
Abstract
Introduction
Alzheimer’s Disease and Related Dementias (ADRD) is a series of progressive diseases that affect brain function in older adults and leads to challenges in memory, language, and cognitive function (Alzheimer’s Association, 2023). There are currently 6.7 million adults in the US with ADRD and this is projected to grow to 13.8 million by 2060 (Alzheimer’s Association, 2023). Conditions such as cardiovascular disease, diabetes, hypertension, and depression, are common comorbidities among patients with ADRD (Santiago & Potashkin, 2021). As such, there is a need to establish reforms to create high-quality care plans for patients with ADRD, including patients with ADRD and co-existing multiple chronic conditions (MCC).
The emergency department (ED) is a common source of care for patients with ADRD, as the Centers for Medicare and Medicaid (CMS) reports an annual ED visit rate of 1,545 per 1,000 Medicare beneficiaries with ADRD (U.S. Centers for Medicare & Medicaid Services, 2021). Older adults with ADRD are reported to use and return to the ED at higher rates and have higher mortality rates after an ED visit than patients without ADRD (LaMantia et al., 2016). Previous research found various care challenges for persons with ADRD such as a lack of information sharing between health care providers and limited information about disease progression that can lead to a reliance on ED care (Jacobsohn et al., 2019), which accentuates a desire to examine emerging hospital-based features on care outcomes for the difficult health needs of patients with ADRD.
Health information exchange is a feature adopted by some hospitals that provides clinicians with comprehensive patient information from multiple sources of care with the potential to enhance emergency care (Shapiro et al., 2016). Previous research found that health information exchange is associated with improved ED care through faster access to patient information from outside organizations which is associated with lower hospital charges and the likelihood of hospital admission (Everson et al., 2017). Health information exchange also provides clinicians with information such as county and ZIP code social determinants of health which can be combined with patient records to create better predictive models of emergency department revisits (Vest & Ben-Assuli, 2019). Electronic information exchange can also produce efficiency gains in health care by documenting health services to avoid duplicate lab and imaging tests (Pylypchuk & Johnson, 2022).
While limited, previous research on the ADRD population has shown certain types of health information technology (HIT) functionalities may reduce preventable ED visits, such as hospital-HIT patient engagement, a measure of health information exchange between patients or a patient proxy and hospital providers (N. Wang et al., 2021; N. Wang & Chen, 2023).
Yet, there is a lack of evidence surrounding HIT and preventable ED visits for patients with ADRD during the COVID-19 pandemic. This is an important period to study because COVID-19 resulted in many health challenges for patients with ADRD, as people with ADRD were found to be twice as likely to contract COVID-19 and have higher risks of hospitalization and mortality compared to people without dementia (Q. Wang et al., 2021). Additionally, COVID-19 periods of recommended and voluntary social isolation may have heightened the role and significance of hospital-HIT patient engagement between patient and hospital provider. The COVID-19 pandemic also exposed the challenges in the documentation and distribution of diagnosis results while also motivating the case for improving electronic health data exchanges (Greene et al., 2021). During the COVID-19 pandemic, health information exchange was used to combine sociodemographic, clinical, and lab results for patients with COVID-19, and found that COVID-19 fatalities are associated with patients who are older adults, males, and smokers (Tortolero et al., 2021).
There is limited research on HIT and health information exchange for ED patients with ADRD and to our knowledge, no research has examined differences in the odds of preventable ED visits by electronic health information exchange as related to COVID-19 (N. Wang et al., 2021). This study examines the odds of a preventable ED visit during the COVID-19 pandemic among the ADRD population, with a focus on hospital-based information exchange. We hypothesize that the availability of electronic information exchange can lead to lower odds of preventable ED visits. We base our hypothesis on recent literature showing that the successful implementation of health information exchange before and during COVID-19 improves health care delivery, care coordination, and health care outcomes (Sarkar, 2022). In addition, a recent cohort study of hospitalized patients with ADRD who had a readmission to a different hospital that shared a health information exchange had lower odds of mortality compared to hospitals without a shared health information exchange (Turbow et al., 2023).
Finally, we tested the association among patients with ADRD and MCC as these patients are more likely to experience cognitive decline (Bratzke et al., 2018). Our rationale was to examine whether health information exchange can lead to increases in the efficiency of providing and coordinating health care amid the COVID-19 pandemic. Our study aims to underscore the integration of HIE and the potential of utilizing health information exchange as strategic tools for preparing people with ADRD, and especially those with ADRD and MCC, for future public health emergencies.
Methods
Data
This study uses the 2020 State Emergency Department Databases (SEDD) from six states (Arizona, Florida, Kentucky, Maryland, North Carolina, and Wisconsin) as well as the 2020 Area Health Resources File (AHRF), American Hospital Association (AHA) Annual Survey, and the AHA Information Technology Supplement (AHAIT). The SEDD provides information such as diagnoses and patient characteristics for all the ED discharges for a given state and year, the AHRF provides county-level data, and the AHA Annual Survey and AHAIT provide data about hospital characteristics.
Our sample consists of patients aged 50+ with a diagnosis of ADRD and a routine discharge in the SEDD data. ADRD is diagnosed using ICD-10 codes and based on guidelines from the CMS Chronic Condition Warehouse (CCW) (Centers for Medicare & Medicaid Services, 2022).
Measures
The dependent variable is whether the ED visit is considered preventable based on the New York University (NYU) ED Algorithm (NYU, 2016). The NYU algorithm uses the primary ICD-10 diagnosis code of each ED visit and creates a measure stating the likelihood that an ED visit was potentially preventable or treatable in primary care settings, we used an updated patch of the algorithm for increased accuracy (Johnston et al., 2017). We create a binary variable using a threshold of ≥75% of the sum of the categories of Non-emergent, Emergent/Primary Care Treatable, and Emergent—ED Care Needed—Preventable/Avoidable and excluded ED visits with an unclassifiable preventable ED category based on prior literature (B. K. Chen et al., 2015; N. Wang & Chen, 2023). Our final sample consists of 85,261 discharges with a diagnosis of ADRD and complete information.
The key independent variables are measures of hospital health information exchange as related to treating COVID-19. The first key independent variable asks how frequently each type of clinical information that is necessary for treating patients with COVID-19 is electronically available from outside providers. There were seven information types available (diagnoses, problem lists, lab results, clinical notes, medications, images, immunization details). For each information type, we created a value of 1 for always/often and 0 for all others (sometimes, rarely, never, don’t know) and summed up the values for each hospital. We then created an indicator of high HIE-outside clinical information equals 1 if hospitals always/often received six or more types of clinical information from outside providers (i.e., above the 75th percentile of score 6 of the distribution of HIE-outside clinical information) and 0 otherwise.
The second key independent variable asks that when patients who were admitted to your hospital had been tested for COVID-19 outside of your health system, to what extent did the hospital receive results from each entity in an electronic format. There were six entities examined (large commercial labs, small/independent/regional labs, public health labs, other hospitals, traditional ambulatory providers, and emerging providers such as pharmacies and “pop up” testing). For each entity, we created a value of 1 for always/often and 0 for all others (sometimes, rarely, never, don’t know). Hence, we defined high HIE-COVID testing results equals 1 if hospitals received COVID-19 results from at least three outside entities (i.e., above the 75th percentile of score 3 of the distribution of HIE-COVID testing results) and 0 otherwise.
The Elixhauser comorbidities index examines the ICD-10 diagnoses codes for comorbidities that can influence a patient’s disease burden and predict the mortality rate and is based on the latest Elixhauser Comorbidity Software (v2023.1) (Healthcare Cost and Utilization Project (HCUP), 2022). Two or more co-present chronic conditions are defined as MCC (Lefèvre et al., 2014).
We selected covariates based on the ADRD literature and the Andersen Behavioral Model of Health Services Use (Andersen, 1995). Individual characteristics included sex, race and ethnicity, age, primary insurance, and discharge quarter. Hospital characteristics included bed size, urban and rural locations, ownership, and teaching hospital status. Geographic characteristics included the income quartile based on the median household income of residents from the patient’s ZIP code, the county percent African American (median of 11.60%), and county mental health care shortage area status.
Analysis
Figure 1 shows the availability of health information exchange for patients with ADRD and patients with ADRD and MCC separately. Sample characteristics based on the variables above are provided in Table 1. We compared the sample characteristics by high HIE-COVID measures (i.e., both HIE-outside clinical information and HIE-COVID testing results above the 75th percentile vs. not). In Table 2, logistic regressions were applied to examine the associations between having HIE-outside clinical information or HIE-COVID testing results with the odds of having preventable ED visits. We also present the results of interactions of each HIE measure with the presence of MCC among patients with ADRD in Table 3.

Preventable emergency department (ED) visit probability by electronic health information exchange (HIE) distribution for patients with Alzheimer’s disease and related dementias (ADRD). Note. Analysis of 2020 State Emergency Department Databases, American Hospital Association Annual Survey Information Technology Supplement, and Area Health Resources File (N = 85,261). HIE = Health information exchange; ADRD = Alzheimer’s Disease and Related Dementias; ED = Emergency Department. Clinical information for treating patients with COVID-19 measures how frequently each type of clinical information that is necessary for treating patients with COVID-19 is electronically available from outside providers. There were seven types available (diagnoses, problem lists, lab results, clinical notes, medications, images, immunization details). Above 75th percentile equals 1 if there are six or more types of clinical information from outside providers (i.e., above the 75th percentile of the distribution) and 0 otherwise. COVID-19 results from outside entities measures when patients who were admitted to your hospital had been tested for COVID-19 outside of your health system, to what extent did the hospital receive results from each entity in an electronic format. There were six entities examined (large commercial labs, small/independent/regional labs, public health labs, other hospitals, traditional ambulatory providers, and emerging providers such as pharmacies and “pop up” testing). Above 75th percentile equals 1 if three or more outside entities (i.e., above the 75th percentile of the distribution) and 0 otherwise.
Sample Characteristics of Patients with ADRD by Hospital HIE Characteristics.
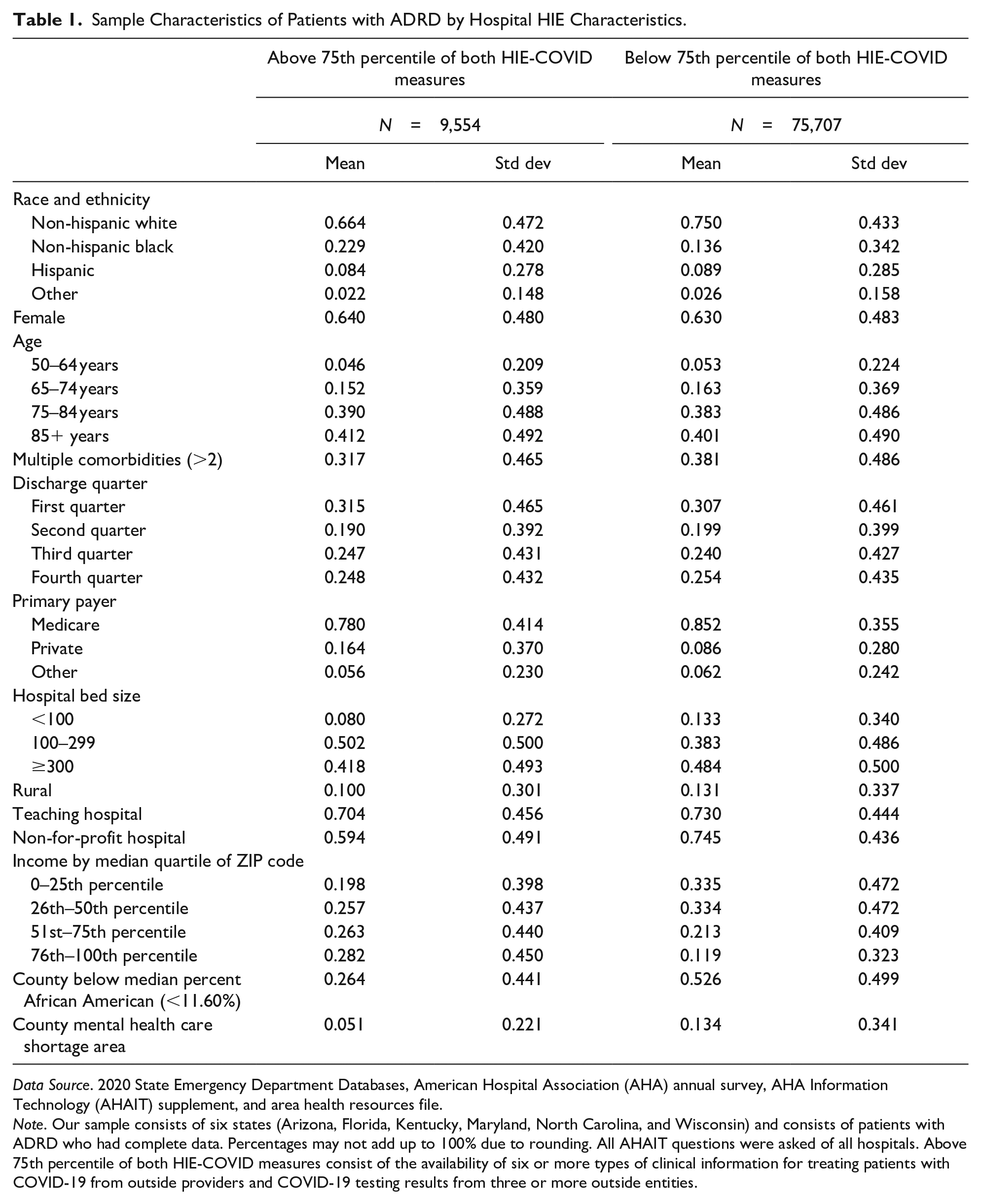
Data Source. 2020 State Emergency Department Databases, American Hospital Association (AHA) annual survey, AHA Information Technology (AHAIT) supplement, and area health resources file.
Note. Our sample consists of six states (Arizona, Florida, Kentucky, Maryland, North Carolina, and Wisconsin) and consists of patients with ADRD who had complete data. Percentages may not add up to 100% due to rounding. All AHAIT questions were asked of all hospitals. Above 75th percentile of both HIE-COVID measures consist of the availability of six or more types of clinical information for treating patients with COVID-19 from outside providers and COVID-19 testing results from three or more outside entities.
Logistic Regression for Preventable Emergency Department Visit for Patients with ADRD and Multiple Chronic Conditions.

Data Sources. 2020 State Emergency Department Databases, American Hospital Association Annual Survey and Information Technology Supplement, and Area Health Resources File.
Notes. N = 85,261. Clinical information for treating patients with COVID-19 = 1 if hospitals always/often received from 6 or more types of clinical information from outside providers (diagnoses, problem lists, lab results, clinical notes, medications, images, immunization details), that is, above the 75th percentile of the distribution.
COVID-19 results from outside entities = 1 if hospitals always/often received COVID-19 results from three or more outside entities (large commercial labs, small/independent/regional labs, public health labs, other hospitals, traditional ambulatory providers, and emerging providers such as pharmacies and “pop up” testing), that is, above the 75th percentile of the distribution. OR = odds ratio; CI = confidence interval.
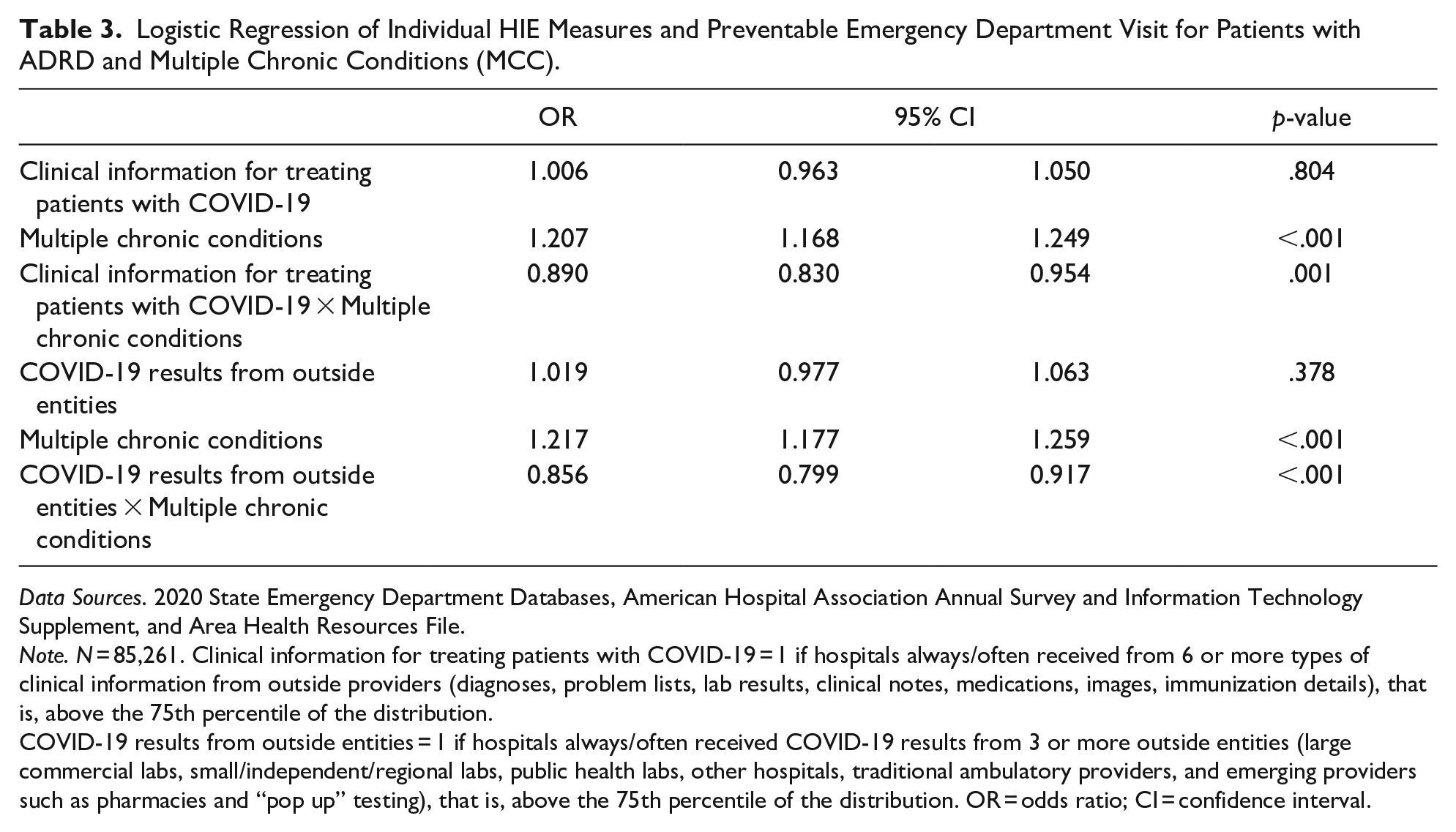
Logistic Regression of Individual HIE Measures and Preventable Emergency Department Visit for Patients with ADRD and Multiple Chronic Conditions (MCC).
Data Sources. 2020 State Emergency Department Databases, American Hospital Association Annual Survey and Information Technology Supplement, and Area Health Resources File.
Note. N = 85,261. Clinical information for treating patients with COVID-19 = 1 if hospitals always/often received from 6 or more types of clinical information from outside providers (diagnoses, problem lists, lab results, clinical notes, medications, images, immunization details), that is, above the 75th percentile of the distribution.
COVID-19 results from outside entities = 1 if hospitals always/often received COVID-19 results from 3 or more outside entities (large commercial labs, small/independent/regional labs, public health labs, other hospitals, traditional ambulatory providers, and emerging providers such as pharmacies and “pop up” testing), that is, above the 75th percentile of the distribution. OR = odds ratio; CI = confidence interval.
We tested different sensitivity analyses to check the robustness of the results. We applied the linear regression and considered HIE measures as continuous variables. We also tested the analyses among the population aged 65 and above only; the results were similar and available upon request. Our analysis was conducted in Stata 17 MP and was approved by the University of Maryland Institutional Review Board.
Results
Figure 1 shows the bivariate association of the patient’s preventable ED visit rate by HIE measures. The probability of preventable ED visits among patients with ADRD was lower for patients who went to hospitals that received more types of clinical information for treating patients with COVID-19 (33% vs. 34%) and received COVID-19 testing results from more outside entities (33% vs. 34%). The reduction in preventable ED visits was more pronounced among patients with ADRD and MCC as the results showed 3% points lower in preventable ED visits among patients with ADRD and MCC when they were admitted to hospitals with higher HIE scores (34% vs. 37%).
Table 1 shows the characteristics of our sample population. Patients with ADRD who are treated in hospitals with high scores in both HIE-COVID measures were more likely to be Black (23% vs. 14%), privately insured (16% vs. 9%), be located in urban (90% vs. 87%), living in a ZIP code with the top quartile of income (28% vs. 12%), living in a county with a below-median percent of African Americans (26% vs. 53%), and not in a county designated as a mental healthcare shortage area (5% vs. 13%).
Table 2 shows the results of our multivariable logistic regression. Patients with ADRD who were treated in hospitals that received more types of clinical information from outside providers for treating patients with COVID-19 were significantly less likely to encounter preventable EDs (OR = 0.961, p < .05). Similarly, patients with ADRD who were treated in hospitals that received COVID-19 results from more outside entities were significantly less likely to encounter preventable EDs (OR = 0.964, p < .05).
The results also showed that patients with ADRD and MCC were more likely to have a preventable ED. When compared to Non-Hispanic White patients, Non-Hispanic Black and Hispanic patients had higher odds of having preventable ED visits. Patients with ADRD and living in the lowest ZIP code income quartile had higher odds of having preventable ED visits compared to the highest ZIP code income quartile. Patients with ADRD and living in mental health care shortage areas were also more likely to encounter preventable EDs.
Table 3 presents the results of logistic regression controlling for interaction terms between HIE and the presence of MCC. Patients with ADRD and MCC were more likely to have a preventable ED, however, patients with ADRD and MCC who were admitted to hospitals adopting high levels of COVID-related HIE were significantly less likely to have preventable ED visits (OR = 0.89, p = .001; OR = 0.856, p < .001, respectively.)
Discussion
The results of this study suggest that hospital-based information exchange can help reduce the probability of having a preventable ED visit for patients with ADRD and patients with ADRD and MCC during COVID-19. Our findings are consistent with previous research that shows associations between beneficial health care outcomes from telehealth and health information technology-related features for patients with ADRD (N. Wang et al., 2022). Research has also shown a beneficial association between hospital Meaningful Use (MU) of electronic health records (EHRs) and process quality, suggesting a connection between technological investment and utilization, clinical information availability, and quality of care, which may be especially meaningful for patients with complex health needs such as those with ADRD (Y. K. Lin et al., 2019). For patients with ADRD, the added challenges surrounding memory and communication heighten the need for electronic information exchange, which can be used by hospital clinicians to obtain outside clinical information and coordinate with primary care physicians to create a care plan for health services outside of the ED setting.
Specifically, the results of the study showed that obtaining test results for COVID-19 from entities outside of the hospital was associated with lower odds of having a preventable ED visit for patients with ADRD. COVID-19 testing for patients with ADRD is crucial to creating appropriate care plans during the pandemic, as a recent study showed that a sample of 14 patients with pre-existing dementia who tested positive for COVID-19 had all experienced greater fatigue and depression, worsening memory and attention, and 10 of them required hospitalization after a one-year follow-up (Dubey et al., 2023). Testing for COVID-19 early in the pandemic was crucial for determining COVID-19 transmission rates and was performed in a variety of health care, community, and home settings (Rosenberg et al., 2020). The pandemic spotlighted the need for health information exchange capability between hospitals and a variety of partners, and greater standardization of health data and systems compatibility.
Our results also find racial and ethnic disparities in the odds of having a preventable ED visit during COVID-19. Previous research by the CDC shows that Black and Hispanic patients had 1.4 times the rate of emergency department visits for COVID-19 during October–December 2020 compared to White patients (Smith et al., 2021). A recent study shows that enhanced HIT infrastructures can improve patient engagement and care coordination and identify patients’ needs that can improve racial and ethnic health disparities among patients with ADRD (J. Chen et al., 2022). Another study on HIT quality found that the effect sizes of attaining MU of EHRs for process quality of care were larger in small and rural hospitals, which led authors to conclude that HIT may mitigate disparities in the quality of health care (Y. K. Lin et al., 2019). It is imperative that ADRD research continue to analyze both technology’s ability to reduce health care disparities and the effects of the digital divide.
There are some limitations to this study. First, this study is a cross-sectional analysis and does not infer causality about its results. Second, we acknowledge that we measured hospital-level HIE adoption and hence an intent to treat analysis. There is a lack of data on the actual use of the information being exchanged for each ED visit. Third, we used multiple indices of HIE measures to test the overall variation. Future research may focus on specific aspects of information exchange tailored to different patient characteristics, health needs, and social determinants of health. Fourth, there may be omitted variables such as disease severity and cultural preferences of data sharing and privacy that are not measured in the data. Finally, our sample consists of six states and may not be nationally representative.
Policy Implications
Alternative payment models (APMs) that reward quality and require collaboration financially incentivize greater health information exchange among providers and across the health care continuum. For example, earlier work showed ACO-affiliated hospitals had 0.91 lower adjusted odds of preventable ED visits for patients with ADRD compared with hospitals not affiliated with an ACO (N. Wang et al., 2021). Another study found APMs were associated with greater hospital health information exchange diversity, breadth, and depth than volume-based contracts, leading researchers to conclude that value-based payment models may be an effective driver of hospital health information exchange infrastructure, and able to overcome the competitive forces beneath information blocking (S. C. Lin et al., 2019). While our study does not differentiate payment model type within payer entities, the finding that health information exchange of COVID-19 diagnosis results is associated with a reduction in preventable ED visit rate underscores the importance of health information exchange in reducing preventable ED visits for patients with ADRD and indicates that policymakers should continue to advocate for and incentivize payment structures that attract collaboration and health information exchange. We believe future research that analyzes contract type, health information exchange, and preventable ED visits for ADRD care is important.
Conclusion
The COVID-19 pandemic prompted efficiency in health care decision-making, and electronic information exchange can make the health care delivery and planning process more efficient. The results of our study show that the availability of electronic health information exchange from multiple health care entities is associated with lower odds of having a preventable ED visit. Hospitals can promote information exchange by coordinating efforts with local outside entities and ensuring that information can be easily exchanged and processed when needed. Further research can examine other potential benefits of hospital-based information exchange, such as its use in care coordination outside of hospital settings, public health reporting, and planning for future pandemics and disasters.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Institutes of Health, National Institute on Aging Grant [R01AG062315 and RF1AG083175].
Ethical Approval
This study was approved by the University of Maryland IRB (institutional review board) as a secondary data analysis of deidentified patients with minimal risk, as such patients were waived from informed consent by the University of Maryland IRB.