
Abstract
Depression and personality traits are independent predictors of dementia or cognitive impairment. Despite the well-established relationship between these two psychosocial factors and dementia, no research has been documented on how personality traits can influence dementia in older adults exhibiting depressive symptoms. This study explores the influence of personality traits on the association between change in depression and dementia in old age. A population-based longitudinal cohort study involving two waves of data collected 5 years apart, containing 2210 American older adults, from the National Social Life, Health, and Aging Project to explore if personality traits influence how change in depression predicts the development of dementia. We assessed these relationships while adjusting for sociodemographic characteristics. Change in depression increased the likelihood of dementia at T2 by 4.2% (AOR = 1.04, p = 0.019) in the co-variate adjusted model. Personality traits, overall, did not influence how depression predicts the development of dementia. However, agreeableness individually nullified the effect of depression on the development of dementia, whereas extraversion was the only personality trait that significantly predicted dementia. Prosocial behaviors should be promoted in old age as these appear to be protective. In addition, early life education and a strong social support can keep the depression–dementia spectrum at bay in old age.
Introduction
Dementia is a common disorder among older adults and is associated with important risk factors such as older age, educational attainment, income, cardiovascular disorders, depression, and other chronic medical illnesses (Bellou et al., 2017; Campbell et al., 2013; Lopez & Kuller, 2019). Over the years, numerous studies have linked long-term depression to the subsequent development of dementia in old age (Byers & Yaffe, 2011; Valkanova et al., 2017; Yu et al., 2020). One of these studies noted that patients with early life depression or depressive symptoms exhibit more than a two-fold increase in the risk of dementia (Saczynski et al., 2010). Interestingly, one longitudinal study revealed that the trajectory of depression could be the most significant risk factor for the development of dementia (Kaup et al., 2016). In this study, older adults with a high and increasing depressive symptom trajectory were reported to have a significantly heightened risk of dementia compared to those with consistent minimal depressive trajectory. However, in studies that try to demonstrate an association between late-life depression and dementia, the results appeared mixed. These associations have been best described as weak or unclear (Byers & Yaffe, 2011; Valiengo et al., 2016).
Aside from depression, the personality trait of an individual is another psychological risk factor that had been remotely associated with the development of dementia, albeit remotely (Terracciano et al., 2017). Some studies describe personality traits as having a direct effect on a person’s behavior, lifestyle, and health (Ali, 2019; Hampson, 2012). There are five major categories of personality traits, also known as the Big-Five personality traits, described by McCrae and John (1992). These are Neuroticism, Extraversion, Openness, Agreeableness, and Conscientiousness. Of these categories, both high Neuroticism and low Conscientiousness have been associated with increased risk of dementia incidence (Kaup et al., 2019; Low et al., 2013). Terracciano et al. (2017) also reported lower Conscientiousness, Agreeableness, and higher Neuroticism as independent risk factors for dementia. Furthermore, Ayers et al. (2020) highlighted that older adults with higher Openness may have a reduced risk of developing cognitive impairment.
Even though several studies have associated late-life depression and personality traits as independent risk factors for dementia, to our knowledge, no single study has evaluated how personality traits influence the way depression predicts the development of dementia in old age. Taking all these into consideration, we sought to explore if personality traits influence the association between late-life depression and the development of dementia over a period of 5 years. The purpose of this study is in two-folds; first, we sought to investigate the association between change in depression following 5 years and the risk of dementia. Second, to explore how the Big-Five personality traits influence this relationship. We utilized two waves of publicly available data, containing 2210 American older adults, from the National Social Life, Health and Aging Project (NSHAP) to explore these relationships. Although two waves of data may not establish causality, we hope to explore if there is a predilection of a particular personality trait to the development of dementia in older adults exhibiting depressive symptoms.
Methods
Study Design and Data Source
This longitudinal study utilized data from the NSHAP population-based study. The publicly available dataset was accessed from the Interuniversity Consortium for Political and Social Research (ICPSR) online website. The NSHAP study sought to explore the various health and social factors that influence the health and wellbeing of older adults across all ethnicities and gender in the United States. This study consists of three waves of data, each collected 5 years apart, with the first and third wave collected in 2005 and 2015, respectively. Face-to-face interviews using structured questionnaires were used in the survey. The wave 1 survey had a total of 3005 participants which increased to 3400 during the Wave 2 period. A total of 4777 older adults were interviewed during the Wave 3 period. Wave 1 data was excluded from this study because the variables representing personality traits were not introduced until the Wave 2 period. Thus, we used only data from Waves 2 and 3. Additionally, only respondents who participated in both waves were included in the analysis. A cohort of 2210 older adults present in both Waves 2 (Time 1-T1) and 3 (Time 2-T2) made up our sample size for this study.
Sampling Method
The NSHAP survey selected community-residing adults based on the Health and Retirement Study’s (HRS) national household screening method. A national area probability sampling method was used to determine the areas to be surveyed. A more detailed sampling method was described elsewhere (Heeringa & Conner, 1995; Waite et al., 2019).
Study Measures
Outcome Variable: We used the Montreal Cognitive Assessment (MoCA), a screening tool for cognitive impairment and early dementia, at time 2 as the outcome variable. Both Waves of NSHAP contained an 18-item MoCA screening survey questions that were extensively described by Kotwal et al. (2016). The total score for the screening scale was 30 points which was divided into three categories based on previous studies: <18 points (dementia), 18–22 points (mild cognitive impairment), and >22 points (normal). We further dichotomized this category into “Normal” coded as “0” (>22 points) and “Dementia” coded as “1” (<22 points) by merging those with mild cognitive impairment and dementia into one. We controlled for baseline Dementia (T1) because it is an important confounder as it might predict both dementia at T2 and other independent variables. Therefore, there could be reverse causality.
Independent Variables:
The two independent variables were depression and the Big-Five personality traits. Depression was measured using the 11-item Center for Epidemiological Studies Depression (CES-D) scale. Respondents were asked a set of 11 questions that were scored as 0, 1, and 2 for rarely or none of the time, some of the time, and much of the time, respectively. The scores were summed up and the participants who had a score between 0 and 22 at both time 1 and time 2 were given a CES-D score (continuous variable). Higher scores indicated a higher depression symptomology. Internal consistencies of all scales were assessed using coefficient omega (Hayes & Coutts, 2020; Peters, 2014). The coefficient omegas were 0.78 and 0.79 for CES-D at T1 and T2, respectively. We attempted to assess “Change in Depression” as a predictor of the risk for dementia rather than depression at a point in time based on Kaup et al. (2016) findings. Therefore, the change was calculated using: (CES-D score at T2) − (CES-D score at T1).
The NSHAP survey also contained 21 items assessing personality traits. Responses to these items were recorded on a Likert scale of “0” to “3” representing “Not at all” to “A lot.” An exploratory factor analysis (EFA) was conducted on these 21 items to determine the Big-Five factor structure as conceptualized by Iveniuk et al. (2014) using varimax rotation. We had a five-factor loading for both waves of data, also reported by Iveniuk et al. (2014), except for the item “Active” that cross-loaded between Extraversion and Conscientiousness at both times. It was found that the item “Warm” also cross-loaded between Extraversion and Agreeableness at T2. The total variance explained by the five factors was 58.5 and 57.7% for times 1 and 2, respectively, and communalities greater than 0.41 for each item at both times. Our five-factor loadings represented the Big-Five traits. We maintained “Active” under Extraversion and “Warm” under Agreeableness in accordance with previous literature (Iveniuk et al., 2014; Sutin et al., 2019). Following EFA and identification of factor components, we used utilized items under each factor loading as scales for both waves. Internal consistencies for the Openness, Conscientiousness, Extraversion, Agreeableness, and Neuroticism scales were 0.75, 0.69, 0.75, 0.77, and 0.68, respectively, at T1. At T2 coefficient omega were at 0.70, 0.70, 0.72, 0.75, and 0.65 in the same order, representing good reliabilities.
Descriptive Statistics.

RTAF = Relative to American families. T = T-test, C = Chi-square for bivariate analysis.
Data Analysis
Model 1: Relationship between depression and dementia at T2.
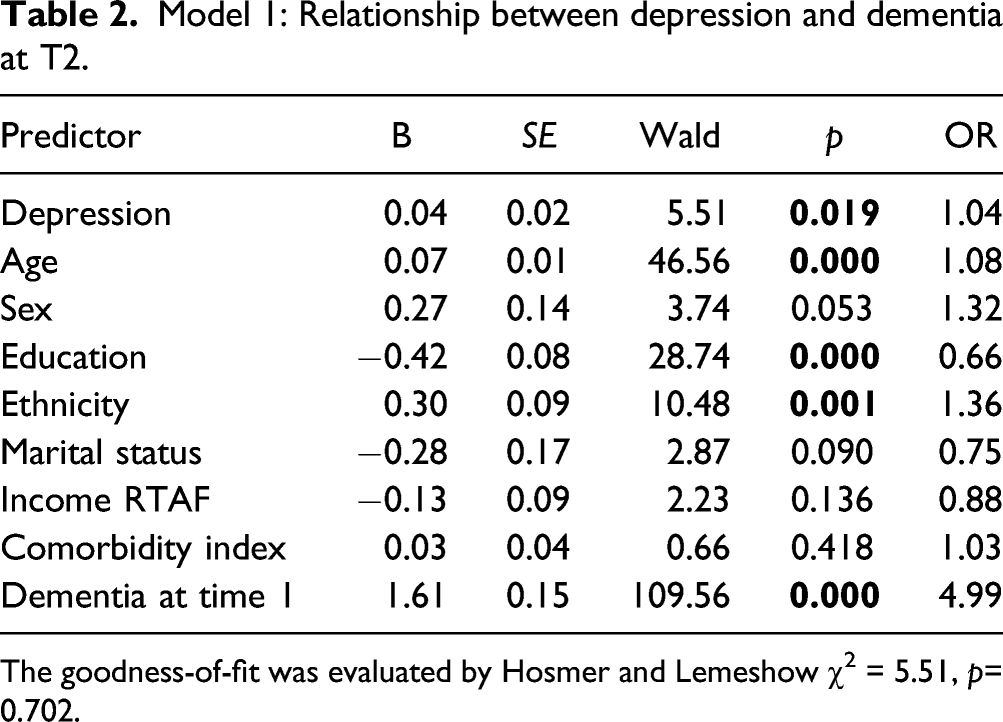
The goodness-of-fit was evaluated by Hosmer and Lemeshow χ2 = 5.51, p= 0.702.
A descriptive statistic of the variables of interests was computed to assess for the distribution of missing data. Majority of the socioeconomic variables had complete data, except for income which was missing some cases. The computed outcome variable and predictor (change in CES-D score) had no missing cases, whereas the 21 variables assessing personality traits had missing cases. Percentage of missing data ranged from 1 to 31%. Patterns of missing data were non-monotone, that is, some individuals did not respond to some of the personality traits-related questions. Therefore, it was assumed that data was missing completely at random (MCAR). Five missing data imputations were created through multiple imputations using a polytomous logistic regression method. Imputation was also conducted with IBM SPSS software version 27.0.
Results
Characteristics of the Participants
The mean age of the participants in this nationally representative sample was 71.6 ± 6.6 years, consisting mainly of non-Hispanic whites (72%). The average age of people exhibiting dementia symptoms was significantly higher at both times (Table 1). There was no gender difference in the rates of dementia. However, at both times dementia was statistically significantly higher among non-married, low income earning, non-White individuals and who have attained a lower level of education (Table 1). We found no statistically significant difference in CCI rates among people with dementia, but depression was significantly higher in individuals with dementia at both times (p < 0.001). Among the five personality traits, people with dementia had a lower Conscientiousness mean score at both times and a lower Openness score at T2.
Model 1: Depression as a Predictor of Dementia
Table 2 shows the logistic regression analysis between change in depression and dementia at T2 while controlling for sociodemographic characteristics, CCI, and baseline dementia. Controlling for baseline dementia is equivalent to assessing the changes in dementia from T1 to T2. Change in depression increased the likelihood of dementia at T2 by 4.2% (AOR = 1.042, p = 0.019). Although used as control variables, age (AOR = 1.077, p = 0.000) and ethnicity (AOR = 1.355, p = 0.001) positively contributed to dementia at T2, whereas educational attainment decreased the odds of dementia (AOR = 0.658, p = 0.000).
Model 2: The Influence of Personality Traits
Model 2: Influence of Personality Traits on the Relationship Between Depression and Dementia.

The goodness-of-fit was evaluated by Hosmer and Lemeshow χ2.
aStatistically significant relationship with dementia itself.
Being extraverted improved the model significantly, that is, Hosmer and Lemeshow χ2 improved from 5.51 to 17.29, and extraversion itself was the only personality trait that statistically significantly predicted dementia among the other traits. Additionally, Extraversion also slightly increased the odds of depression leading to dementia in old age to 4.8%. With Agreeableness, depression did not predict dementia. Conversely, Neuroticism, although it improved the model (Hosmer and Lemeshow χ2=8.63), it did not influence how depression predicts dementia. Surprisingly, however, it slightly decreased the odds of developing dementia from depression (from 4.2 to 3.9%). Finally, the addition of all the Big-Five traits into the model improved it only slightly, with the odds at 1.049.
Discussion
Consistent with other studies, our analysis of data from this population-based longitudinal study showed the well-documented association between depression and the development of dementia among older adults (Bellou et al., 2017; Ly et al., 2021; Saczynski et al., 2010; Valkanova et al., 2017). We see this association after adjusting for sociodemographic characteristics, strengthening the legitimacy of this finding. Bryers and Yaffe and Valiengo et al. (2016) reported weak or unclear associations between late-life depression and dementia. The significant association seen in our study suggests otherwise. However, the existence of depressive symptoms prior to T1 was not ascertained. Neuropsychiatry symptoms like depression are sometimes a component of the symptomatic spectrum of dementia (Cerejeira et al., 2012; Yatawara et al., 2018). Though there was a significant increase in depression scores over the study period, there remains a chance that association seen in our study is due to depression as a symptom of dementia in these patients.
Of the sociodemographic characteristics controlled for, increasing age and ethnicity significantly predicted the development of dementia while higher educational attainment was protective. Age and ethnicity have been known to influence the development of dementia (Masel et al., 2010; Momtaz et al., 2013). Two possible mechanisms for the protective effect of education in the development of dementia were suggested by Orrell and Sahakian (1995). First, education improves neuronal networking such that there is a larger pool of neurons that can perform the same functional tasks, delaying the onset of dementia with neuronal aging. Second, higher socioeconomic status and education is more likely to result in a greater neural reserve and premorbid intellect thus slowing the cognitive decline. This reinforces the need to promote early life educational pursuits in the general population which can positively influence cognitive functioning in late life (Lövdén et al., 2020; Momtaz et al., 2013). Though not statistically significant in our study, having a partner positively affected the association between depression and dementia, reducing the likelihood of the latter. Prior studies have shown similar results, which emphasizes the protective effects of healthy long-term relationships and social support in depressed patients (Sjöberg et al., 2020; Sundström et al., 2016).
To explore how the Big-Five personality traits influence the relationship between depression and dementia, we adjusted for the five traits. After including all five traits in the sociodemographic-adjusted model, the significant relationship between depression and dementia remained the same, suggesting no confounding effect of personality traits on this relationship in our study population. However, individually, neuroticism slightly decreased the odds of dementia in depressed patients, while openness, conscientiousness, and extroversion resulted in slightly increased or unchanged odds. These findings were interesting because previous studies have reported higher incidence of dementia in patients with lower conscientiousness and higher neuroticism (Low et al., 2013; Terracciano et al., 2017), and a possible reduced risk of cognitive impairment in patients with higher openness (Ayers et al., 2020).
We expected neuroticism to be strongly associated with higher depression and increase the likelihood of dementia. However, our findings suggest otherwise. Since previous studies did not account for depression, the observed difference may be due to this. A meta-analysis by Kotov et al. (2010) showed that patients with depression scored higher than non-clinically depressed samples on neuroticism, and lower on extraversion and conscientiousness. This association was also seen in a cross-sectional study involving patients with a diagnosis of major depressive episodes (Jourdy & Petot, 2017).
Other findings of interest were observed for agreeableness and extraversion. Agreeableness nullified the effect of depression on the development of dementia in our older adult study population while extraversion was observed to significantly increase the model fit despite no significant difference in the odds (compared to Model 1). Moreover, extraversion was the only personality trait that was significantly related to change in depression. Most studies that explored the relationship between agreeableness and dementia reported a negative association (Aschwanden et al., 2021; Terracciano et al., 2014, 2017). Notably, agreeableness was strongly associated with a better performance of four out of the five cognitive domains in another study (Sutin et al., 2019). These study reports of the positive influence of agreeableness on cognition support our findings on this personality trait nullifying the effect of depression on dementia. However, a longitudinal study identified agreeableness, together with neuroticism, as a major personality trait that can alter parahippocampal cortices of the brain (Block, 1993). The prosocial nature of agreeableness likely has a positive effect, significant enough to slow the development of dementia in older adults with depressive symptoms. On the other hand, being extraverted in old age may significantly increase not only the risk of dementia, but also the strength of depression predilection to dementia.
From the foregoing, our expectation was to find a confounding effect of personality traits given its independent association with both depression and dementia. Our study results instead, suggest that the association between depression and dementia remains the same irrespective of personality traits. This may be because personality traits of our study participants did not change significantly over the 5-year study period. Some previous longitudinal studies also highlighted no personality change in old age (Allemand et al., 2008; McCrae & Costa, 2003), supporting our findings in this large, longitudinal, and population-based sample of older Americans.
One particular strength of this study is that aside from being a population-based sample, the demography (particularly ethnicity) of the sample of older adults’ mirrors that of the US Census report (Roberts et al., 2018). This consolidates the generalizability of our findings. Additionally, it may appear to be the first study to our knowledge to investigate the relationship between these psychosocial factors. Despite the contribution of this study to the understanding of how personality traits influence the association of late-life depression with dementia, this study has limitations. First, the use of secondary data constrained our variables of interest such that we were unable to utilize the first wave of the survey. Second, longitudinal studies require more than two data points for best practices. However, this study utilized two waves of data with two time points. For this reason, we could not claim any causality in the reported associations.
Conclusion
From this study, we conclude that personality traits, overall, do not influence how depression predicts the development of dementia in old age. However, agreeableness and extraversion personality traits may have some impact on this relationship. Prosocial behaviors should be promoted in old age as these appear to be protective. In addition, early life education and a strong social support can keep the depression–dementia spectrum at bay in old age. Future research may explore how personality traits influenced the relationship between chronic depression and the development of dementia in old age.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.