
Abstract
Introduction
In light of the ongoing COVID-19 pandemic, there has been an increased focus on monkeypox disease, a zoonotic viral ailment that belongs to the Orthopoxvirus genus within the Poxviridae family (Wogu et al., 2020). The resurgence of this previously disregarded ailment has raised apprehension within the medical field. The recent outbreak of the monkeypox virus has posed a significant global threat (Velavan & Meyer, 2022; Zumla et al., 2022). Monkeypox outbreaks began in May 2022, with over 57,000 new cases reported worldwide. As of Jan. 1, 2022, 111 Member States in all six zones have reported monkeypox cases to the WHO. In June 2022, monkeypox cases in older people were predicted to be 1.5% of the total, a low incidence rate. However, the number of instances increased, with 715 cases in 60 to 69-year-olds, 78 70 to 79-year-olds, and 14 in 80-year-olds. No fatalities have been reported, although 10% of these incidents have required hospitalization (Bruno & Buccoliero, 2022).
As of the most recent data, Egypt has reported a small number of monkeypox cases among its older adult population, reflecting a broader global trend. While detailed statistics on monkeypox infections, specifically in older adults in Egypt, are limited, it is crucial to highlight the global context to better understand the disease’s impact. Through Sept. 22, demographic data show confirmed Mpox cases for adults ages 61 and older were among the lowest recorded. The CDC reported 277 cases in that age group. The CDC does not cite older age as a risk factor for older adults, but public health officials continue to stress that anyone who has had close, personal contact with someone who has pox is at risk (CDC, 2022).
While monkeypox has a low fatality rate, vulnerable populations, including older adults, face a higher risk of severe illness, and complications. Older adults, particularly those with weakened immune systems or chronic conditions, are at increased risk. The exact number of deaths among older adults worldwide is not extensively documented, but the overall case-fatality rate remains low, under 1% (National Council on Aging, 2022).
The World Health Organization (WHO) recorded 87,529 laboratory-confirmed cases, 1,098 probable cases, and 141 deaths on May 23, 2023. A weekly diagnosis of numerous unconnected cases and intermittent monkeypox detections in wastewater across jurisdictions suggest a continued transmission that has yet to be noticed. However, daily monkeypox cases have decreased significantly since August 2022. As we approach the following spring and summer seasons, when individuals gather for festivals and similar gatherings characterized by a heightened probability of skin-to-skin contact or greater sexual activity, there is a potential for a significant escalation in the risk of breakouts, necessitating immediate action (CDC, 2023; WHO, 2023).
The clinical presentations associated with monkeypox exhibit considerable heterogeneity in individuals with compromised immune function, such as older adults. Systemic symptoms, rash types, and asynchronous skin lesions resembling other dermatological disorders may delay diagnosis (Bruno & Buccoliero, 2022). Since many older adults have comorbidities and chronic illnesses, they may exhibit disease symptoms that depend on their health state (Chavda & Apostolopoulos, 2022). The smallpox vaccine has been shown to reduce monkeypox transmission. Nevertheless, since smallpox vaccination ceased over four decades ago, over 70% of the global population may lack protection. Due to their sensitivity to monkeypox cross-immunity, older adults with comorbidities are at higher risk from the virus outbreak (Figure 1).

Monkeypox outbreak: probable reasons and management strategies.
Natural disasters, epidemics, and preventive measures such as implementing social distancing protocols significantly impact the mental well-being of older adults. These impacts might manifest in the immediate aftermath and over an extended period. The impact of epidemics on the mental well-being of older adults extends beyond social isolation (Torales et al., 2020). Research after the SARS pandemic in Hong Kong from Nov. 1, 2002, to Aug. 7, 2003, found a 31% increase in elderly suicides compared to 2002 10. During the COVID-19 pandemic in China, 37% of 60-year-olds had depression or anxiety (Meng et al., 2020). Furthermore, the study revealed that women were more susceptible to mental health concerns than men. In an Egyptian prevalence study of older persons, 31.0% expressed substantial peritraumatic distress (Fadila et al., 2021). During the COVID-19 pandemic, this newly found virus may worsen mental health difficulties like worry, distress, anger, frustration, despair, and anxiety in specific populations (Barchielli et al., 2022; Temsah et al., 2022).
In the Arab world, Egypt has the highest proportion of older adults. In 2020, there were 1906.4 million people aged 60 years and over, accounting for 13.5% of the population. By 2050, this number will rise to 20.8% (Aly et al., 2021). Therefore, the existing literature must adequately address the evaluation of information and psychological responses among older adults related to monkeypox. It does not explore if there is an increased level of concern as the reported cases continue to climb. Gerontological nursing has a role in contacting older adults effectively and providing them with care and education that reduces their worry and keeps their minds and feelings intact, which can efficiently affect their quality of life. The rising incidence of monkeypox, particularly in non-endemic countries, underscores the need for focused research on vulnerable populations, including older adults. This demographic is often more susceptible to severe outcomes due to age-related immune system decline and comorbidities. Healthcare systems can better allocate resources, develop targeted interventions, and improve vaccination strategies by understanding the specific impact on older adults. Therefore, this study aims to identify Egyptian older adults’ awareness, concerns, and mental health about the monkeypox outbreak after the World Health Organization declaration (WHO).
Research Question
RQ1: Are Egyptian older adults aware of monkeypox?
RQ2: What are the sources of information regarding monkeypox?
RQ3: What is the level of worry, anxiety, and depression among older adults?
RQ4: What is the relationship between sociodemographic characteristics, awareness, worry, and mental health?
Materials & Methods
A cross-sectional descriptive study design was followed. The study’s target population consisted of adults aged 60 and older attending outpatient clinics. The participants were obligated to possess proficient communication abilities to help collect data and give informed consent to participate in the research.
The combination of initial clinical interviews using standardized psychological assessments, such as the Mini-Mental State Examination (MMSE), medical history reviews, self-reported questionnaires, and behavioral observations ensured that participants with mental health disorders. Signs of low motivation included reluctance to participate, lack of responsiveness during interviews, and minimal engagement with study staff. The initial assessment was done with the participant’s primary care providers to ensure accurate and up-to-date information. This approach maintained the integrity and focus of the study, ensuring that the findings would be relevant to the target population without these confounding factors. So, 254 older adults out of 300 clinic visitors were included in the criteria (30 had mental health issues, and 16 lost the motivation to complete the interview).
The selection used consecutive sampling for 4 months. Consecutive sampling involves selecting all eligible participants who meet the inclusion criteria and are available during the study period. This method ensures that every potential participant accessible within the time frame and fits the study’s criteria is included, providing a comprehensive and unbiased sample.
Data Collection
The survey instrument was solely constructed using the English language. Following this, the tools were translated into Arabic and thoroughly modified by professionals in linguistic studies. The study’s content validity was evaluated according to the health-Related Quality of Life (HRQoL) protocol as follows:
(a) A comprehensive review of existing instruments to ensure the relevance and comprehensiveness of the tool.
(b) A panel of distinguished gerontology, psychiatry, and public health experts, with their wealth of knowledge and experience, reviewed the tool for content validity. Their involvement ensures the tool’s credibility and relevance.
(c) The tools were pre-tested on a 20-person pilot sample selected before data collection, and they were not included in the study, but they were carefully selected to mirror the study population.
(d) The tool’s reliability was assessed using Cronbach’s alpha to measure internal consistency. Test-retest reliability was evaluated by administering the tool to the same participants at two different points in time. Both awareness and worry tools were evaluated for their internal consistency. The Cronbach’s alpha coefficients were .79 and .90, respectively.
(e) Construct validity was established by comparing the tool’s results with established HRQoL measures, such as the SF-36 or WHOQOL-BREF, using correlation analyses.
(f) Exploratory and confirmatory factor analyses were conducted to ensure the tool accurately measured the intended HRQoL domains.
After the study was approved by (BLINDED FOR REVIEW), it took place at the outpatient clinics at (BLINDED FOR REVIEW) from 15 September 2022 until 15 January 2023. Three of 16 hospitals were selected using a simple random sample.
Tools
Tool I: The demographic and health-related characteristics interview sheet included questions regarding the older adults’ age, sex, marital status, educational level, residence, income, living arrangement, and chronic illness.
Tool II: Seven questions examined older adults’ awareness of monkeypox. Two questions required a “yes” or “no” answer. Four questions required participants to choose “true,” “false,” or “I do not know” on a Likert scale. Finally, one question was asked about Monkeypox information sources.
Tool III: Older adults’ worry about acquiring monkeypox was assessed using a Likert scale of five questions, each rated on a five-point scale ranging from “Extremely “worried to “not worry.” A rating of 0 was assigned to the response option “Not worry,” while a rating of four was assigned to the “Extreme worry.”
Tool IV: Mental Status Assessment
A. Mental Health Inventory-5 (MHI-5) was conducted in 2019 by Rivera-Riquelme et al. (2019), and its findings were reported. A person’s psychological well-being and distress are assessed using five components. It measures how often the person has enjoyed himself throughout this period. Mental Health Inventory-5 (MHI-5) uses a Likert scale with four response possibilities from 0 (never) to 3 (always). Higher scores indicate psychological well-being on a 0 to 15 scale. Recent research has revealed that the MHI-5 demonstrates a satisfactory level of reliability, with a coefficient of reliability (CRI) of .854 (Caycho-Rodríguez et al., 2022).
B. Patient Health Questionnaire (PHQ-9) was developed by Huang et al. (2006), and it is a self-report scale of nine items. The nine-item Patients Health Questionnaire (PHQ-9) is self-reported18. It measures depression severity and diagnoses major depressive disorder. Participants assessed their symptoms in the last 2 weeks on a 4-point scale (0 = none to 3 = virtually daily). Good internal reliability was found in a previous study α = .85 (Shrira et al., 2020).
C. Generalized Anxiety Disorder-7 (GAD-7) was developed by Spitzer et al. (2006) and is a seven-item self-report scale that uses DSM-IV diagnostic criteria to assess generalized anxiety disorder severity in 2 weeks. Each item is scored on a 4-point Likert scale that measures symptom frequency. This scale spans 0 (no incidence) to 3 (every day). Internal reliability showed good consistency with a Cronbach’s alpha coefficient of .89 (Shrira et al., 2020).
D. Three-Item Loneliness Scale (UCLA) is a measurement tool used to assess an individual’s level of loneliness (Hughes et al., 2004). This unidimensional measure has demonstrated a notable association with other measures of loneliness. The items in the study were evaluated using a 5-point scale, with a rating range from 1 (indicating “not at all”) to 5 (representing “almost always”). The internal reliability of the measure was found to be satisfactory, with a coefficient alpha (α) of .81(Shrira et al., 2020).
Data Analysis
The data were inputted into the computer and analyzed using IBM SPSS software package version 20.0. The qualitative data were represented using numerical values and percentages. The Kolmogorov-Smirnov test has been used to assess the conformity of the distribution to the normality assumption. The quantitative data were characterized by statistical measures such as the range (minimum and maximum), the mean, and the standard deviation. The statistical significance of the acquired results was evaluated using a significance level of 5%. Pearson’s correlation coefficient was used to evaluate the association between the different study variables. The multivariate regression analysis was used to determine the association between demographic characteristics, other study variables, and awareness.
Results
Sociodemographic and Health-Related Characteristics
According to WHO standards, 51.2% of the participants were classified as “young-old” (65–74 years). Participants’ mean age was 65.24 ± 3.07 years. Females made up 58.3% of studied older adults. Regarding marital status, many older adults, precisely 83.1%, were found to be married. In addition, 38.6% of individuals had completed high school. Approximately 48.8% of the older adults included in the study had previous employment as workers before retirement. For more than half of the older adults, monthly income is sufficient. Also, 91.7% of them live with their families. Comorbidity was common among older adults, with Diabetes Mellitus in over half (61.4%). The results reveal that 51.2% of the older persons under study were middle-aged, aged 65–70. Participants’ mean age was 65.24 ± 3.07 years. Females made up 58.3% of studied older adults (Table 1).
Distribution of the Studied Older Adults According to Demographic and Health Related Data (n = 254).
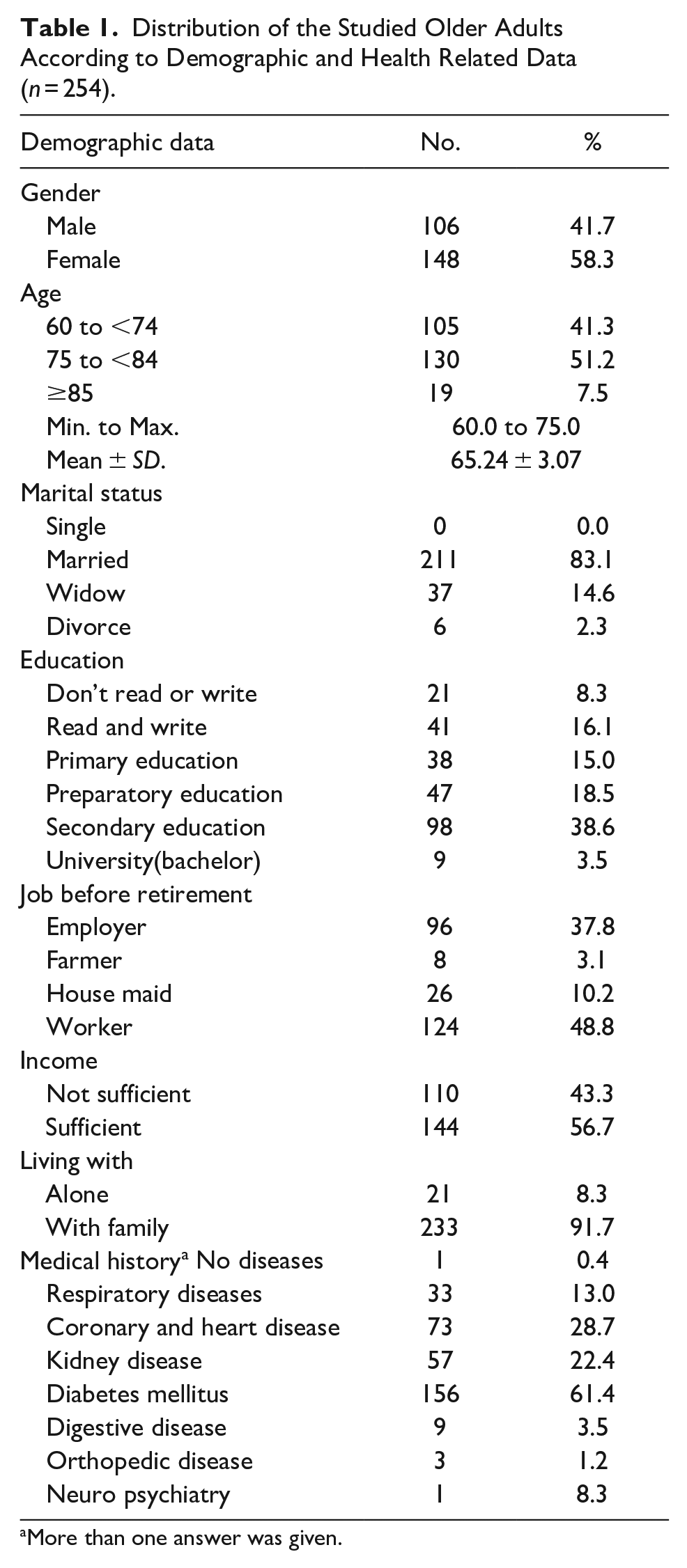
More than one answer was given.
Awareness of Older Adult Participants Regarding Monkeypox
Table 2 demonstrates that 74.0% of older study participants were unaware of Monkeypox, while 26.0% heard it. Television exposure familiarized 72.0% of people with Monkeypox. Over half (78.0%) said Monkeypox is not a new outbreak. The older adults under investigation also lacked knowledge of monkeypox transmission, cases in Egypt during data collection, symptoms, and prevention. When asked if they wanted the monkeypox vaccine, 60.6% of older were willing to take it.
Distribution of the Studied Older Adults According to Awareness Regarding Monkey Pox (n = 254).

Worries of Getting an Infection of Monkeypox
34.3% of the study participants reported a slight worry about getting the infection, and 39.0% and 31.1% were somewhat and little worried about infecting family or friends, respectively. Also, 32.7% reported being somewhat worried about a pandemic, and 35.4% worried about locking down (Table 3). Additionally, 42.5% of the studied older adults felt a high worry about monkeypox infection, 38.6% had a moderate worry, and only 18.9% had a low worry (Figure 2).
Distribution of the Studied Older Adults According to Worry Regarding Getting Monkey Pox Infection (n = 254).


Percentages of the studied participants according to their level of worry regarding getting monkey pox infection.
Mental Health Status of the Participants
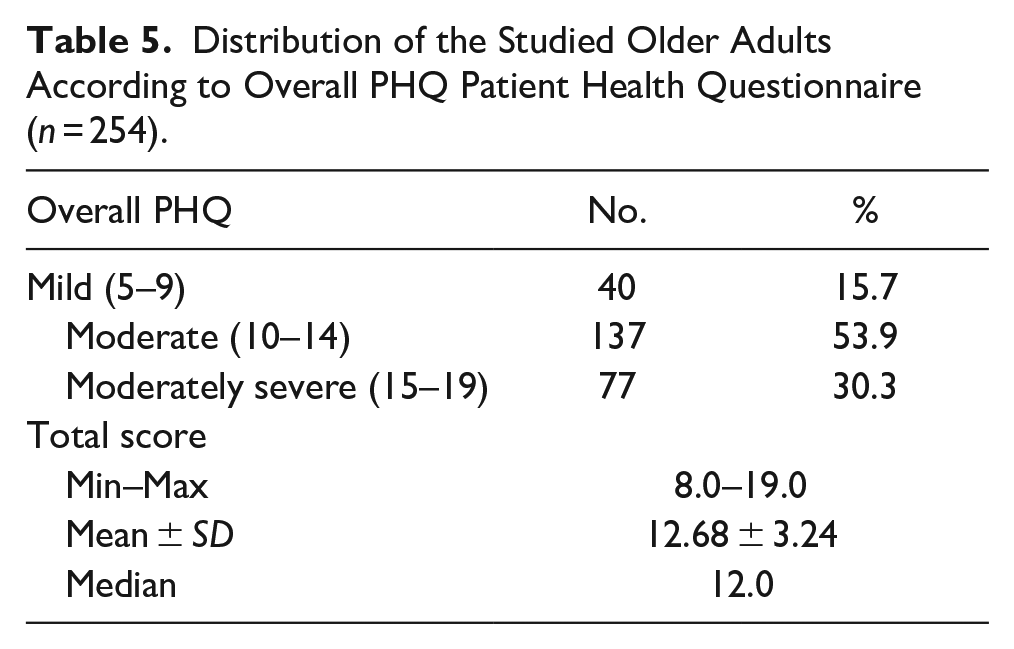
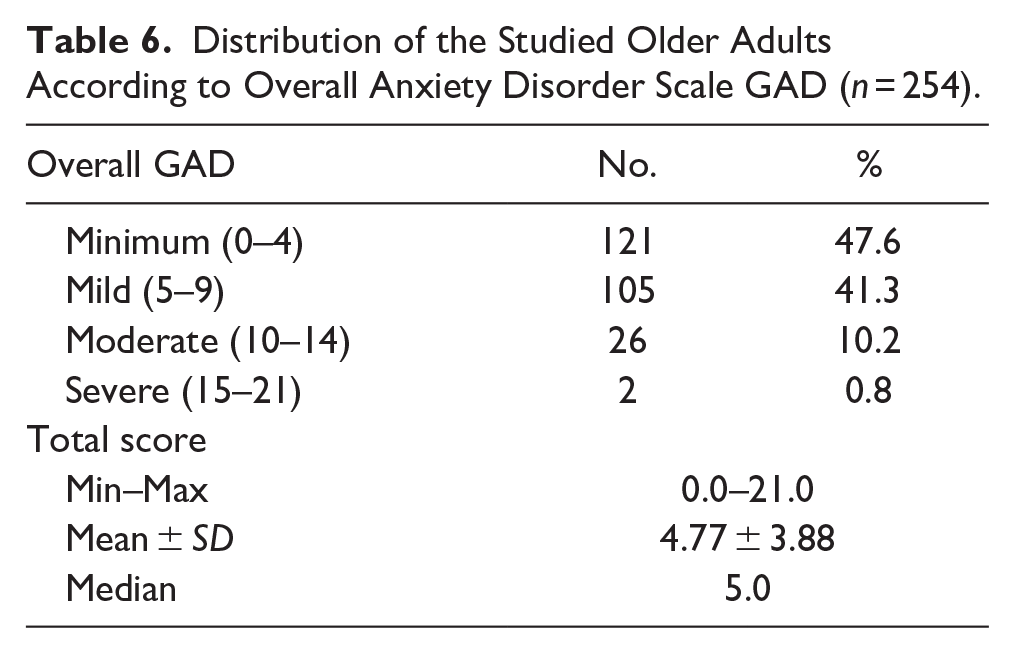
The older study participants’ mental health ratings were descriptively analyzed. The study found a mean score of 6.12 ± 1.17 for mental well-being and 3.60 ± 0.99 for mental discomfort (Table 4). Another important finding was that 53.9% and 30.3% of older people experienced moderate and severe levels of depression, respectively, whereas 15.7% had mild depression, with a mean score of 12.68 ± 3.24 (Table 5). Of the older population studied, 10.2% and 0.8% had moderate to severe levels of anxiety, 47.6% had minimum anxiety, and 41.3% had mild anxiety with a mean score of 4.77 ± 3.88 (Table 6). 37.8% of the older people analyzed in the study reported feeling lonely, as seen in Table 7.
Descriptive Analysis of the Studied Older Adults According to Score of Overall Mental Health (n = 254).

Distribution of the Studied Older Adults According to Overall PHQ Patient Health Questionnaire (n = 254).
Distribution of the Studied Older Adults According to Overall Anxiety Disorder Scale GAD (n = 254).
Distribution of the Studied Older Adults According to Overall UCLA Loneliness SCALE (n = 254).

Correlations Between the Variables
Table 8 reported a negative correlation between awareness about Monkeypox and worries about getting the infection (r = −0.221, p < .001), as the participants with a high awareness level reported a low worry about getting the infection. The analysis found a substantial negative link between MonkeyPox worry and overall mental health (r = −0.292, p < .001). Worry of Monkey Pox infection positively correlated with the GAD anxiety scale (r = 0.179, p = .004). In addition, the overall mental health measure and the GAD anxiety scale are inversely correlated (r = −0.407, p = .001). Depression positively correlates with UCLA loneliness (r = 0.270, p = .001).
Correlation Coefficient Between the Different Parameters.

rs Spearman coefficient.
Statistically significant at p ≤ 0.05.
Multivariate Linear Regression of Monkeypox Awareness
Table 9 shows the results of the multivariate linear regression analysis indicate that gender, level of education, residence, worry about contracting monkeypox infection, and mental distress are predictors of awareness about Monkeypox (p < .001). Worry of contracting monkeypox infection was common among female participants (p = .038), highly educated (p = .001), who had a low level of awareness and high level of mental distress (p = .001 for both).
Multivariate Regression Analysis for the Parameters Affecting Awareness in Studied Participants.
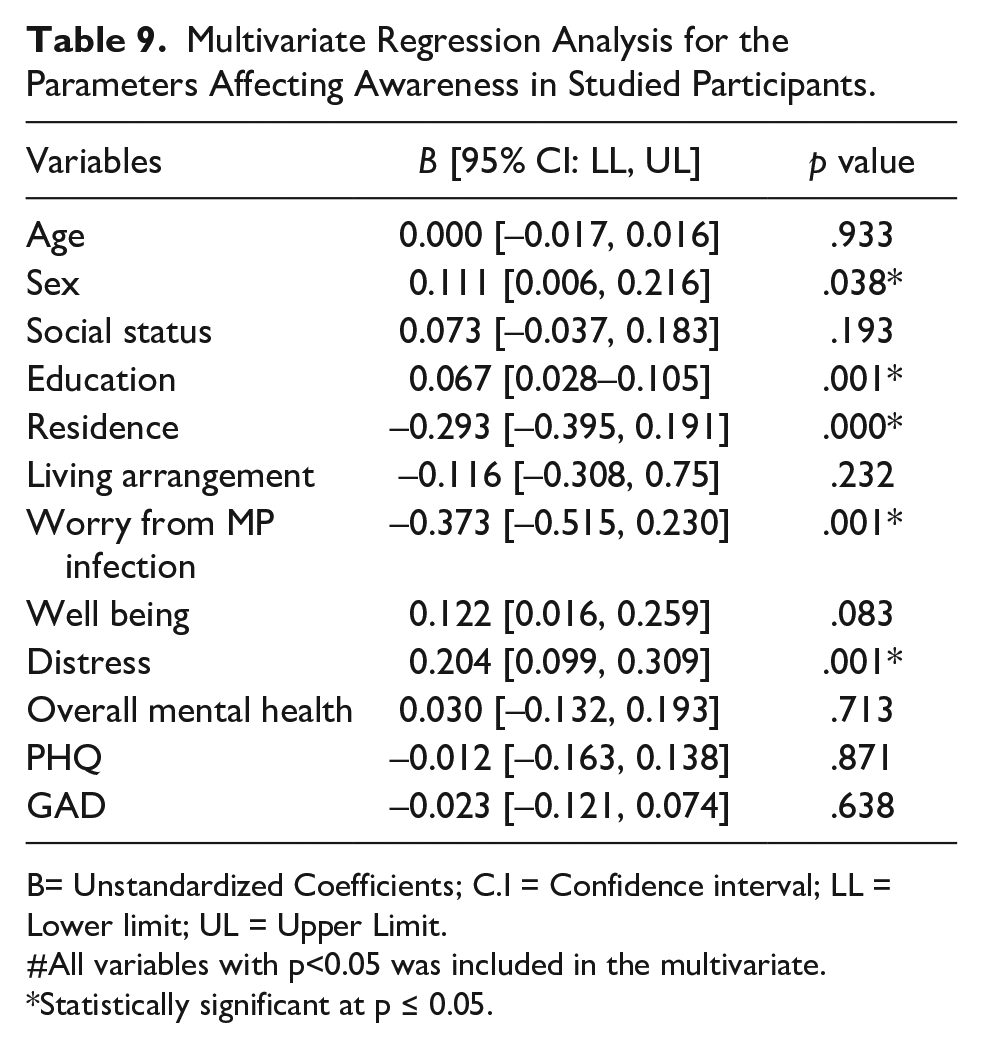
B= Unstandardized Coefficients; C.I = Confidence interval; LL = Lower limit; UL = Upper Limit.
All variables with p<0.05 was included in the multivariate.
Statistically significant at p ≤ 0.05.
Discussion
After 2 years of COVID-19 pandemic containment, zoonotic monkeypox virus transmission has emerged in various non-endemic countries. Unlike smallpox, the illness usually cures independently but must be detected and treated immediately (Shanmugaraj et al., 2022). Previous research in many countries found that the general public’s view of monkeypox needed to be revised, with no studies addressing older persons’ perceptions (Gallè et al., 2022; Jairoun et al., 2022). This underscores the urgent need for more research on older adults’ awareness, worry, and mental health regarding monkeypox.
Epidemics and pandemics repeat, causing many issues for varied people. Insufficient awareness leads to a negligent mindset, which might hinder an individual’s capacity to solve these problems. Outbreaks and pandemics can harm a population’s mental health. The anxiety and stress associated with pandemics and epidemics affect people’s behavior and emotions (Roy et al., 2020). This study assessed older adults’ awareness, worry, and mental health.
This study revealed that 74% of older adults were unaware of monkeypox, while 26% indicated prior knowledge of its existence. Due to television, 72% of people knew about monkeypox. There is an absence of prior research examining the level of awareness of monkeypox among older persons. Existing studies primarily focus on the general community, clinicians, and medical students. This study found a significant difference in awareness levels between older people and those in other studies. The analysis included 1,028 community members, of whom 77.9% had heard of monkeypox, and 65.3% knew about the global outbreak (Ren et al., 2023). A study by Sallam et al. (2022) found that less than 50% of 651 Jordanian health school students knew about the global outbreak. Swed et al. (2023b) stated that Arabic monkey pox awareness was low.
Epidemic status refers to a disease outbreak’s current state and characteristics within a specific population or region. It includes several aspects like prevalence, transmission, severity of the disease, and control measures. Regrettably, the older adults under investigation lacked knowledge of monkeypox regarding transmission, cases in Egypt during data collection, symptoms, and prevention. Furthermore, it is worth noting that 22% of the participants surveyed conveyed the perspective that monkeypox resembles the COVID-19 pandemic, thus suggesting it has the potential to become an epidemic, a scenario that demands immediate attention. A study done by Swed et al. (2023a) showed that a substantial portion of the participants, precisely 43.8%, had a suboptimal level of understanding regarding monkeypox.
In contrast to the findings of Ren et al. (2023), approximately 50% of the participants surveyed demonstrated a high level of knowledge regarding monkeypox and its associated symptoms. Additionally, a notable 9% of respondents expressed concerns that monkeypox could potentially escalate into an epidemic, posing a significant burden on human health, similar to the COVID-19 pandemic. A survey conducted by Riccò et al. (2022) encompassing 163 Italian physicians revealed that just 49.7% of participants demonstrated a general knowledge score of monkeypox that exceeded the median. A survey conducted among a sample of 558 university students revealed that around 80% of the participants exhibited a level of knowledge regarding monkeypox ranging from moderate to good (Jairoun et al., 2022).
While it is not feasible to directly compare knowledge levels across studies due to variations in knowledge items and study groups, it is possible to discover shared deficiencies in knowledge about monkeypox. The limited occurrence of monkeypox cases in Arabic-speaking countries may have influenced our research findings by reducing individuals’ awareness and knowledge. This highlights the necessity of public awareness campaigns to educate the population about the disease. Additionally, older adults primarily relied on television as their primary source of information, whereas younger individuals, who spent more time on social media platforms, exhibited higher knowledge. Consequently, their exposure to monkeypox-related topics on social media platforms may have heightened their curiosity (Lounis et al., 2023). It is imperative to implement awareness campaigns regarding the modes of transmission, prevention strategies, and management approaches to the condition of the public.
Regarding the participants’ desire to receive the vaccine, it was observed that more than half of the participants, precisely 60.4%, agreed when asked about their willingness to obtain the vaccine. This finding aligns with the analysis of Swed et al. (2023b), who revealed that a substantial proportion of survey respondents accepted the monkeypox vaccination. Therefore, a viable strategy for mitigating the outbreak in the Arab world involves adopting vaccination protocols targeting high-risk populations and the application of circular vaccination, which entails vaccinating individuals who have had direct contact with proven cases of infection. This targeted vaccination strategy holds promise for controlling the spread of monkeypox and protecting vulnerable populations, instilling a sense of hope and optimism for the future (Poland et al., 2022). Given the circumstances above, the prior encounter with the COVID-19 pandemic underscores the significance of enacting robust immunization regimens. According to the analysis of the global impact of COVID-19 immunization, many fatalities were prevented following the administration of vaccines (Watson et al., 2022).
A limited number of studies have highlighted concerns arising from monkeypox. The results of the present study indicate that 42.5% of older adults felt high worry concerning monkeypox infection, 38.6% had moderate worry, and only 18.9% had a bit of worry. The results of this survey align with those of a study conducted in Saudi Arabia, in which only 25.3% of the participants expressed significant concern. In comparison, 48.7% reported no or minimal worry regarding the possibility of another monkeypox pandemic (Aljamaan et al., 2022). A study by Ahmed et al. (2022) in the Kurdistan Region of Iraq observed that the level of worry among the general population was determined to be moderate. The observed discrepancies can be attributed to variations in the epidemic status and the impact of preventive and control strategies among different countries. In addition, alternative methodologies existed for assessing the level of worry.
A significant negative link was observed between the level of worry regarding Monkey Pox infection and the individual’s general mental well-being. The concerns regarding the unknown and uncertainty surrounding daily life exacerbate the social isolation and loneliness experienced by the elderly population. These factors have the potential to impact their mental health negatively. In contrast, an inverse relationship was identified between worry regarding Monkey Pox infection and knowledge about Monkey Pox. The combination of inadequate knowledge and susceptibility due to preexisting health issues contributes to increased worries and fears regarding death, as evidenced by the experiences observed during the recent pandemic. Furthermore, a positive correlation was observed between levels of worry and anxiety, which could potentially be attributed to less exposure to mass media and news concerning the impact of monkeypox on elderly individuals. The research recently conducted revealed that over 80% of the study participants indicated a favorable association between social media exposure and anxiety (Gao et al., 2020).
Older adults represent one of the most vulnerable populations to present with behavioral and mental disorders as a consequence of the COVID-19 pandemic (Meng et al., 2020). In addition to the COVID-19 pandemic’s direct impact, several other risk factors contribute to psychological distress in older adults, as loss of close family members or friends can lead to profound grief and a sense of isolation, transitioning into retirement, preexisting health issues can worsen during times of stress, leading to increased anxiety and depressive symptoms, and limited ability to engage in physical activities. Older adults’ psychological distress and psychiatric manifestations ranged from mild symptoms, such as feelings of frustration, distress, fear, and anger, to moderate and severe symptoms of anxiety, depression, sleep disorders, and worsening of preexisting psychiatric disorders (Forlenza & Stella, 2020; Rajkumar, 2020).
The results indicated that the average score for mental distress was 3.60 ± 0.99. The findings align with the research of Hao et al. (2021), who indicated that individuals in mainland China experienced elevated levels of psychological distress during the initial phases of the COVID-19 outbreak compared to periods without an epidemic. Several studies conducted in China, Iran, and India have reported the prevalence of psychological distress linked with COVID-19 among respondents. Specifically, Jahanshahi et al. (2020), Qiu et al. (2020), Varshneyet al. (2020) found that 35%, 61.1%, and 33.2% of participants experienced such distress. Furthermore, it was observed that a significant proportion of the elderly population, precisely 30.3%, exhibited symptoms indicating severe depression.
In addition, it was found that 11% of the participants displayed indications of moderate to severe anxiety. The findings of study 28 agree with the present analysis, as they also reported a comparable proportion of individuals (11.4%) experiencing moderate to severe anxiety levels. Symptoms related to anxiety and depression may be attributed to several factors, including the unknown trajectory of the epidemic, apprehension of personal infection, and anxieties surrounding the health of oneself and other family members (Lai et al., 2020). Prior research has also indicated the occurrence of public health issues during epidemics of Ebola (Shultz et al., 2015) and SARS (Maunder, 2009).
Higher levels of awareness about monkeypox and its risks can lead to increased worry about catching monkeypox, which can significantly impact mental health, causing stress, anxiety, and heightened vigilance. Older adults might limit their social interactions as a coping mechanism to avoid infection, leading to increased loneliness. The pandemic has already heightened feelings of isolation; the added fear of another infectious disease like monkeypox can deepen these feelings. About 37.8% of the older people analyzed in the study reported feeling lonely. A study by Shrira et al. (2020) revealed that the subjective age, or the perception of being younger than one’s actual age, was associated with a reduced experience of loneliness among the older population during the COVID-19 epidemic. Consequently, a higher prevalence of psychological problems was seen among individuals in the older age group. By understanding the interconnected nature of awareness, worry, and loneliness, targeted interventions can be developed to support older adults’ mental health. Enhancing awareness with accurate information, providing psychological support, and fostering social connections are crucial strategies to mitigate the adverse effects of health-related fears and social isolation.
There was no statistically significant link observed between feelings of loneliness and the presence of anxiety, depression, and mental health problems. This finding aligns with the research that observed similar trends among older persons in Spain during the COVID-19 pandemic (García-Fernández et al., 2020). The maintenance of social contacts is significant for older persons. Although older adults tend to use online technology less frequently, there is potential for these technologies to facilitate the establishment of social support networks and foster a sense of belonging. Tailored interventions and support to increase digital literacy and access among older adults could help bridge this gap.
The older adult population exhibits significant heterogeneity across different categories. This heterogeneity can be observed in age periods, as older adults differ physically and cognitively. Additionally, living conditions further contribute to this heterogeneity, with some older adults living alone or in extended families, being retired or actively employed, appearing unemployed but actively engaged in household tasks and grandchild care, living independently or relying on assistance for daily activities, and having either a permanent caregiver at home or residing in nursing homes (Jahanshahi et al., 2020; Qiu et al., 2020; Varshney et al., 2020).
The results of the linear regression analysis revealed a significant relationship between awareness of monkeypox and levels of worry and mental distress. Individuals who possess knowledge of the indicators and manifestations, diagnostic procedures, preventive measures, and approximate mortality rates associated with the pandemic are more inclined to exhibit reduced levels of anxiety and depression. Therefore, it can be asserted that possessing accurate information serves as a preventive factor against the development of anxiety and distress in older adults.
The utilization of Internet counseling and online mental health services has experienced significant proliferation in the 21st century and has also garnered extensive usage during epidemic outbreaks. Given the limited familiarity of older adult adults with online services, it is advisable to offer mental health support lines explicitly catering to the senior population. These support lines serve as a means for voluntary mental health workers to connect with older adults.
Conclusion
The present study identified gaps in the awareness of monkeypox among older adults. Considering null sure cases of monkeypox in Egypt and no significant public attention yet, it seems evident that older Egyptian adults still need to be more concerned about the general knowledge and the possible disastrous consequences of monkeypox. 74.0% of older study participants were unaware of monkeypox. Gender, level of education, residence, worry about contracting monkeypox infection, and mental distress are predictors of awareness about monkeypox (p < .001). Worry of contracting monkeypox infection was common among female participants (p = .038), highly educated (p = .001), who had a low level of awareness and high level of mental distress (p = .001) for both.
This study proposes the subsequent recommendations for further interventions: (1) Increased emphasis should be placed on addressing the needs of vulnerable populations, with particular attention given to the elderly demographic. (2) Enhancements and fortification of medical resources and the public health service system are imperative. (3) Establishing a nationwide framework for strategic planning and coordinating psychological first aid during significant disasters, potentially utilizing telemedicine, is recommended. (4) To mitigate psychological distress and prevent the exacerbation of mental health issues among this population, the development of a comprehensive crisis prevention and intervention system is essential. This system should encompass epidemiological monitoring, screening, referral, and targeted interventions.
The Implication of This Paper
The results emphasize the significance of focused public health communication campaigns to enhance awareness and comprehension of monkeypox among elderly individuals in Egypt through customized educational resources and initiatives to reach the community.
Healthcare practitioners can have a crucial impact on treating the mental health issues experienced by older persons by offering compassionate assistance, facilitating access to mental health resources and services, and incorporating psychological screening and support into regular healthcare procedures. In this way, healthcare professionals can help lessen the negative impacts on older individuals’ mental well-being and general resilience.
It is crucial to emphasize the need for additional research to investigate the enduring consequences of new infectious diseases on older persons’ mental health, social well-being, and resilience. Furthermore, conducting research that targets explicitly efficient interventions and strategies to minimize the consequences of disease outbreaks on older individuals can provide valuable insights for implementing evidence-based practices and policies to safeguard this susceptible population. This research is not just beneficial, but it is also necessary to ensure the well-being of older adults in the face of infectious diseases.
Limitations of the Study
The study’s cross-sectional design limits the establishment of causality between the variables. Plus, the study was conducted within a specific cultural context, and the findings may not apply to older adults from different cultural backgrounds, so the results can’t be generalized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.