
Abstract
Introduction
The coronavirus (COVID-19) pandemic is becoming the “new normal,” with repeat spikes of infections in communities across the globe (Saito & Haruyama, 2023). It has disproportionately affected nursing homes in the USA in particular, with widespread outbreaks and an excess mortality rate of two to three times more than the general population (Li et al., 2020). The Centers for Medicare & Medicaid Services (CMS) (2021) reported 570,626 nursing home residents’ infections and 112,383 residents’ deaths in the USA before the wide availability of COVID-19 vaccination in 2020 for nursing home residents (e.g., Pfizer, Moderna, and Johnson and Johnson). In the early Delta stages of the pandemic (summer 2021) to winter 2022 (Omicron), nursing home residents were at excessive risk for severe infections and death (United States Government Accountability Office, 2023). There is a need to establish baselines to benchmark new COVID-19 infections due to the various mutations of new variants and thus the introduction of vaccinations and their competing risks. Findings could inform prevention and management strategies for minimizing excess infections and reduce mortality in nursing home residents.
Earlier empirical studies published in 2020 (e.g., Belmin et al., 2020; Bui et al., 2020; Gorges & Konetzka, 2020; He et al., 2020) reported nursing homes’ COVID-19 infection rates were associated with nursing homes’ characteristics such as staff, and resident’s demographic characteristics and the residents’ pre-existing comorbid conditions. Thus, there is a need for a systematic review that aims to integrate the evidence for guiding nursing home care services and their COVID-19 management plans. This has now been described as “the new normal” where the COVID-19 has been described as the virus that is here to stay, similar to the influenza virus. Findings from a systematic review could also inform future related studies on COVID-19 amongst nursing home residents. This is important due to their enormous diversity both in the USA and globally. Specifically, this systematic review aims to summarize the evidence on how the areas in which the nursing home is situated (e.g., counties) as well as how individual residents’ demography are associated with COVID-19 infections in order to guide future research and to inform related interventions.
Conceptual Framework
The conceptual framework for this systematic review was the Geographic Information Systems (GIS) Based Spatial Model (Tomlinson, 2007). The reason that GIS was used is that its GIS allows an extra analysis of information layers in social ecologies such as nursing homes in communities (e.g., counties). The GIS was used to assess these characteristics for patterns in the data suggesting inter-level associations important for planning decisions for prevention (Sugg et al., 2020). The GIS based spatial modeling compares patterns across COVID-19 nursing homes (meso level) to assess environments at multiple levels of vulnerability for prevention intervention.
The GIS-Based Spatial Model was used in this systematic review as it has previously been utilized to examine COVID-19 outbreaks and infections (Franch-Pardo et al., 2020). It was utilized on both the meso (community level) and micro (nursing home characteristics, also resident profiles by demographics and vaccination statuses) levels. Environmental interventions at the community and nursing home levels for preventing and managing COVID-19 infections appear to hold promise, beyond what is possible with person level interventions only (Palese et al., 2022).
Community-Level Factors
In the 2020s, it appeared that there was variability in COVID-19 infection prevalence rates at the county level in the USA (Bui et al., 2020; Gorges & Konetzka, 2020; Sun et al., 2020; White et al., 2020), suggesting contextual influences. In addition, high population density, locations (e.g., urban locations in the early pandemic), and subsequently high certificate of need (CON) laws have impacted nursing home residents’ COVID-19 infection rates (Gmehlin et al., 2021; Klompmaker et al., 2021; Sun et al., 2020). Thus, this review investigated those community-level factors that were related to COVID-19 infections in order to provide information for healthcare departments to enable them to monitor and evaluate the transmission of COVID-19 at the macro level. Thus in the future, health departments may be able to organize approaches for efficient implementation of preventative measures for nursing homes.
Nursing Home Characteristics and Staffing
Larger nursing home facilities or those who failed to pass quality assurance had more residential COVID-19 infections (Gmehlin et al., 2021; Lane et al., 2022; Yin et al., 2021). Also, those who were privately owned and had low mask usage were also associated with higher COVID-19 infection rates (Abrams et al., 2020; Figueroa et al., 2020; Simoni-Wastila et al., 2021; Yin et al., 2021). However, in contrast, larger size nursing homes often had better resourcing and higher quality ratings, which would minimize risk for COVID-19 infections (Figueroa et al., 2020; Gopal et al., 2021). Staffing levels and registered nurse hours were also associated with higher COVID-19 prevalences/rates (Gorges & Konetzka, 2020; Shi et al., 2020; Sun et al., 2020; Xu et al., 2020), likely from the asymptomatic staff spreading infections and who were unable to take time away from work (Belmin et al., 2020; McGilton et al., 2020). However, there is conflicting evidence regarding how nursing homes’ qualities (e.g., star ratings) affected residents’ risk for COVID-19 infections (He et al., 2020; White et al., 2020).
Personal Resident Factors
Personal factors such as minority background (e.g., African Americans and Hispanic), gender (male), older age, and higher frequency of travel among individuals dwelling in higher-income communities have been associated with risk for infections, especially for nursing home residents with Medicaid (Bailey et al., 2020; Zhang & Schwartz, 2020). For example, more African Americans and Hispanics had higher prevalence of COVID-19 infections (He et al., 2020; Mehta & Goodwin, 2021). In one study, it was found that male residents in nursing homes had a two-fold possibility of being infected compared to female residents (Shi et al., 2020). Another study reported older adult age was a risk factor for COVID-19 (Chen et al., 2021). In addition, past and present infections pre-existing chronic illnesses and decreased capabilities in activities of daily living were also reported as risk factors for COVID-19 infections (Bigelow et al., 2020; Shi et al., 2020).
The Present Study
The systematic review studies conducted previously focused on long-term care facilities (e.g., assisted living, senior housing) (Bach-Mortensen et al., 2021; Konetzka, White et al., 2021). As residents in nursing homes are more vulnerable to COVID-19 due to their multiple chronic conditions and high chances of mortality, a more focused systematic review is needed to expand on risk factors in these populations. Although a scoping review (Giri et al., 2021) investigated factors associated with the severity or the mortality of COVID-19 as of January 2021, there was a need for such a review to investigate relationship between COVID-19 infections and more individual, social, and demographic risk factors not investigated by Giri et al in the nursing homes.
This mixed-method systematic literature review aims to summarize the research evidence of nursing home care and residents’ personal risk factors associated with COVID-19 infections over the pandemic period (January 1st, 2020 to October 31st, 2022) in the USA.
The specific research question was: What are the risk factors associated with nursing home residents’ COVID-19 infections over the critical pandemic period (January 1st, 2020 to October 31st, 2022) in the USA?
It is hoped that the findings of this systematic review will provide evidence that will inform the pandemic preparedness of nursing home care services and add to the growing body of literature for future related studies on resident’s COVID-19 infections in the USA.
Methods
Research Design
This present systematic review protocol is registered with PROSPERO (CRD42023469015).
This mixed methods systematic review integrated evidence from both qualitative and quantitative studies. “Mixed methods systematic reviews (MMSRs) have become an important development in evidence-based health care as they maximize the ability of review findings to assist in clinical and policy decision-making” (Stern et al., 2021). These authors concluded that health systems managers found MMSR to be more credible for providing guidance on evidence-based decisions than they would with single method approach findings (Stern et al., 2021). Ethics approval and informed consent are not applicable for this present systematic review.
Search Strategy
The literature search included four databases (PubMed, Web of Science, Scopus, and Sage Journals Online), and the search terms were (“nursing homes” OR “care homes” OR “long term care” OR “residential care” OR “aged care facility”) AND (“COVID-19” OR “coronavirus” OR “2019-ncov” OR “cov-19” OR “sars-cov-2”) AND (“residents”) AND (“factors” OR “causes” OR influences” OR “reasons” OR “determinants” OR “predictors”) AND (“United States” OR “America” OR “U.S.” OR “USA”).
Selection Criteria
Studies were included if they met the following criteria: (a) articles were published between January 1st, 2020 and October 31st, 2022, and in the English Language. The country and the setting were restricted to skilled nursing home facilities in the USA. Studies where included if employing either quantitative, qualitative, or mixed analytical research designs.
The exclusion criteria were: (a) irrelevant to COVID-19 infections, (b) written in languages other than English, (c) comments, recommendations, letters, or editorials, not full research papers, and (d) countries other than the USA. A library reference librarian assisted our searches to maximize the yield.
Search Outcome
The predefined search strategy initially identified 579 records (99 in PubMed, 77 in Web of Science, 70 in Scopus, 333 in Sage Journals Online, and 2 from other sources), resulting in 390 articles after removing duplicates. After using a combination of Medical Subject Headings (MeSH) and text-word to screen the title, abstract and full-text, a further 310 articles were removed, 80 articles sought for retrieval. Except one report not retrieved, assessment for eligibility resulted in 48 articles for the systematic review (Appendix 1) and excluded 31 articles with reasons (e.g., subjects not in nursing homes, articles not relevant to COVID-19 factors, and staff subjects) (Appendix 2).
Risk of Bias and Quality Assessment
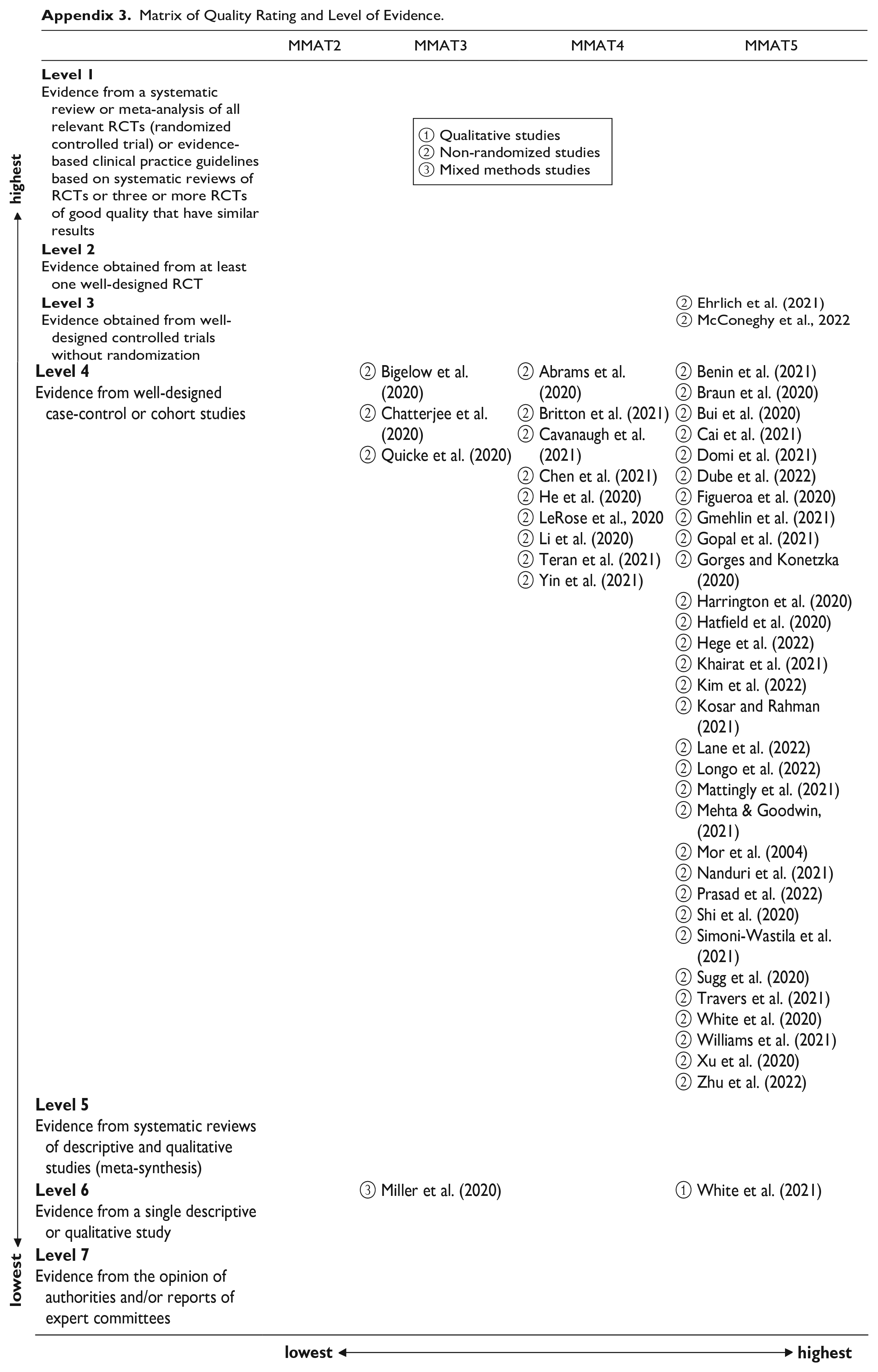
Bias assessment was implemented through the usage of the Mixed Methods Appraisal Tool (MMAT), and each qualified study was appraised as low or high bias against the methodological quality of studies across five categories (qualitative, quantitative randomized controlled trials, quantitative non-randomized, quantitative descriptive, and mixed methods) (Hong et al., 2018). The value of the MMAT exists in its capacity to evaluate the appropriateness and accuracy of the methods utilized and the risk of bias in a study, thereby enhancing the overall reliability and validity of the findings (Hong et al., 2018). For example, the MMAT provides sampling strategies to evaluate whether a sample size in a study can represent the target population, which helps reviewers determine any biases or issues that are caused by inadequate sampling. The MMAT was applied at the outcome level. The Levels of Evidence or Hierarchy of Evidence (Ackley et al., 2008) utilized at the study level were used to map each article’s quality based on the different types of research studies from level 1 (lowest level) to level 7 (highest level) on the vertical line (See Appendix 3 for the matrix of quality rating and level of evidence).
Data Extraction
The data extraction prioritized studies based on known risk factors associated with nursing home residents’ COVID-19 infections utilizing the Geographic Information Systems (GIS) Based Spatial Model as a framework (Sugg et al., 2020) (Appendix 4). These factors were abstracted and then categorized into different levels (geography, demography, nursing home characteristics, staffing, resident’s characteristics, and COVID-19 vaccination status).
Three Reviewers independently screened the titles, abstracts and full-body of articles and then evaluated the full contents of those selected articles associated with nursing home residents’ COVID-19 infection status. Data from prioritized studies were extracted by applying the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines (PRISMA) guidelines (Page et al., 2021). Disagreements were handled by the first reviewer RefWorks software was employed to find and delete duplicated articles.
Data Synthesis
A narrative synthesis (Popay et al., 2006) was then conducted for the prioritized studies (n = 48) which depended primarily on using the MeSH and text-word to identify common findings and themes from multiple studies. The narrative synthesis fitted this review because of the inconsistencies in the reporting of associations between the included variables and COVID-19 infections.
Following the guidelines of the systematic review without meta-analysis (SWiM) (Campbell et al., 2020), the first listed author conducted a thematic analysis and assessed the extracted evidence for coherence, followed by checks by the second listed author. Any discrepancies were resolved by checks by the third listed author and consensus discussion Subsequently, the first listed author categorized the evidence based on recurring themes and variables applying the GIS model (Sugg et al., 2020) by nursing home contexts, offering a concise summary of key findings and then analyzing variations across studies, for verification by the third listed author. The synthesis was performed in a narrative description that weaved the key findings and the implications of the combined evidence from mixed-method studies. The other two reviewers scrutinized and validated the collated evidence and confirmed the results of the first reviewer.
Results and Discussion
This mix-method literature review is the first investigating risk factors associated with nursing home residents’ COVID-19 infections in the USA into six major areas: factors associated with geography, demography, type of nursing home, staffing in nursing home, resident’s status, and COVID-19 vaccination status. These indicators are important for policy and practice improvements as well as for intervention research studies as discussed below.
Forty-eight articles referring to nursing homes in the United States and published between January 2020 and October 2022 were selected in November 2022. Table 1 describes articles included for review in the order of author/year, number of settings/participants, study design, and key factors the adapted levels of evidence by Ackley et al. (2008), 92% articles were classified as observational studies, indicating a mid-rating of methodological quality in the study field. Adopting the MMAT, 92% of articles were graded as four or five points based on their study design, reflecting a low bias and a high quality of these studies.
Basic Characteristics of Included Studies in the Systematic Review.

Note. CA = California; CO = Colorado; CT = Connecticut; DE = Delaware; FL = Florida; MD = Maryland; WV = West Virginia; KY = Kentucky; GA = Georgia; IL = Illinois; MA = Massachusetts; NJ = New Jersey; PA = Pennsylvania; WI = Wisconsin; AR = Arkansas; MI = Michigan; NM = New Mexico; UT = Utah; VT = Vermont; ND = North Dakota; SC = South Carolina; VA = Virginia; TN = Tennessee; NC = North Carolina; MS = Mississippi; AL = Alabama; AZ = Arizona; WA = Washington; NV = Nevada; TX = Texas.
More specifically, 2 control trials articles (range of nursing homes 34–196), 9 retrospective cohort (range of nursing homes 2–15,038), 7 case-control (range of nursing homes 1–15,236), 28 cross sectional (range of nursing homes 1–15,390), and 2 either qualitative or mixed method were identified.
Themes
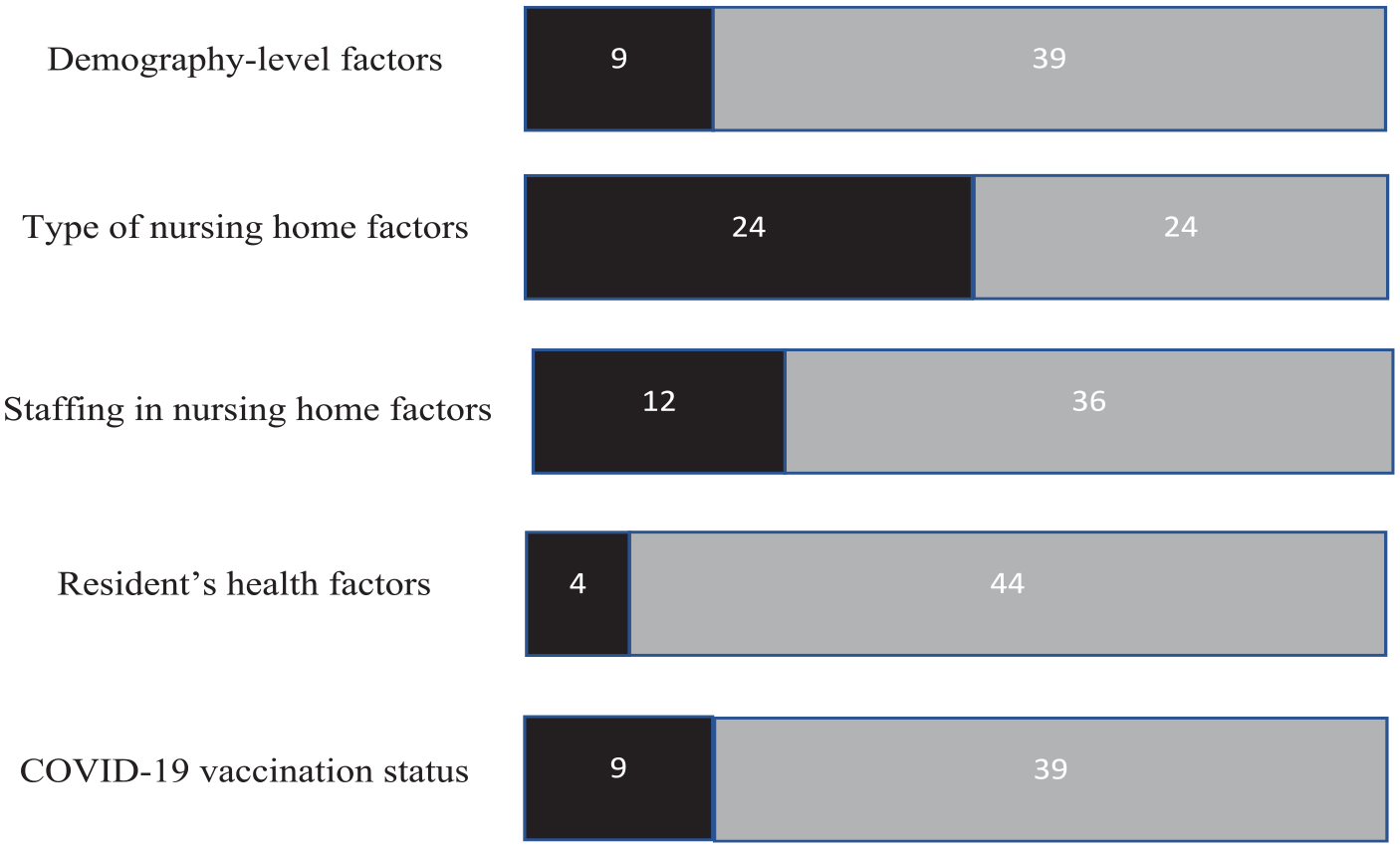
Six major themes of risk factors in the studies included were explored and categorized: geography, demography, type of nursing home, staffing in nursing home, resident’s health, and COVID-19 vaccination status. Ten out of 48 studies (21%) identified geography, 9 (19%) evaluated demography, 24 (50%) estimated type of nursing home, 12 (25%) determined staffing in nursing home, 4 (9%) analyzed resident’s health, and 9 (19%) investigated COVID-19 vaccination status (see Figure 1 for a summary of reported/unreported studies).
Overview of study findings based on the modified GIS model framework and four main themes.
Geography
In summary, geography-level factors related to COVID-19 prevalence included COVID-19 prevalence in counties, counties with population density, and locations (urban/rural).
Nursing home’s county’s infection prevalence/rate was the strongest predictor of resident infections (Gorges & Konetzka, 2020; Sun et al., 2020). Bui et al. (2020) and Mattingly et al. (2021) described it as a strong factor contributing to nursing home infections (e.g., OR = 4.38, 95% CI = 2.24, 8.56). If the county had a higher COVID-19 prevalence, nursing homes located in that area experienced higher risks of admitting new residents with COVID-19 or the virus being introduced via serving staff (White et al., 2020). Gorges and Konetzka, (2020) reported that nursing homes’ COVID-19 infection cases in the top 20th percentile of counties’ infection rate were at least six-fold higher compared to these nursing homes located in the bottom 20th percentile of counties’ infection rate.
Population density was also a risk factor, and thus counties with high population density had a higher likelihood of COVID-19 infections in nursing home residents (Sun et al., 2020). As COVID-19 is a respiratory virus, transmission is rapid among individuals living in high-density areas (see also Zhang & Schwartz, 2020). Thus, nursing homes in high population density areas had a greater risk of suffering outbreaks and infections. However, Sugg et al. (2020) reported that such a relationship was only proven in eleven states, such as California, Nevada, Missouri, Kansas, Iowa, and Indiana. Until September 2020, nursing homes located in urban areas were identified with higher COVID-19 incidences. However, since this time, COVID-19 incidence has increased significantly in rural nursing homes (Gmehlin et al., 2021).
Demography
In summary, demography-level factors related to COVID-19 prevalence included percentage of the total Africa Americans or Hispanic population in counties, percentage of Africa American, Hispanic, and Asian residents in nursing homes, older age, male gender of residents, per capita income and Medicaid-based residents.
Minority Status
There was a higher prevalence of COVID-19 infections in a home with counties who had a higher percentage of minority populations (Hispanics, African Americans, and Asians) (Sugg et al., 2020). This is supported by evidence that the COVID-19 prevalence was higher (OR = 1.27) in counties with a higher percentage of African Americans. In addition, the rate was much more significant in the Southern USA states, such as Texas, Florida, and Louisiana (Sugg et al., 2020). It has been hypothesized that the COVID-19 deaths may be due to higher incidence of underlying health conditions and less access to medical care among minority populations (Patel et al., 2020; Thomeer et al., 2023). This further reveals the racial and ethnic health disparities in the USA (Gorges & Konetzka, 2020).
A higher percentage of racial and ethnic composition of nursing home residents (e.g., African Americans, Hispanics) was found to be a risk factor for COVID-19 infections (Cai et al., 2021; He et al., 2020; Mehta & Goodwin, 2021). Another correlated factor was that nursing homes with a higher percentage of African American residents were more reported to be likely to experience staff shortages and financial restrictions and have Medicaid-dependent residents (Travers et al., 2021). There were severe health disparities in COVID-19 prevalence and its related mortality during the pandemic (Abrams et al., 2020).
Older Age
Advanced age was reported that positively associated with resident COVID-19 cases (Chen et al., 2021). This may be because those who had more pre-existing chronic conditions required more healthcare services and had more close interactions with staff, which increased the likelihood of being infected with COVID-19 (McGilton et al., 2020).
Sexual Status
Men were reported to have a higher rate of COVID-19 infections in nursing homes compared to women (OR = 2.00) (Shi et al., 2020). Although unproven X-linked genetic differences and androgen promotion of TPRSS2 are hypothesized as being a causal factor and in addition different gender-based personality factors such as risk-taking, impulsivity in men were suggested as affecting high levels of perceived loneliness.
Per Capita Income
Bailey et al. (2020) determined that individuals dwelling in higher-income communities tended to travel and thus introduced COVID-19 to communities during the early pandemic. As the pandemic spread sharply in the USA, lower income and/or poverty became a risk factor associated with increased COVID-19 infections in poorer counties (Zhang & Schwartz, 2020). Sugg et al. (2020) reported decreased COVID-19 infections in nursing homes located in high per-capita income communities compared to these nursing homes in low per-capita income communities.
Medicaid-Based Residents
Medicaid-based residents were found to be associated with increased COVID-19 prevalence because these nursing homes were more likely to have insufficient clinical and financial resources compared to their counterparts, and they tend to be located in communities with lower socioeconomic situations. Thus as previously reported, residents who receive poorer quality of care also experience worse health outcomes (Li et al., 2020). Medicaid-based nursing homes experienced more COVID-19 outbreaks and infections than Medicare-based nursing homes due to the disparities noted above (Chatterjee et al., 2020). Li et al. (2020) reported that Medicaid residents had a higher chance of being infected compared to their counterparts (incidence rate ratio = 1.16).
Types of Nursing Homes
In summary, nursing home-level factors related to COVID-19 prevalence included number of beds, historical health deficiencies, count of fines, star rating, number of separate units in nursing homes, governmental and private ownership, percentage of facility-wide testing, pass quality assurance check, proportion of short-stay residents, shortage of N95 masks, the Certificate of Need (CON) presence, and staff and resident density.
Nursing Home Size
Nursing home size had a dominant association with residents’ COVID-19 infections in many studies (Harrington et al., 2020; White et al., 2020; Yin et al., 2021). It was found that the number of separate units in nursing homes was a substitute for the size of nursing homes (Sun et al., 2020). Specifically, in many studies, larger facilities experienced a higher possibility of COVID-19 outbreaks and infections due to more employees and admissions (Gmehlin et al., 2021; Kosar & Rahman, 2021; Mattingly et al., 2021; Ryskina et al., 2021; Zimmerman et al., 2021). Inversely, smaller nursing home facilities experience fewer infections (Abrams et al., 2020).
Nursing homes with CMS cited historical health deficiencies (e.g., staffing insufficiencies, resident’s neglect, or abuse, and dietary and nutritional deficiencies) or a record of frequent fines for violations (e.g., non-compliance with CMS infection control regulations) had an increased likelihood of residents’ COVID-19 cases (OR ranges from 1.05–1.26 based on counties) (Harrington et al., 2020; Sugg et al., 2020).
Star Rating
As a corollary of the above Quality Assurance measure, nursing homes with lower star ratings were more likely to have COVID-19 outbreaks and infections (Figueroa et al., 2020; Gopal et al., 2021; Williams et al., 2021). It has been hypothesized that lower star ratings led to lack of the improvement of resident’s health outcomes because of reduction of nursing home costs (He et al., 2020). However, it was reported that lower-star-rated nursing homes were generally located in higher COVID-19 prevalence areas and had more vulnerable residents who were impacted by worse demographics compared to higher-rated nursing homes (He et al., 2020; Khairat et al., 2021; Li et al., 2020), and thus the star rating was a marker for socioeconomic level and demography.
Types of Nursing Homes
Privately-owned nursing homes experienced more COVID-19 residential infections when compared with non-profit and government-owned nursing homes. However, it has been reported that this was due to the lower quality of care provided to residents in privately nursing homes (Braun et al., 2020; He et al., 2020). However, in contrast, one study (Gmehlin et al., 2021) concluded that governmental ownership was associated with increased COVID-19 infections within facilities, which was inconsistent with the above-mentioned studies and probably dues to different counties. This discrepancy could be a marker of the fact that Gmehlin was reporting infection rates in 2021 and also the difference in the prevalence of COVID-19 in different counties (Gmehlin et al., 2021).
Nursing homes with enough resources to implement facility-wide COVID-19 testing were found to be able to identify initial cases in asymptomatic residents and staff. Thus testing helped nursing homes regulate infection prevention and thus further effective preventive strategies. Hatfield et al. (2020) reported that nursing homes that conducted facility-wide testing identified eight times higher COVID-19 cases compared to those that did not (25.7 vs. 3.5 on average). Unfortunately, in the early stages of the pandemic, limited testing supplies prompted stringent testing requirements in nursing homes (Ouslander & Grabowski, 2020). Consequently, residents had to exhibit more symptoms before being eligible for a test, increasing the likelihood of infections in the constrained PPE environment. As the pandemic progressed, there was an improvement in the availability of tests and PPE supplies, allowing for testing without the necessity of symptoms (Konetzka, 2021). Despite concerns that variations in testing supplies and PPE availability might introduce biases in COVID-19 infection data between the early (January–December 2020) and later pandemic (January 2021–October 2022) phases, our study reveals that over the later pandemic, the patterns of COVID-19 infections in nursing home residents were centered on COVID-19 vaccinations (see Table 1, study date), while there was no any study focused on other perspectives.
Quality Assurance
Quality assurance refers to “the specification of standards for quality of services and outcomes, and a process throughout the organization for assuring that care is maintained at acceptable levels in relation to those standards” (CMS, 2016). Thus, quality assurance evaluates quality of staffing levels, safety measures, resident’s care, and compliance with regulations (CMS, 2016). Nursing homes that did not meet these quality checks and then failed Quality Assurance (QA) experienced more total counts of fines or total health deficiencies; therefore, hence had a higher likelihood of COVID-19 infections (SE beta = 1.98) (Yin et al., 2021).
Masks
Deficiency in the availability of N95 masks was a risk factor for increased COVID-19 cases in nursing homes. It is well known that N95 masks prevent COVID-19 spread and penetration (Li et al., 2020). Thus the COVID-19 prevalence was reported to be higher in nursing homes with shortage of N95 masks compared to those with sufficient N95 masks (OR = 1.21), highlighting the role of N95 masks especially during the early phase of the pandemic (Simoni-Wastila et al., 2021).
Nursing Homes With Short Stay
A short-stay residence is defined as a period of care in nursing homes of less than 100 days. Nursing homes with a higher proportion of short-stay residents were more likely to have COVID-19 outbreaks and infections in the early pandemic (Mattingly et al., 2021). This was probably because of higher chances of introducing the virus into the facilities from these short-stay residents who also required more care compared to long-stay residents. This then resulted in more interactions and thus introduced and transmitted the virus within facilities. Mattingly et al. (2021) proposed a possible intervention, which was to separate short-stay and long-stay residents into different units in nursing homes.
The certificate of need (CON) laws are state-level regulatory mechanisms for controlling healthcare expenditures by avoiding overlapping services or unneeded expansion (National Conference of State Legislatures, 2023), and it, as one of the healthcare policies in the long-term care field, impacts the size of a nursing home indirectly. Nursing homes located in counties under the CON laws documented additional 104 COVID-19 cases than those were not subject to the CON, on average (Kosar & Rahman, 2021). Larger nursing homes had more employees and thus admissions, resulting in greater risks of introducing COVID-19 into nursing homes (Abrams et al., 2020; Gmehlin et al., 2021).
Density
As with geographic density, both staff and resident density were positively associated with resident infections within nursing homes (Sun et al., 2020). Nursing homes with a higher staff density had more employees and thus more frequencies of exposure from the outside community. Additionally, higher staff and resident density had subsequently more interaction between staff and residents, and residents thus were more likely to be exposed to COVID-19 exposure. Zhu et al. (2022) found that by reducing density in nursing homes COVID-19 cases could be reduced. Sun et al. (2020) proposed that by reducing occupied beds rates could be a strategy to manage early transmission in the pandemic. However, an unintended consequence was that this strategy impacted nursing homes that were depended on Medicare revenue.
Staffing in Nursing Home
Risk factors at the staff level are categorized into different types, including but not limited to staffing levels, number of registered nurse hours, high COVID-19 prevalence/rate in the staff residence, and asymptomatic subjects.
Staffing Numbers and Types
Higher total staffing levels were examined as a protective factor for nursing home residents’ infections in the USA (Harrington et al., 2020). On the contrary, inadequate staff levels or staff shortages were related to higher residential COVID-19 infections (Li et al., 2020; Yin et al., 2021). Interestingly, shortage of clinical staff and licensed nurse staff was reported as more significantly related to COVID-19 rather than nurse aids (Xu et al., 2020). It has been reported that staff shortage of nurses resulted in deficient care, lower standards of monitoring, and thus worse resident outcomes during the COVID-19 pandemic (Belmin et al., 2020; Palese et al., 2022).
In addition, a greater level of licensed practical nurses (LPN), nurses (not registered nurses), and certified nursing assistants, compared to registered nurses, were found to be associated with increased resident infections. And the result might be due to interacting closely with more residents and their working experience and environment (e.g., less training, lower pay) (Dube et al., 2022; Sugg et al., 2020). The reason for this finding was thought to be that the level of qualified staff who were paid less often increased the possibility of spread the virus into nursing homes (Ladhani et al., 2020).
Staff Residence
Staff’s residence was the most dominant factor in residents’ infection. This association was similar to COVID-19 prevalence in counties at the external level, as staff who lived in high COVID-19 prevalence areas had a greater likelihood of being infected (symptomatic or asymptomatic) and unwittingly introduced the virus into nursing homes (Shi et al., 2020). Similarly, untested asymptomatic staff were predictors of increased residential infections (Quicke et al., 2020). Interestingly, Lennon et al. (2020) reported that over 90% of staff working in assisted living and skilled nursing facilities in Massachusetts were tested as asymptomatic. This facility-wide COVID-19 prevention and management, based on facility-wide testing strategies or availability of adequate PPE supplies, was debated in the literature (Telford et al., 2021).
Nurse Hours
Registered nurses who worked large numbers of hours were found to increase resident infection rates in such facilities (Gorges & Konetzka 2020). A possible explanation was hypothesized that nursing homes were shortage of staff and were difficult to recruit more staff. And thus, these hired registered nurses needed to work longer than before.
In addition, the qualitative studies conducted by White et al. (2021) and by Miller et al. (2020) reported factors as
(a) fears of being infected within facilities under the shortage of PPE and testing
(b) burnout due to staff shortage and increased workload,
(c) lack of team cooperation and organizational communication during the pandemic and
(d) a lack of preparedness for COVID-19 within facilities and access to PPE for direct-care workers. These four explanations were also identified as risk factors for resident’s infections.
Asymptomatic Subjects
Either asymptomatic staff or residents who are asymptomatic unwittingly spread the virus within nursing homes without adequate COVID-19 testing (Shi et al., 2020). One study (Arons et al., 2020) identified that 56% of residents were diagnosed as asymptomatic in a nursing home. This finding provides important information for the challenges facing formulation of policies for COVID-19 prevention with hopefully future universal testing.
Resident’s Health
In summary, resident’s health factors related to COVID-19 prevalence included dialysis demands, diabetes, hypertension, higher BMI, and more bowel incontinence, lower Social Vulnerability Index (SVI), activities of daily living scores, smoking, and asymptomatic residents.
Chronic Illnesses
Residents who required hemodialysis were a notably vulnerable population and were more likely to be infected during the pandemic due to the frequency of transport to dialysis centers and interactions with staff members (Bigelow et al., 2020). These residents were a possible source for the virus transmission into nursing homes and might be an undiagnosed (asymptomatic) source for both nursing homes and dialysis centers (Bigelow et al., 2020). Likewise, residents with bowel incontinence, diabetes, hypertension, high BMI, or smoking increased close contact with staff and exposed themselves to higher risks of virus contingence (Mehta & Goodwin, 2021; Shi et al., 2020).
It was found that when COVID-19 policies and nursing homes’ regulations (e.g., lockdown, keeping social distance) were implemented, residents subsequently had reduced Activities of Daily Living (ADL) (Trevissón-Redondo et al., 2021). In addition, nursing homes ranked in lower quartiles of the Social Vulnerability Index (SVI) experienced more total counts of fines or total health deficiencies; therefore, their residents had a higher likelihood of COVID-19 infections (LeRose et al., 2021).
COVID-19 Vaccination Status
As discussed in the previous section, risks for infections were higher among the unvaccinated residents. Benin et al. (2021) pointed out that nursing homes with initial vaccinations had 27% lower infection cases than those that did not start the vaccinations in early 2021. Nanduri et al. (2021) investigated the effectiveness of vaccinations (EV) (vaccinated vs. unvaccinated) during the Delta period and reported a 51% to 53% EV range, which was lower than the EV before the Delta period (74.5% on average). A newly published study (McConeghy et al., 2022) reported a lower EV against infections (26%); however, the EV against hospitalization, death, and severity of COVID-19 was significantly improved (60.1%, 89.6%, and 73.9%, respectively).
Implications, Limitations, and Future Directions
The rapid dissemination of COVID-19 and its repercussions present one of the most notable challenges for nursing homes in recent years. With over 40 scientific articles published on this subject over the COVID-19 pandemic, it is essential to convey the primary findings through a thorough review of the available evidence. This systematic review extracted and synthesized six key themes of COVID-19 infections among nursing home residents in the USA from the available literature. Based on the collated evidence, most studies focused on nursing home characteristics and staffing factors. Although the systematic review primarily centered on COVID-19 infections in US nursing homes, more comprehensive studies have been identified to investigate the impact of staff on residents COVID-19 infections and the strategies for preventing and managing such infections. As an example, Belmin et al. (2020) revealed that in French nursing homes where staff confinement with residents was not implemented, there was a higher incidence of COVID-19 infections and mortality, indicating a critical role for staff confinement in mitigating the spread of COVID-19. Furthermore, Palese et al. (2022) suggested comprehensive interventions at the environment level to combat COVID-19 in Italian nursing homes. These interventions encompassed nine domains, including the reorganization of expanding services, the augmentation of nursing care, ensuring adequate staff levels, and delivering specialized training (Palese et al., 2022). To bolster support for staff in nursing homes, McGilton et al. (2020) put forth various recommendations encompassing the provision of clear direction and guidance, prioritizing staff health, implementing human resource polices, and incorporating new clinical practices related to COVID-19.
This review makes the unique Geographic Information Systems (GIS) Based Spatial Modeling framework to suggest a need to prioritize universal COVID-19 vaccination interventions in COVID-19 mitigation at nursing homes, while also employing selective interventions by community-level factors; nursing home characteristics and targeted interventions by resident socio-demographic and personal characteristics. According to the modified GIS model as a framework, nursing home COVID-19 safety should focus on context and personal factors simultaneously.
Implications for Clinical, Professional, and Policy Practice
The evidence from this review has implications for clinical, service, and policy practices.
Clinical
The results of this review suggest that while universal COVID-19 vaccination interventions reduced risk for excess mortality from COVID-19, nursing homes still endure high mortality rates among residents with COVID-19 (CMS, 2021), emphasizing that interventions are needed to consider and take into account personal factors of residents, community factors, and nursing home characteristics while switching the focus from infections to the severity/mortality of COVID-19 and COVID-19 vaccinations. While studies have demonstrated the effectiveness of COVID-19 vaccinations in preventing infections and reducing severity, there is a growing apprehension regarding the ethical considerations associated with these vaccines and resident autonomy (Benin et al., 2021; McConeghy et al., 2022; Nanduri et al., 2021).
There is evidence to suggest that “a sub-acute setting of care (e.g., providing oxygen and treatments), considering the facility to be the right place to care for residents” may provide better clinical care than with hospital admissions (Palese et al., 2022). Prospectively, nursing home need to invest into their subacute care resources, including staff training for timely on-campus resident monitoring and care.
Professional
Nursing homes could consider both nursing home characteristics and resident personal resident factors for improved COVID-19 risk management. The findings of nursing home characteristics suggest that residents experience high risk of COVID-19 exposure when their facilities endure multiple deficiencies, limited funding, a shortage of PPE and lack of vaccines. Evidence from these studies has shown that these factors lead to poor management and control of COVID and lead to more vulnerability for residents. In addition, lack of staff and high workloads caused staff burnout and fear of infection. Inadequate organizational communication induced insufficient COVID-19 management and control and manifested psychological burdens on staff and residents, especially for the residents in the initial lockdown period. Precariously low nursing home staffing levels and staff work overload are known risk factors for COVID-19 infections (Belmin et al., 2020; McGilton et al., 2020).
Policy
This review suggests that there is a need to manage COVID-19 infections while considering mental wellness amongst residents and staff (McGilton et al., 2020). It also identifies the importance of community factors (e.g., high COVID-19 prevalence in counties especially when with high minority composition) on nursing home residents’ COVID-19 prevalence. Whilst chronic illnesses are common in older adults, they are also an important comorbidity to COVID-19 infection rates in nursing homes. Self-isolation practices by nursing home staff and residents appear to hold great prospects for containing community spread diseases like COVID-19 (Belmin et al., 2020).
Lower occupancy was seen as a protective predictor of residents’ COVID-19 infections and thus may be one potential strategy utilized in future (Sun et al., 2020). However, such implementation causes financial issues, such as increased resident management costs and curtailed Medicare revenue (Grabowski & Mor, 2020). Moreover, practitioners may endure low occupancy penalization, which indicates potential unexpected consequences. We believe that the management and prevention of residents’ COVID-19 infections should not merely center on any specific category of factors.
Limitations of the Review and Suggestions for Further Research
The limitations of this mixed methods systematic review research are twofold: First, while a mixed methods systematic review has the strength of being inclusive, they also carry the limitation of subjectivity in interpreting the findings in contrast to systematic reviews and meta-analysis of purely quantitative studies. Secondary, all articles for this review focused on the USA; therefore, these risk factors may not apply to nursing homes in countries other than the USA. Another limitation is that this review only categorized factors associated with COVID-19 infections rather than factors related to the actual severity and mortality of diseases stemming from COVID-19 infections. Some factors may interact to produce both COVID-19 infections and their severity; however, further studies are required to center on those factors.
Additionally, the search strategy for this review was limited to studies that were published in the English language, which excluded some relevant articles in other languages. Although vaccinations were included in this review, for almost half of the time period considered vaccinations were not available. Significantly, existing studies on COVID-19 infection in nursing homes have not clearly demonstrated its connection with cognitive diseases. Further research is recommended to specifically investigate the correlation between COVID-19 severity and mild cognitive decline, subjective cognitive decline, and dementia.
Conclusion
This systematic review study categorized risk factors associated with COVID-19 amongst nursing home residents into six major types during the pandemic based on the GIS model framework: factors associated with geography, demography, type of nursing home, staffing in nursing home, resident’s status, and COVID-19 vaccination status. Findings suggest nursing home characteristics of large nursing homes with lower star ratings, and asymptomatic staff to be associated with an increased risks for COVID-19 infection rates. Also, nursing homes with a low percentage of fully vaccinated residents or without COVID-19 (regardless of size of facility) had lower rates of COVID-19 infection and death. Personal factors such as residents with advanced age, racial minority, and chronic illnesses were at higher risk for COVID-19 infections. County-level infection rates were an important context for the risk of infection in nursing homes and also at the person level of their residents. Prioritizing universal COVID-19 vaccination interventions at nursing homes, nursing home safety characteristics, and targeted interventions by resident’s personal characteristics may lead toward long-term COVID-19 risk reduction for nursing home residents in the USA.
Footnotes
Appendix
Matrix of Quality Rating and Level of Evidence.

|
Acknowledgements
N/A.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
The systematic review presented in this manuscript did not require Institutional Review Board (IRB) approval because it did not involve primary data collection or human subjects. As such, the study was exempt from IRB review under the regulations and guidelines. Specifically, the study did not meet the definition of “research involving human subjects” as outlined in 45 CFR 46.102(f) of the Common Rule, which states that research involving only the collection or study of existing data, documents, records, pathological specimens, or diagnostic specimens is not considered to involve human subjects.
HIPAA Identifiers
The authors certify that they have complied with the Health Insurance Portability and Accountability Act (HIPPA) in the conduct of this systematic review. The review did not involve the collection of patient health information, and all data used in the analysis were obtained from previously published studies that had already been de-identified. As such, no patient consent was required.