
Abstract
Background
People living with Alzheimer's disease and other types of dementia are vulnerable to medicine-related problems. More research is needed to support achieving quality use of medicines in people living with dementia.
Objective
To determine the top 10 unanswered quality use of medicines questions for people living with dementia, as prioritized by Australians living with dementia, their carers, and healthcare professionals.
Methods
The James Lind Alliance Priority Setting Partnership method was used. This manuscript reports the second half of the priority setting process. Using a quantitative survey, consumers (people living with dementia, their carers and family and friends) and healthcare professionals selected up to ten research questions about quality use of medicines that they felt were most important. The research questions were informed by a previous national qualitative survey and evidence checking process to identify those that were unanswered. An online workshop was then conducted with consumers and healthcare professionals to prioritize the unanswered questions, resulting in a top 10 list.
Results
171 consumers and 67 healthcare professionals completed the survey and the workshop included 17 participants. The top 10 priorities related to shared decision making, education of healthcare professionals, communication between healthcare professionals, reducing the use of unnecessary and harmful medicines, managing medicines safely at home, medicine reviews, residential aged care facilities and managing pain, behavioral changes, depression and anxiety.
Conclusions
Targeting research efforts towards these identified consumer and healthcare professional priorities will ensure research funds are being directed to the most urgent areas of need in practice.
Keywords
Introduction
Medicines are the most common intervention used in healthcare, especially in people living with Alzheimer's disease and other types of dementia. 1 Approximately 50 million people were living with dementia worldwide in 2015, and by 2030, this is predicted to rise to 75 million. 2 It has been estimated that there are 400,000 people currently living with dementia in Australia. Similar to international figures, this number is expected to more than double by 2058. 3 Most people living with dementia have additional medical conditions, such as cardiovascular disease, depression, and diabetes leading to polypharmacy (use of multiple medicines).4,5 Therefore, it is essential to ensure that medicines used to manage dementia and other medical conditions are used appropriately and in line with the individual's goals and preferences.6,7
Quality use of medicines means ensuring medicines are used safely, effectively, and judiciously to achieve optimal health outcomes. The importance of quality use of medicines has been recognized in Australia and internationally.8–10 However, quality use of medicines is complex to achieve for people living with dementia. Reasons for this include heterogeneity, multimorbidity, polypharmacy, non-adherence, involvement of multiple healthcare providers, and fragmented care. Furthermore, changes in cognition, executive functioning and behavior can further increase the risks of medicine use and necessitate the involvement of carers (who may have different perspectives and priorities). This also leads to challenges in establishing goals of care (and changing goals of care) and difficulties recognizing and reporting adverse drug reactions.11–14 Additionally, people living with dementia are often excluded from clinical trials, compounded by language limitations and recruitment processes to achieve required sample sizes. These issues limit evidence to inform the likely benefits and harms of medicine use in this population.15–17 Consequently, there are many unanswered questions regarding quality use of medicines in people living with dementia.14,18 Australia, like many other high-income countries has an ageing population with increasing prevalence of dementia, polypharmacy and multimorbidity and associated medicine related harm. Several recent national initiatives such as the Royal Commission into Aged Care Quality and Safety and naming dementia and quality use of medicines and medicine safety as the 9th and 10th (most recent) national priority areas highlight the need for focused research on quality use of medicines in people living with dementia in Australia.10,19
Historically, research priorities were often informed by commercial entities, researchers and government and other research grant funding agencies.20,21 More recently, however, government, funding bodies and consumer advocacy groups internationally have highlighted the need for genuine consumer and healthcare professional engagement to inform research priorities and associated research questions.22–24 Stakeholder engagement has great potential to improve research adoption in practice by ensuring research meets people's preferences and needs. 25 Recognizing and prioritizing the needs of those most affected by medical conditions is imperative to informing how to optimize treatment and care.
The overall aim of this project was to identify the top 10 unanswered quality use of medicines questions for people living with dementia, as generated and prioritized by Australians living with dementia, their carers, and healthcare professionals (clinicians). The target audience of these priorities includes policy makers, funders, researchers, healthcare professionals, consumers and the general public. This was a multi-step project, as outlined in Figure 1. The first three steps of this project have been published including the creation of a priority setting partnership, gathering of evidence uncertainties from people living with dementia, their carers, family/friends and healthcare professionals via a survey, and evidence checking to ensure that the questions had not previously been answered by research. 26 The findings of the evidence checking process including relevant references are provided in the Supplemental Material of this previous manuscript. These research steps resulted in compilation of a list of 67 unanswered questions that are potential priorities for research in the field of quality use of medicines in people living with dementia. They encompass questions about the benefits and harms of medicines as well as how to achieve high quality use of medicines in people living with dementia. 26
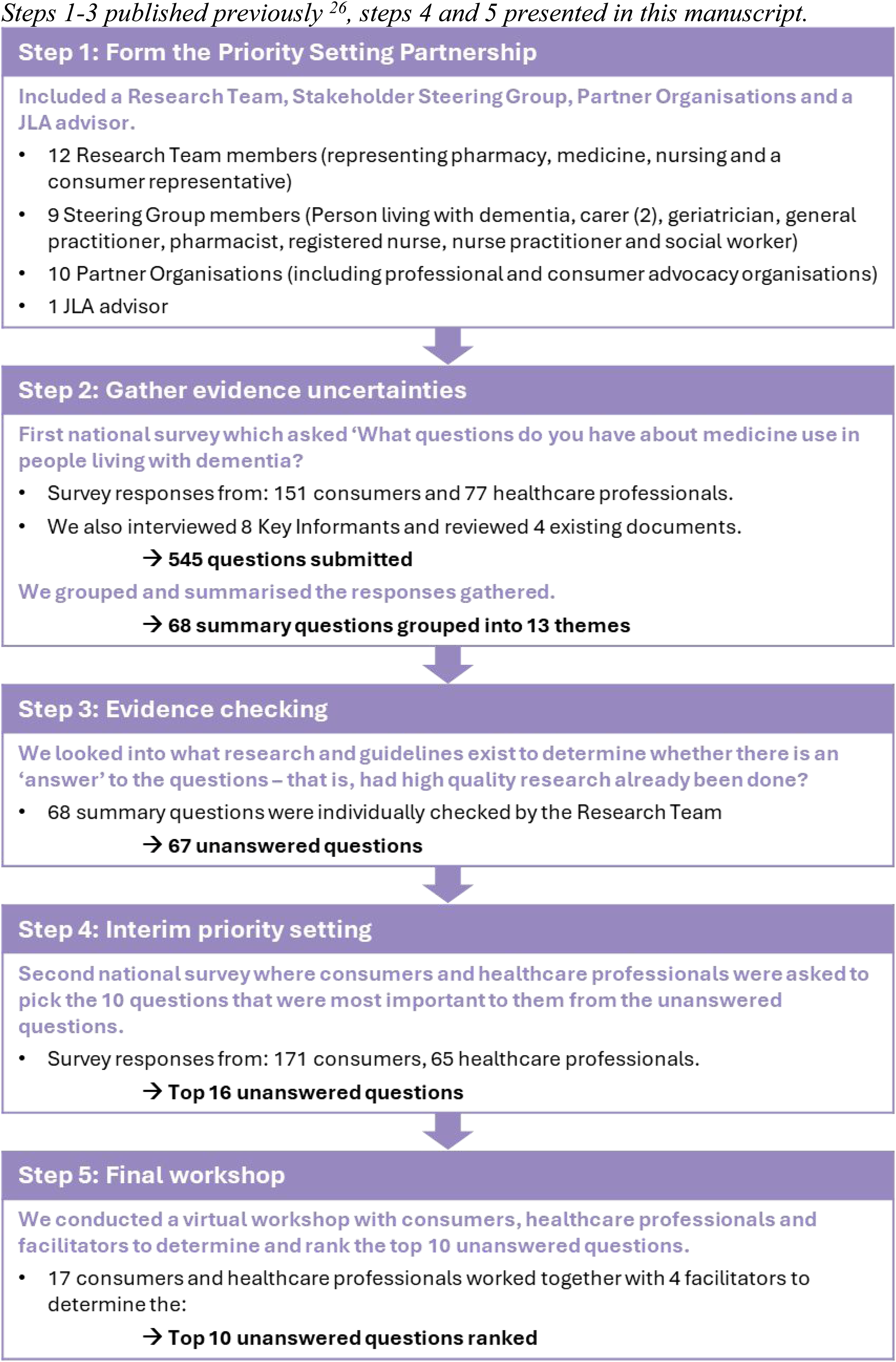
Overview of the multi-step process to establish the top 10 unanswered quality use of medicines questions for people living with dementia. Steps 1–3 published previously, 26 steps 4 and 5 presented in this manuscript.
While all these unanswered research questions have merit, pragmatic considerations such as funding and time limitations, necessitate prioritization of those that are most important to answer. This manuscript reports on the steps undertaken to prioritize these 67 unanswered research questions to establish a top 10, according to consumers and healthcare professionals (steps 4–5, Figure 1).
Methods
This project was conducted using the James Lind Alliance (JLA) Priority Setting Partnership method. This method supports consumers and healthcare professionals to collaborate, as partners, to determine priority research areas. The Priority Setting Partnership was composed of a Stakeholder Steering Group, Partner Organisations and Research Team, supported by a JLA advisor (full details have been previously published 26 ). This study was reviewed and approved by the University of South Australia Human Research Ethics Committee (#202847). The reporting guideline for health research priority setting with stakeholders (REPRISE) checklist is shown in Supplemental Material 1.
We operationalized research priorities related to quality use of medicines to include any questions that would support safe and effective use of medicines to get the best possible health and wellbeing outcomes. It included all medicines that a person living with dementia could take (i.e., not limited to dementia medicines), and all prescription, over the counter, herbal and complementary medicines. We encouraged questions about the possible benefits and harms of specific medicines (or combinations of medicines), and what healthcare professionals could do to make sure that medicines are being used safely and effectively. Questions about the development or discovery of new medicines were excluded. We focused the work on the care of people living with dementia, but without limiting to specific types of dementia.
Interim priority setting (step 4, Figure 1)
Initial question reduction
Sixty-eight summary questions across 13 themes were identified through a survey designed to gather evidence uncertainties from people living with dementia, carers, family/friends and healthcare professionals (step 2, Figure 1). Then the evidence was checked to ensure that the questions had not previously been answered by research, resulting in 67 unanswered research questions (step 3, Figure 1, details described in 26 ). The Steering Group considered that 67 questions were too many to be included in the interim priority setting survey (i.e., too high cognitive load for people living with dementia, and would take too long), and that about 50 questions would be an acceptable number for consumers and healthcare professionals to consider. Two steps were undertaken to reduce the number of questions from 67 to 50. Firstly, the top 25 unanswered research questions that had been informed by the greatest number of respondents to the evidence uncertainty survey (step 2, Figure 1) were retained. The remaining 42 questions were then reviewed by the Steering Group with each member asked to select their unranked top 10. All the questions that received one or more votes from Steering Group members were included in the interim priority setting survey. In addition to the 25 unanswered research questions that were contributed to by the greatest number of respondents in the step 2 survey, 29 additional questions were included based on the Steering Group vote (see Supplemental Material 6). This led to a total of 54 unanswered research questions to be included in the interim priority setting survey.
Interim priority setting survey
The interim priority setting of unanswered research questions was conducted using an anonymous cross-sectional survey that consisted of two sections (Supplemental Material 3 and 4). In the first section, the 54 unanswered questions were presented, and respondents were asked to select up to ten questions that they felt were most important (unranked). The 54 questions were grouped in their themes to make review and selection of the top 10 questions easier. We created four versions of the survey through randomization of the order of the themes and order of the questions within the themes to reduce bias. These different surveys were randomly presented to respondents who provided responses online. The online survey was administered via Research Electronic Data Capture (REDCap) (Vanderbilt University, Nashville, TN) tool hosted at the University of South Australia.27,28 The option of a paper version was made available for respondents, although none were requested. The second section of the survey collected respondent characteristics (see Table 1).
Interim priority setting survey respondent characteristics (n = 171/65; consumers/healthcare professionals).

Demographic questions were optional to maximize responses to the first part of the survey. Numbers are shown as consumer/healthcare professional.
May add up to greater than 100% as respondents were able to select more than one option.
Those who were previous friends, family, or carers of a person living with dementia who is now deceased were included in these figures.
For example, respondents reported being an interested party, a dementia advocate, a care companion, living with cognitive impairment but without a dementia diagnosis, or didn’t specify further.
These respondents included a psychiatrist, and a general medicine advance trainee.
Allied Health professionals included psychologists, occupational therapists, optometrists, and speech pathologists
These respondents included one unspecified, a dentist, an unspecified healthcare professional, a health care ethicist, an Aged Care Assessment Team (ACAT) assessor, an activities coordinator for aged care residents, and a community care team leader.
Survey dissemination
The survey was disseminated through multiple mechanisms (convenience sampling), using the same procedures as the first survey (step 2, Figure 1, previously reported 26 ). This included 1) We sent the advertisement (which included the link to the REDCap survey) to partner organizations and other relevant professional and advocacy organizations, who then disseminated it to their members. Examples of this promotion included social media posts, newsletters and promotion at events (e.g., seminars and conferences); 2) A research engagement service called StepUp for Dementia Research Australia (https://www.stepupfordementiaresearch.org.au/) was used to advertise the consumer survey (Supplemental Material 3); 3) Respondents who completed the survey were invited to share with their networks (snowballing); 4) Respondents of the first survey who consented to be contacted for future steps of the research were directly sent the advertisement; 5) The research team and Steering Group members disseminated the advertisement via their personal networks. The survey was open from July to September 2021.
Participants
The study involved consumers and healthcare professionals. Consumers included people living with dementia, carers (informal and/or unpaid carers of people living with dementia such as family members or friends), friends and family who do not identify as carers, and other members of the public with a direct interest in medicine use in people living with dementia (such as previous carers or advocates). Healthcare professionals (including students and trainees) were required to have experience providing care for people living with dementia. Participation was not limited to any particular profession(s). All participants were at least 18 years old, able to read and write in English, and Australian citizens or currently living and/or working in Australia. This work was limited to Australia to identify questions most important for the Australian context. Consent was implied through completion and submission of the survey. No remuneration for participation in the survey was provided.
Analysis
Participant characteristics were analyzed descriptively. The total number of votes for each question was determined separately for consumers and healthcare professionals to ensure equal weighting of the two groups. The number of votes for each question was then converted to a ranking (i.e., the question with the greatest number of votes was ranked #1, the question with the next highest number of votes was ranked #2, etc.). If a participant had selected more than 10, but less than 20 questions, then a total of 10 points was distributed evenly among the questions (e.g., if they had selected 20 questions, each question would receive 0.5 votes). If they selected more than 20 questions, all their votes were excluded from analysis as per JLA methods to avoid giving unfair weighting to the priorities of these individuals. To determine the combined rank, the consumer and healthcare professional ranks were summed and a new ranking was identified based on the summed ranks. We also looked at the top three ranked questions in participant subgroups who were identified by the Steering Group to be important, but who were underrepresented in the survey responses (e.g., General Practitioners, people taking >10 regular medicines). The combined and subgroup findings were then reviewed by the Steering Group to decide on approximately 15 questions to include in the final prioritization workshop. All analysis was conducted in Microsoft Excel. (See Supplemental Material 5: Survey methods checklist for further details of survey methods.)
Final priority setting workshop (step 5, Figure 1)
The final prioritization of the unanswered research questions was conducted via a workshop with consumers and healthcare professionals to allow for sharing of knowledge and experiences, and to facilitate a group decision. We aimed to have 20 participants for the workshop (which could be split into four groups of five participants for discussions). We aimed to recruit 10 consumer participants (equally split between people living with dementia and carers) and 10 healthcare professionals. Healthcare professionals were recruited purposively to include one or more of the following: geriatrician, GP, nurse, aged care worker, pharmacist, and social worker. We also aimed to have a diverse, gender-balanced group with participants from across Australia. Consumer participants were recruited through the advocacy network of Dementia Australia, and healthcare participants were recruited through partner organizations and networks of the research team and Steering Group. Additionally, we invited respondents from the first two surveys (who consented to future contact) to achieve the aimed for diversity. Consumer participants could participate as individuals, people living with dementia could participate with a carer present for support, or dyads (person living with dementia and their carer) could both be participants. Participants needed to be able to read and speak English and provide written informed consent. Written informed consent was obtained from all participants prior to the workshop. Participants were offered a $100 gift card as honorarium in recognition of their time.
The workshop was held via Zoom over two separate days (held two days apart), with each session less than 2.5 h long (with breaks) to maximize participation across Australia, reduce risk of COVID-19 infection and minimize videoconferencing fatigue. Participants were asked to watch two short videos prior to the workshop; one about the structure of the workshop, and another on the topic of quality use of medicines and the findings of the study to date. We sent participants the questions shortlisted through the interim priority setting exercise and the workshop agenda via email and in hard copy via the post. We also met individually with consumer participants who requested further information and/or support to use the teleconference platform prior to the workshop. Four professional facilitators with expertise in the JLA method were hired to facilitate the workshop groups. We also had an individual available to attend to technology difficulties, and a support person (registered nurse experienced in caring for people living with dementia and their care partners) on call if any participants felt uncomfortable, disorientated, or sought counselling or direction about their concerns.
On the day, the workshop participants were broken into four groups (using Zoom breakout rooms) of four to five participants. Small groups were formed to ensure a variety of participants, for example, one person living with dementia, one carer, and two healthcare professionals, plus one facilitator. The workshop was divided into phases as follows:
Day 1:
Phase 1: In small groups each participant was given the opportunity to say which questions they felt were most important for research to answer and why, and which questions they felt were less important and why. Phase 2: Each group worked together to put all the questions in order of priority. This was facilitated by a virtual pinboard whereby the facilitator moved abbreviated versions of the questions around the virtual screen.
After conclusion of Day 1 the results of all four small groups were combined to create an aggregate shared ranked order.
Day 2:
Phase 3: The whole group came together and were presented with the aggregate shared rank order from Day 1. Phase 4: During a second round of small group discussion, with a new mix of participants in the small groups, participants worked together to review and revise the aggregate shared ranking of the questions as presented in Phase 3. All questions were open to discussion, but the groups were advised to focus on the high to medium ranked questions, as the process moved them towards the stage of agreeing a final top 10. Phase 5: A new aggregate shared rank was created based on the re-rankings in each of the four groups in Phase 4 to create the final ranking of the questions. The whole group then had the opportunity to discuss and share reflections on the final ranking of the questions.
Results
Interim priority setting
Survey respondent characteristics
A total of 238 respondents completed the survey. However, two healthcare professionals selected more than 20 questions and so were excluded from analysis leaving 171 consumers and 65 healthcare professional respondents. The majority of consumer respondents identified as a friend or family member of a person living with dementia (42.7%), or a carer (40.9%) (Table 1). Approximately 80% of consumer respondents identified as female. The most common healthcare professionals to respond were pharmacists (30.8%) and nurses (20.0%), and the majority of all healthcare respondents were women (78.5%). Healthcare professionals predominantly worked in a hospital (37.5%), primary care (28.6%), or residential aged care facility (39.3%), and over half (56.8%) had greater than 15 years of professional experience.
Survey results
The consumer and healthcare professional number of votes, question ranking and combined rank are shown in Table 2 for the top 20 questions (the full 54 questions are shown in Supplemental Material 7). Questions within the top 10 combined rank were all ranked within the top 14 by consumers and healthcare professionals. Additionally, the top 10 from each group were all in the top 16 combined rank. The combined top ranked question related to medicine use in treating changed behaviors; 34.3% of consumers and 43.5% of healthcare professional respondents selected this question in their top 10.
Results of interim priority setting survey, top 20 questions.
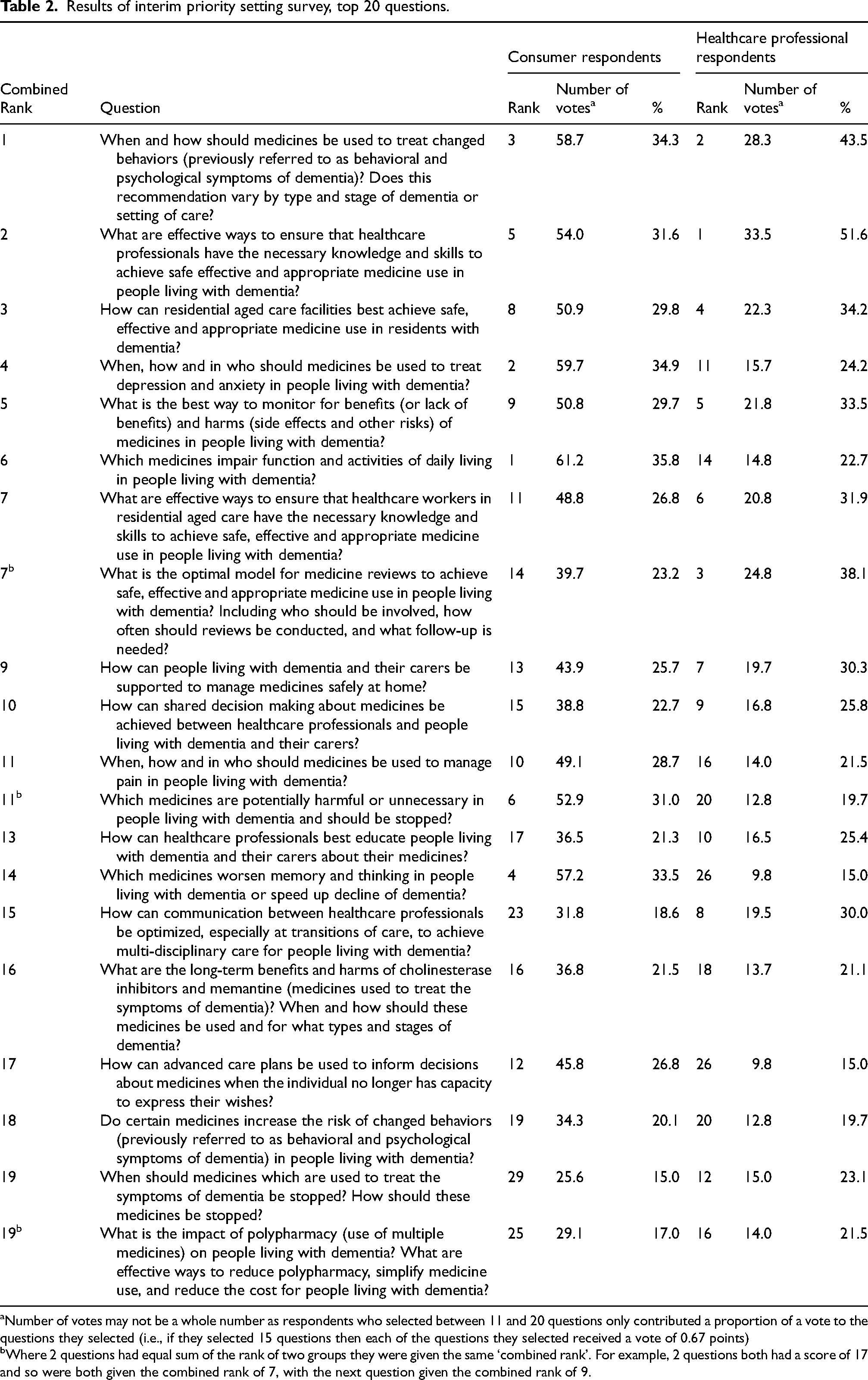
Number of votes may not be a whole number as respondents who selected between 11 and 20 questions only contributed a proportion of a vote to the questions they selected (i.e., if they selected 15 questions then each of the questions they selected received a vote of 0.67 points)
Where 2 questions had equal sum of the rank of two groups they were given the same ‘combined rank’. For example, 2 questions both had a score of 17 and so were both given the combined rank of 7, with the next question given the combined rank of 9.
Selection of questions for the final priority setting workshop
The results of the survey were presented to the Steering Group to review and select which questions would be included in the final priority setting workshop. Sixteen questions were selected to go through to the workshop (Supplemental Material 8). These were the Top 15 questions from the survey, plus the question that was ranked at number 17 due to it being highly ranked by a number of the important subgroups such as people living with dementia and people who identify as Aboriginal or Torres Strait Islander. Additionally, two questions that were outside the top 15 that were highly ranked by several of the important under-represented subgroups were combined with questions in the top 15 (i.e., two of the top 15 questions were edited to add additional, but closely related concepts). The two concepts were related to changed behaviors and polypharmacy.
Final priority setting
Eighteen participants consented to participate in the workshop; although, one participant was unable to attend. The remaining 17 participants included eight consumers (4 people living with dementia and 4 carers, none were dyads) and nine healthcare professionals (2 geriatricians, 1 General Practitioner, 3 pharmacists, 1 registered nurse, 1 assistant in nursing and 1 social worker). Thirteen participants (76.4%) were female, and participants were from across Australia including South Australia (6), New South Wales (4), Queensland (3), Victoria (1), Tasmania (1) and Australian territories (2).
The small group rankings and intermediate combined ranking are shown in Supplemental Material 9. At the end of the workshop all participants agreed with the final ranking and the Top 10. The final rankings for the top 16 unanswered research questions are shown in Table 3, presented with the theme developed after the first survey to identify the evidence uncertainties. 26
Priority setting workshop final ranking.
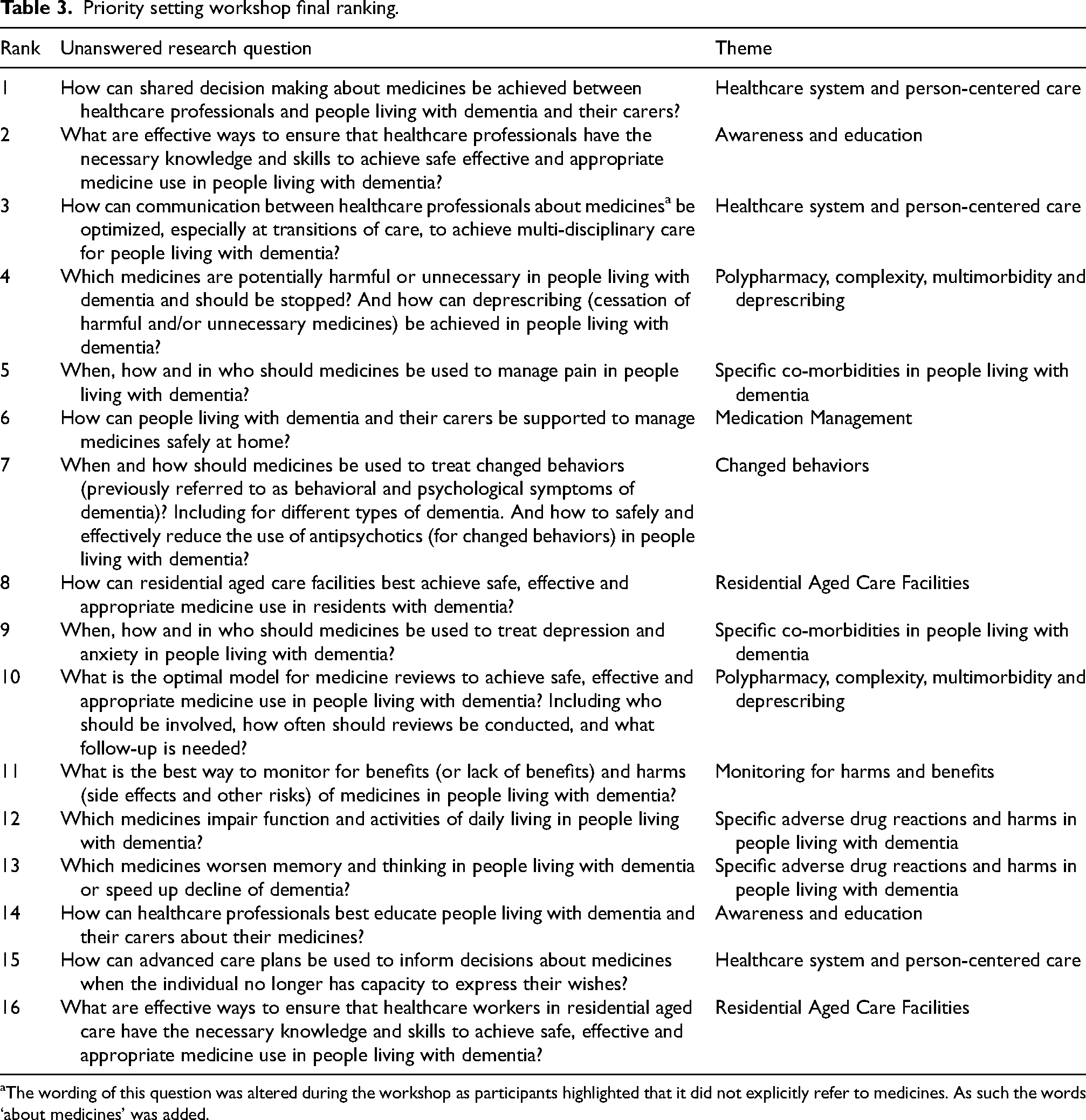
The wording of this question was altered during the workshop as participants highlighted that it did not explicitly refer to medicines. As such the words ‘about medicines’ was added.
Discussion
Summary of the findings
We were able to complete the multi-step Priority Setting Partnership process to establish a set of Top 10 priority research questions in quality use of medicines for people living with dementia. This is the first time that this process was conducted in Australia for any topic area, and the first time that this process was conducted internationally focusing on the topic of quality use of medicines. The top 10 questions include topics across the entire scope of quality use of medicines including treatment of symptoms of dementia (e.g., changed behaviors), treatment of common co-morbidities (pain, depression, anxiety), polypharmacy, optimizing shared decision making, education of healthcare professionals and how the healthcare system could better support people living with dementia. The questions are applicable across different practice settings, with only two being specific to one setting (i.e., #6 for people living at home, and #8 for people living in residential aged care) and another highlighting the importance of transitions between care settings (#3). To support dissemination of these priority research questions, we conducted a webinar and developed a brochure and brief pamphlet outlining the process and the Top 10 questions (Supplemental Material 10).
These priorities do not necessarily need to be researched in isolation as many of them are interconnected. For example, optimal treatment of changed behaviors (priority #7), pain (#5), depression and anxiety (#9) and reduction of harmful and unnecessary medicines (#4) may be supported through optimizing shared decision making (#1), educating healthcare professionals (#2), improving system level support in aged care facilities (#8) and having an optimal model for medicine reviews (#10). Indeed, a recent overview of reviews found that staff education and training along with appropriate organizational climate and collaboration may be an effective strategy to reduce inappropriate use of antipsychotics in aged care residents living with dementia. 29 The research questions may be answerable with a combination of basic science, clinical, health services and public health research. It is also important to note that while the overall research question was considered ‘unanswered’, this does not mean that there is no research on these topics. New research directed to these priorities should build on existing knowledge, and sustainability and cost-effectiveness also needs to be considered.
Comparison with other studies
A recent systematic review of international dementia research priority setting exercises identified 10 studies, although only two included people living with dementia, carers and healthcare professionals. Fourteen per cent of all priorities identified in this review were related to drugs and interventions. 30 While no other JLA Priority Setting Partnerships internationally have focused on quality use of medicines for people living with dementia, two (conducted in the UK and Canada) have previously focused on dementia.31,32 Additionally, in 2016 the World Health Organization conducted a Research Prioritization exercise with experts and stakeholders with the focus of reducing the global burden of dementia. 6 Similar to our findings, all these three studies found that research into the management of behavioral symptoms and how the healthcare system can better support people living with dementia should be a priority.6,31,32 Education of healthcare providers was also identified as a priority in Canada and by the WHO.6,31 Additionally, priorities related to communication between healthcare professionals, managing people safely at home, deprescribing, education of healthcare professionals and managing pain have been identified in Priority Setting Partnerships related to multiple conditions in later life, frailty, patient safety and safe care for adults with complex health needs.33–36 While this study was conducted from the Australian perspective, it is likely that the priorities are relevant to similar high-income countries internationally, especially as we consulted the international literature when determining if the questions were ‘unanswered’. 26
Many of our identified priorities align with Australian and international literature on areas for improving medicine use in people living with dementia. It has been established that people living with dementia are able to participate in shared decision making, and they along with carers and healthcare professionals want to use shared decision making. While there is growing research into shared decision making in this population, it is currently mostly limited to a few areas such as health promotion and advanced care planning.37,38 Additionally, a recent scoping review identified that there were limited resources to support carers in medication management (i.e., to support safe medicine use at home); and those that existed had minimal consideration of shared decision making. 39 Studies continually show a high prevalence of use of antipsychotics29,40–42 and other potentially harmful or unnecessary medicines (referred to as potentially inappropriate medications) in people living with dementia.42–46 Additionally, use of these medicines is associated with increased risks of harms including hospitalization and mortality in this population.43,47–49
In the interim priority setting survey, while there were slight differences in consumer and healthcare professional rankings, there was similarity among those ranked highest and lowest, and the majority of the questions received similar levels of support (see Supplemental Material 7). A previous study focused on anesthesia and peri-operative care found that consumers ranked questions about improving patient experience more highly, while healthcare professionals prioritized questions related to clinical effectiveness. 50 Other studies have also found stark differences between consumer and healthcare professional research priorities.51,52 We did not identify this same trend; this may reflect that healthcare professionals in dementia care are more aware of the experience, needs and perspective of people living with dementia and their carers than in other fields. However, there were some notable questions that received very different amounts of support from consumers and healthcare professionals. For example, in the interim priority setting survey consumers selected the questions about complementary medicines, drug-drug interactions and medical cannabis more often than healthcare professionals. It is expected that consumers and healthcare professionals will have different perspectives, and these findings validate the need for both consumers and healthcare professionals to be involved in research priority setting as per the JLA method.
Strengths and limitations
A strength of this study is the use of the established JLA method which has been used in over 180 studies internationally.53–56 Using this process resulted in engaging with almost 500 consumers and healthcare professionals across Australia over the 5 steps (as reported in this and our previous manuscript 26 ). The final workshop combined qualitative approaches which allowed sharing of experiences and discussion with a final quantitative step of determining the top 10 priorities. Another strength is that our process was driven by a Stakeholder Steering Group. The Group ensured that the process was suitable for the participants (such as recommending the final workshop be held over 2 days, 1 day apart to avoid overtiring participants), and were responsible for several key decisions, such as determining the scope of the project and deciding which questions to take into the final workshop (informed by the survey results). We also used professional facilitators for the workshop to prevent research team members influencing the results of the Top 10 based on their research interests, and to ensure that all participants had an equal opportunity to contribute. Our sample size is consistent with other JLA processes with similar sized scope conducted in Canada and the UK (which have larger total populations).33,36,57–59 Examining the changes in ranking between the interim priority setting survey and the final workshop show the benefit of this final step, which allows for re-prioritization of questions through information sharing, critical discussion and empowerment. 53 Interestingly, the question about the risks and treatment of COVID-19 in people living with dementia was ranked quite low (50 out of 54) in the interim priority setting survey despite data collection happening during the pandemic (2021). This indicates that participants focused on long term issues and how research could support quality dementia care in the future, rather than being strongly influenced by current events. This makes our findings still applicable to current research agendas (considering the final workshop was conducted in 2021), with participants identifying long term priorities (we do not currently have any plans to revise and update these priorities). Since this study was conducted new drugs for the treatment of Alzheimer's Disease have been developed, specifically monoclonal antibodies targeting amyloid-beta protein (e.g., donamemab and lecanemab). While they have been approved in some countries such as the USA and China, they are not currently approved for use in Australia, 60 therefore available treatments for dementia have not significantly changed since completing this study.
Our study does have several limitations. The majority of participants were female, however, this reflects several of our major participant groups, namely, carers, pharmacists and nurses who are predominantly female.61,62 We weighted survey responses from consumers and clinicians equally, as per the JLA method and because balanced representation between consumers and clinicians has been advocated for to fully cover the needs in practice. 30 But, considering the greater number of consumer survey participants, this could be seen as individual consumer responses having less influence in the final survey ranking than healthcare professionals. This is important in the context that people living with dementia made up less than 10% of our survey consumer participants. This and some other populations were under-represented in the survey respondents (e.g., Aboriginal and Torres Strait Islander people). To overcome this, we examined the results from these underrepresented groups to ensure that no important questions were missed. Additionally, in the final workshop we purposely recruited to ensure we had balanced representation of key participants with people living with dementia making up approximately one quarter of workshop attendees. Due to restrictions during the pandemic, the interim survey and workshop were completed online. This likely restricted participation from some important groups, such as people living with severe dementia. The final workshop only had 17 participants; thus, it was not possible for this group of people to be representative of the full spectrum of diversity in Australia. As the workshop contained both consumers and healthcare professionals, there was potential for a power imbalance which might have meant that consumers were less likely to speak up and share their opinion. However, use of professional facilitators ensured that all voices were heard equally and anecdotally all participants were very active in conversation and respectful of others’ views. We also conducted the entire study in English; therefore, the findings of this study may not represent the priorities of people who predominantly speak languages other than English.
It is also important to note that the decision to have a top 10 is an arbitrary cut off. All questions in the top 16, as well as those that did not make it to the final workshop are still important questions that may warrant further research. We did not formally evaluate the process of prioritization; however, an informal survey was conducted with workshop participants by the JLA, with generally positive feedback. Outside of dissemination activities, we do not have a formal plan for ongoing implementation or evaluation of impact, however, all individuals involved in this work continue to advocate for adoption of these priorities.
Implications
There are likely benefits to directing future research towards these consumer and healthcare professional priorities. Research that aligns with the needs of the community is more likely to be usable and therefore adopted. In turn, this has societal benefits through more appropriate resource allocation, i.e., efficient use of research funding.63–66 For researchers, directing research proposals to consumer and healthcare professional priorities can increase the likelihood of successfully obtaining funding. 63 Ongoing consumer and healthcare professional engagement in research to address these priorities is also important and can have additional benefits such as increased participant recruitment and retainment, more relevant research outcomes, improved credibility of research and findings, and greater dissemination of findings. 63 Previous priority setting exercises have led to dedicated funding opportunities and research programs directed towards the identified priorities.67–69 Members of our research team have started directing research towards the Top 10 priorities through successfully funded grants and PhD student studies. However, to achieve significant impact, the priorities need to be adopted by the research community (e.g., funders, researchers, stakeholder organizations) and those responsible for implementation of the research (e.g., health service providers, aged care providers, government) outside of those directly involved in the project.67–69
While there is an increasing push from funders and recognition from researchers about the need for consumer, healthcare professional and other stakeholder engagement in research, there is a comparative dearth of guidance on how to best do this, particularly when working with vulnerable populations such as people living with dementia.65,70 We used the JLA method to guide our engagement. This method aligns with the philosophy of Participatory Research,71,72 where the end-users or beneficiaries of the research are involved and contribute to the process not just as participants. Even those who were participants in our study (e.g., those responding to the surveys and being involved in the workshop) can potentially also be viewed as contributing to future research through their contribution to establishing and prioritizing the research questions.
While this work was focused on informing research, it also has implications for clinical practice because it identifies aspects of care that clinicians and consumers believe need research-informed improvement. For example, it shows that consumers and healthcare professionals value shared-decision making and want to reduce the use of potentially harmful medicines in people living with dementia. While the priorities are ‘unanswered’ in the sense that more research is needed, this should not stop healthcare professionals starting discussions and applying best principles to support these activities in practice.37,73
Conclusion
Using the James Lind Alliance Priority Setting Partnership method we established the Top 10 consumer and healthcare professional priorities for research into quality use of medicines in people living with dementia in Australia. The priorities related to shared decision making, education of healthcare professionals, communication between healthcare professionals, reducing the use of unnecessary and harmful medicines, managing medicines safely at home, medicine reviews, residential aged care facilities and managing pain, behavioural changes, depression and anxiety. These Top 10 research questions can be used to guide future research in the field of quality use of medicines in people living with dementia.
Supplemental Material
sj-docx-1-alz-10.1177_13872877251359984 - Supplemental material for Top 10 consumer and healthcare professional priorities for research in the field of quality use of medicines in people living with dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877251359984 for Top 10 consumer and healthcare professional priorities for research in the field of quality use of medicines in people living with dementia by Emily Reeve, Katherine Cowan, Lisa Kalisch Ellett, Ron Sinclair, Ann Pietsch, Timothy Pietsch, Lenore de la Perrelle, Judy Deime, Josephine To, Stephanie Daly, Craig Whitehead, Sarah N Hilmer, Lynn Chenoweth, Julia Gilmartin-Thomas, Mouna Sawan, Tuan Anh Nguyen, Edwin Tan, Janet K Sluggett, Lyntara S Quirke, Aisling M McEvoy and Nagham Ailabouni in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We appreciate and acknowledge the input provided by Marie Wittwer as a member of the Stakeholder Steering Group (other members of the Steering Group are listed as authors: AP, TP, LdlP, JT, SD, CW, JD and RS). This work would not have been possible without the Steering Group. We would like to acknowledge our Partner Organizations who supported the project including promotion of the surveys, dissemination of advertising materials, and identification of individuals suitable for key informant interviews: Australian Association of Consultant Pharmacy, Australian Association of Gerontology, Australian College of Nurse Practitioners, Australian Nursing and Midwifery Federation, Consumers Health Forum of Australia, Leading Age Services Australia, National Aboriginal and Torres Strait Islander Health Worker Association, Speech Pathology Australia, The Society of Hospital Pharmacists of Australia. We acknowledge support from StepUp for Dementia Research (https://www.stepupfordementiaresearch.org.au/) in advertising the survey. StepUp for Dementia Research is funded by the Australian Government Department of Health and implemented by a dedicated team at the University of Sydney. We acknowledge support from Dementia Australia in advertising the survey (![]() ).
).
ORCID iDs
Ethical considerations
This study was reviewed and approved by the University of South Australia Human Research Ethics Committee (#202847).
Consent to participate
Step 4 Interim Priority Setting: Consent was implied through completion and submission of the survey. Step 5 Final Workshop: Written informed consent was obtained from all participants prior to the workshop.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Proudly supported by the AAG Research Trust and the Dementia Australia Research Foundation – 2019 Strategic Research Grant.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ER was supported by a NHMRC-ARC Dementia Research Development Fellowship (APP1105777), an NHMRC Investigator Grant (APP1195460), United States National Institutes of Health (NIH) grant and has received royalties for co-authoring a chapter on deprescribing in UpToDate and honorarium from the Society of Hospital Pharmacists of Australia (leading workshops on deprescribing). KC received payment for being an advisor for this study (paid to them via University of South Australia, funded by AAG Research Trust and the Dementia Australia Research Foundation Grant). LMKE was supported by an NHMRC-ARC Dementia Research Development Fellowship (APP1101788). RS, AP, TP, LdlP, JD, JT and SD all received sitting fee payments for participating in this study as Steering Group members (paid to them via University of South Australia, funded by AAG Research Trust and the Dementia Australia Research Foundation Grant). SD has also received payments from Dementia Training Australia (for education), Biogen (Advisory Board member and support for attending meeting) and Roche (Advisory Board member). JG-T was supported by an NHMRC-ARC Dementia Research Development Fellowship (APP1107476). MS was supported by a Dementia Centre for Research Collaboration Fellowship. TAN was supported by an NHMRC-ARC Dementia Research Development Fellowship (APP1103860), an NHMRC-Vietnam National Foundation for Science and Technology Development (NAFOSTED) International Collaborative Research Grant (APP1154644) and is currently supported by an NHMRC e-ASIA Joint Research Program Grant (APP2001548) and an NIH R01 Grant (AG064688). ECKT was supported by an NHMRC-ARC Dementia Research Development Fellowship (APP1107381). JKS was supported by an NHMRC Early Career Fellowship (APP1156439) and an NHMRC Investigator Grant (GNT2016277). NJA is supported by an NHMRC Investigator Grant (GNT1195460).
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author (the data are not publicly available due to privacy or ethical restrictions) or are available within the Supplemental Material.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.