019). However, cancer chemotherapy is associated with a wide variety of adverse events, which often reduce patients’ quality of life. Although mucositis, xerostomia, and dysgeusia are the most common oral adverse events, osteonecrosis of the jaw, which occurs among users of bisphosphonates (BPs) and denosumab (Dmab) and is also known as medication-related osteonecrosis (bone exposure) of the jaw (MRONJ) (Ruggiero et al., 2022), has emerged as a new problematic oral adverse event. Research on BP- and Dmab-induced osteonecrosis rapidly increased after 2003 and 2008, respectively, representing approximately 15% to 20% of publications on BPs and Dmab (Figure 1).

Publications on BPs and Dmab.
The incidence of MRONJ is estimated to be 0.001% to 0.01% worldwide (Khan et al., 2015). On the other hand, the incidence of MRONJ in Japan is reported to be 0.06% to 1.47% (Ishimaru et al., 2022), which is higher than the value estimated by the International Task Force. Higher rates of MRONJ have also been reported in other Asian countries, with some differences seen between races (Chiu et al., 2018).
BPs are potent inhibitors of osteoclast-mediated bone resorption (Aapro et al., 2008; Black & Rosen, 2016) and the most common medication in the treatment of osteoporosis and related fractures (Black & Rosen, 2016). In addition, BPs are used to treat Paget’s disease and osteogenesis imperfecta during childhood. BPs are also effective in the management of skeletal-related events (SREs) such as hypercalcemia, spinal cord compression, and pathological fractures caused by bone metastases from solid tumors (e.g., breast cancer, prostate cancer, lung cancer) and multiple myeloma (Palmieri et al., 2013). Dmab, a receptor activator of nuclear factor κB ligand (RANKL), is an antiresorptive agent that exists as a fully humanized antibody against RANKL and inhibits osteoclast functions and associated bone resorption (Ruggiero et al., 2022). Dmab significantly reduces the risk of osteoporosis-related fractures and is also effective in reducing SREs in patients with bone metastases from solid tumors (Sugimoto et al., 2015).
However, the mechanisms of MRONJ generation remain poorly understood. The central hypothesis of this pathophysiology is that antiresorptive medications, including BPs and Dmab, inhibit the activation of osteoclasts, thereby suppressing bone remodeling and causing osteocyte expiration and necrosis without replacement with new bone (Soundia et al., 2016; Wehrhan et al., 2019), eventually leading to jaw osteonecrosis. Inflammatory cytokines and bacterial infection have also been reported to play an important role in the development and progression of MRONJ (Hansen et al., 2006; Mawardi et al., 2011; Ruggiero et al., 2014; Soma et al., 2021).
MRONJ is not a new disease, having already been reported as early as 2003 (Marx, 2003). Although the incidence of MRONJ is low, it continues to be a problematic disease because of the lack of established treatments, its refractory nature, and the increasing number of patients using BPs and Dmab to treat osteoporosis and cancer. The incidences of breast and prostate cancer in Japan have increased in recent years as a result of changes in diet and nutrition (Matsushita et al., 2020; Shin et al., 2016). Within outpatient departments, the number of patients with MRONJ has not decreased; in fact, the number of MRONJ operations has increased. One of the reasons why the prevalence of MRONJ has not yet declined may be that awareness of MRONJ in external clinics (including private dental clinics) is not as high as that in cancer base hospitals. In Japan, most dental care is provided in private clinics, where dentists have many opportunities to gain new knowledge and awareness of MRONJ. However, although they may study on their own, dental hygienists (DHs) in private clinics usually obtain new knowledge and education from dentists. Therefore, even if the dentists have sufficient knowledge of MRONJ, not all such knowledge is passed on to DHs. Although dentists are largely responsible for the decline in health caused by MRONJ, dental care is a team practice. We considered that if DHs also had proper knowledge of MRONJ, they could contribute to a reduction in MRONJ cases through their daily work. In their position paper, Mauceri et al. (2022) described the contributions of DHs to MRONJ. They stated that DHs’ appropriate knowledge of MRONJ and attention to changes in the periodontal tissue of patients through regular practice, that is, clinical periodontal examinations, could greatly aid the prevention of MRONJ. To achieve this goal, questionnaires were devised to clarify the knowledge of MRONJ among DHs. Although questionnaire surveys have been conducted in other countries, that questionnaire specifically asked about the types of knowledge about MRONJ DHs had and did not have (Mah et al., 2015). Given this background, the present study aimed to compare the knowledge about MRONJ between DHs in private dental clinics and cancer base hospitals.
Materials and Methods
Few participants were included in this study because it is a pilot study of a planned larger study that will be conducted in our department. It should be added that the majority of DHs in Japan work in private clinics, and very few in-hospital DHs perform clinical activities in cancer base hospitals. In addition, there are differences in the job descriptions of DHs in different cancer center hospitals. Therefore, in this small pilot study, the number of in-hospital DHs was limited to DHs at our hospital and affiliated facilities who deal with patients with cancer on a daily basis. None of the private clinic DHs from the relevant external private facilities had any experience working in a hospital, including cancer base hospitals. The questionnaires were answered in writing rather than online, and the time period was short to ensure minimal bias.
A questionnaire consisting of four sections designed by a task force (dentists and pharmacists) was used in this study for the purpose of MRONJ case reduction. The first section contained demographic characteristics, and the second section referred to basic knowledge on BPs and Dmab among the study participants. The second section asked about the respondents’ understanding of the terms BPs and Dmab and the relevance of these drugs to cancer treatment. The third section focused on adverse events caused by BPs and Dmab. The third section is common to the parallel questionnaire for pharmacists and relates to adverse events caused by BPs and Dmab. The fourth section presented items related to MRONJ, BPs, and Dmab, and asks about the respondents’ clinical understanding of MRONJ.
The data collected were transferred to Microsoft Excel. All statistical analyses were performed using js-STAR version 9 software (http://www.kisnet.or.jp/nappa/software/star/index.htm; Accessed 25 July 2024). The data were analyzed using the χ2 test or Fisher’s exact test. For all tests, the significance level was set at 5% (p < .05).
Results
A total of 63 female DHs (10 from hospitals and 53 from private clinics) participated in this study and answered the questionnaire. Table 1 shows the respondents’ demographic characteristics and basic information.
Demographic Characteristics and Basic Information of the Study Participants.

Note. SD = standard deviation.
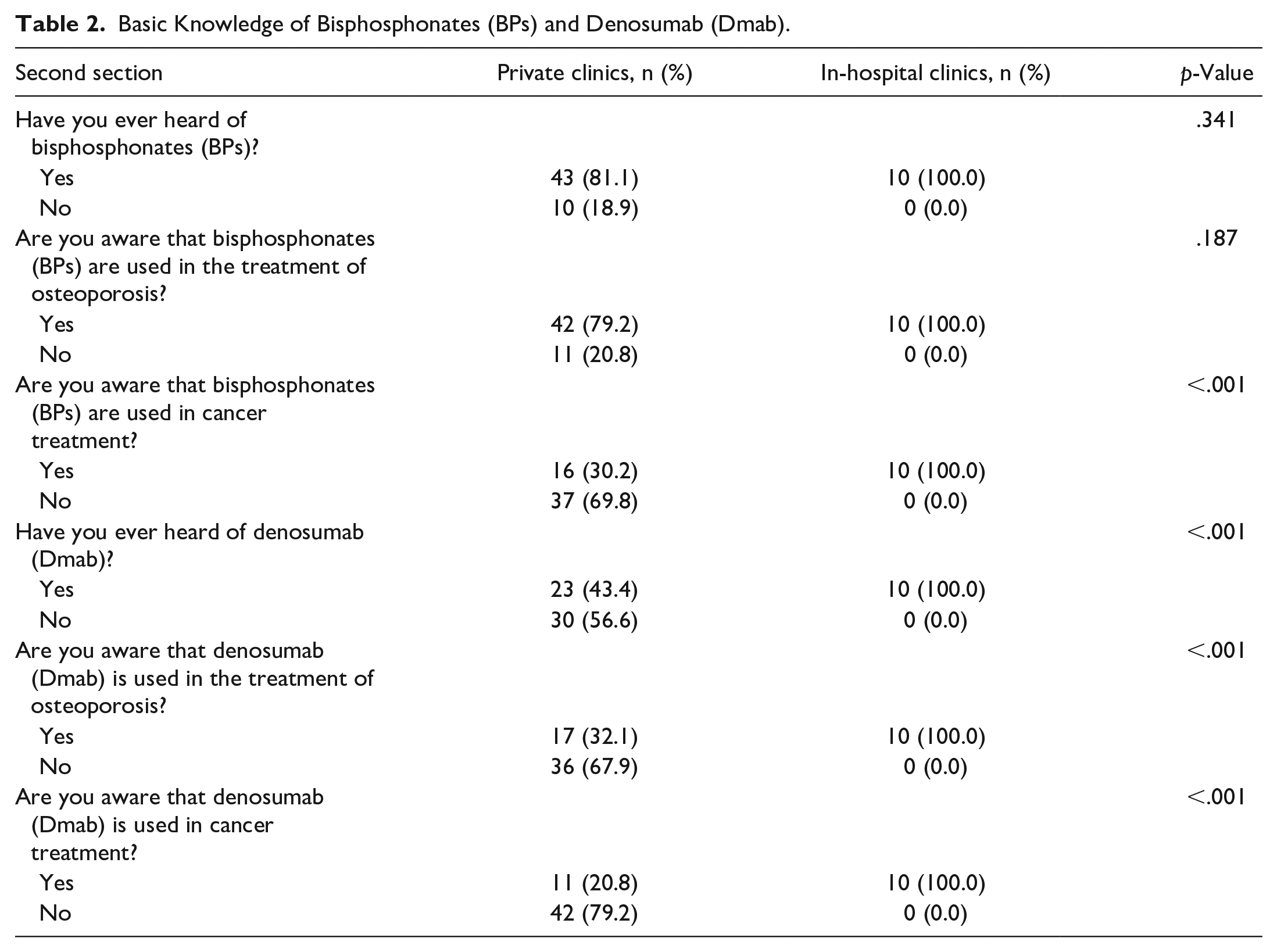
As shown in Table 2, all of the in-hospital DHs were aware that BPs and Dmab were used in the treatment of osteoporosis and cancer. However, very few private clinic DHs knew the name of Dmab or had knowledge about the utilization of BPs and Dmab in cancer treatment (p < .001) (Table 2).
Basic Knowledge of Bisphosphonates (BPs) and Denosumab (Dmab).
In regard to the adverse events caused by BPs and Dmab, 100% of the in-hospital DHs enumerated MRONJ, followed by gastrointestinal symptoms (40%), constipation (30%), hypocalcemia, anemia (20%), skin symptoms (eczema and cellulitis), fatigue, and back pain (10%) (Table 3). It should be noted that the private clinic DHs were aware of all of these adverse events to a lesser extent than the in-hospital DHs.
Adverse Events Associated With Bisphosphonates (BPs) and Denosumab (Dmab).

A significant difference between these two types of DHs was found for Dmab-induced MRONJ (p < .001) and for BP- and Dmab-induced constipation (p = .025).
Table 4 shows the characteristics of MRONJ caused by BPs and Dmab. In relation to dental factors, the private clinic DHs were relatively aware that tooth extraction was associated with BPs and Dmab, but significantly unaware of the other items. Significantly fewer private clinic DHs had seen photographs or observed the actual oral cavity of patients with MRONJ (both p < .001). Regarding the treatments for MRONJ, antibiotics, oral health care, and necrotic bone removal were relatively well known among private clinic DHs, but in general, were significantly less known compared with in-hospital DHs. Knowledge of some cases of MRONJ refractory to antibiotic treatment was significantly lower among private clinic DHs than among in-hospital DHs (p = .012). Knowledge of the importance of regular dental visits and oral health care practices to prevent the development of MRONJ in patients using BPs and Dmab was lower among private clinic DHs than among in-hospital DHs, but this difference was not significant (p = .0502).
Association Between Bisphosphonates (BPs) and Denosumab (Dmab) and Osteonecrosis of the Jaw.

Discussion
The present study was conducted as a pilot study prior to a planned large-scale study in the future. To clarify the level of awareness of MRONJ in external institutions, we conducted a questionnaire survey regarding the level of understanding of MRONJ among DHs in private dental clinics and then compared the results with those of cancer hospital DHs. These DHs were chosen as the target group because DHs in private clinics spend a lot of time talking to patients outside of practice, such as at the reception, during which time, the DHs provide useful information to the patients. Based on the findings of this study, the in-hospital DHs were well informed about recent cases of MRONJ. However, although the DHs in private clinics knew that BPs could cause MRONJ, only a few had any deeper knowledge.
In a previous survey of DHs, Mah et al. (2015) reported that the rate of awareness of BP-related MRONJ in South Korea in 2017 was lower among DHs in private dental clinics (62.7%) than among DHs in university and dentistry hospitals. Although the locations and ages of the DHs in that study differed from those in the present study, the association between MRONJ and BPs is now relatively widely known amongst DHs in private dental clinics in Japan.
With regard to the other basic information about MRONJ, few private clinic DHs knew the name of the other antiresorptive, Dmab, or that antiresorptives are used for not only osteoporosis, but also cancer treatment. This is closely linked to educational issues for DHs; although the relationship between BPs and MRONJ has been incorporated into lectures relatively quickly, the name of a similarly acting drug, Dmab, and information on its use in cancer treatment has not yet been fully incorporated into the syllabus. The numbers of patients with breast and prostate cancers are expected to increase in the future, and higher doses of BPs and Dmab are used in cancer treatment, possibly leading to a higher incidence of MRONJ (Ruggiero et al., 2022; Siegel et al., 2022). Therefore, it is essential for DHs to be aware of Dmab and the fact that BPs and Dmab are used in cancer treatment. In addition, Dmab is an injectable drug, whereas BPs can be taken either orally or via injection. It is important to know that antiresorptive drugs are administered not only orally, but also as injections, which is often omitted from regular medication questionnaires (Emkey, 2008).
Antiresorptive drugs can cause adverse events other than MRONJ, such as gastrointestinal disorders, but many of these were unknown, even among the in-hospital DHs. This is also related to DH education with regard to BPs, where DHs, unlike pharmacists, are not taught about adverse events other than MRONJ.
In terms of the relationship between MRONJ and dental-related factors, many private clinic DHs were aware of the association between MRONJ and tooth extraction. However, few private clinic DHs knew that other factors, such as periodontal disease and incompatible dentures, are also involved in the development of MRONJ (Kyrgidis et al., 2010). This may be due to the over-emphasized fact that only patients with osteoporosis and those on BPs are contraindicated for tooth extraction. Considering that only a few private clinic DHs had seen photographs of or been in charge of patients with MRONJ, it is important to provide them with more opportunities to learn about MRONJ in depth, such as through training sessions.
It was also unclear to what extent the results of this survey of DHs in private clinics had an impact on the current incidence of MRONJ. However, awareness of MRONJ within private clinics still seems to be insufficient. Dental care requires co-operation among DHs, and a team approach including DHs is recommended (Nifosì et al., 2019). Ensuring that DHs are appropriately trained and have adequate knowledge of MRONJ would improve the level of knowledge among private practices (Di Fede et al., 2018; Mah et al., 2015; Mauceri et al., 2022; Rayman et al., 2009). Furthermore, informing their patients about MRONJ on a daily basis would be beneficial for DHs. The increased co-operation of DHs could ultimately lead to a reduction in the number of MRONJ cases.
This study has one major limitation. Only a small number of DHs participated in this study because it was a pilot study. We believe that future studies with a large number of DHs are needed to validate our findings.
In conclusion, the results of this study suggest that private clinic DHs in Japan are generally familiar with the fact that BPs can cause MRONJ, and appeared to use this knowledge in their practice. However, few DHs were aware that Dmab is an antiresorptive drug or that BPs and Dmab are used in cancer treatment. Moreover, few DHs knew that MRONJ is refractory. Therefore, acquiring more knowledge could assist DHs in reducing the incidence of MRONJ.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.