
Abstract
Introduction
Aging is a lifelong developmental process that is often associated with an increased reliance on health-related and support services (Janssen et al., 2011). Old age is often associated with increasingly complex and often interrelated problems, encompassing physical, psychological, and social challenges that can make life more difficult (Janssen et al., 2014). However, through positive aging and adequate support services, well-being of older adults could be improved as older persons are opportune to approach these life challenges in a more positive way (Malone & Dadswell, 2018). Positive aging is seen as an approach that encompasses maintaining a positive attitude, being physically, socially and cognitively active and healthy. Positive aging discourses disrupt the idea that aging necessarily results in a time of morbidity and disability, but views aging as an opportunity for the continued enjoyment of life via diverse forms of activity, engagement and function (Pack et al., 2019). Assisted-living facilities (ALF) can play a significant role in enhancing the well-being of older adults (Formosa, 2019).
ALFs cater for older adults whose chronic physical and cognitive morbidities necessitate social and health services that are unavailable or unfeasible to provide in the community setting (Formosa, 2019). However, some circumstances can truncate the ultimate goals of these facilities thereby making older adult residents’ lives difficult. Older adults may have difficulty adjusting to their new living environments (Umberson & Montez, 2010). Some may feel a loss of control over personal decision making, which may, in turn, affect their overall ability to function and their satisfaction with life (Esliker, 2015). This has led to exploration of factors that could improve the quality of life of older adults in ALFs. Researchers have found that social interactions are a factor in the psychological well-being of ALF residents and have recommended that activities be designed to encourage social interaction and development of social relationships (Umberson & Montez, 2010).
Social activity and involvement with others (which can be in the form of social support and participation) result in an increased ability to cope with age-related challenges, improved self-concept, and enhanced emotional adjustment to the aging process (Oh et al., 2019). Adequate social support, which could come from relatives and close friends, may be necessary to elicit the resilience needed for successful adjustment to the difficulties associated with growing old. Likewise, social participation (which refers to the engagement in recreation, socialization, cultural, educational and spiritual activities (World Health Organization [WHO], 2007). promotes physical health, mental health, intellectual functioning, and serves as a mean by which survival and some informal social support networks are made available for the older adults (Chiao et al., 2011). An individual who is unable to engage actively in the aforementioned activities and enjoy such benefits is thus regarded as having participation restriction. Participation is operationalized through the concept of life habits derived from the Disability Creation Process (DCP) model which specifies the interaction between personal factors (e.g., health condition, physical, and mental capacities), environment barriers or facilitators (e.g., social support) and participation reflected by life habits (Anaby et al., 2011).
Life habits/accomplishments are defined as daily activities such as personal care and mobility, and social roles such as interpersonal relationships and leisure (Anaby et al., 2011). They are regular activities (eating meals, communicating with others, moving around) and social roles (holding a job, studying) that ensure a person’s survival and well-being in society throughout his/her lifetime (unpublished data)). Life habits may be accomplished on a daily basis (e.g. getting into and out of bed, taking a meal) or at various frequencies (e.g., getting around in local stores, planning a budget, taking part in social activities). Two aspects of life habits/accomplishments are suggested by the DCP: (1) accomplishment of participation which refers to the extent to which one can perform an activity independently and with lower level of difficulty; and (2) satisfaction with participation (Anaby et al., 2011).
Owing to the recognition of importance of social lives in aging, a handful of studies had been conducted on social support, social participation, and even life accomplishment among older adults from developed economies. However, there seems to be a dearth of research in these areas among African older adults. This is even truer for older adults in ALFs. These facilities are usually negatively and derisively viewed by Nigerians and most Africans as means by which offspring and extended family members neglect the filial responsibilities of directly taking care of their aged relatives (Amaike & Bammeke, 2014). These ALFs are thus not socially and culturally acceptable (Aboderin, 2006; Akosile et al., 2021). The growing trend of migration of young adults in the quest for a better economic opportunity has resulted in decreasing numbers of children available to care for their aging parents (Adhikari et al., 2011). Older adults are usually left with critical emotional conditions as a result of the harsh disconnection between them and their migrated children; thus making institutionalization of these older adults inevitable. Previous authors have highlighted the need to compare health outcomes (like LA and social participation) between assisted-living and community-dwelling older adults (Akosile et al., 2021); and there may also be a need to assess the perceived social support available to both groups. Available ALFs in Nigeria similarly to many other African nations are mostly poorly-funded and run by non-governmental organizations (NGOs) usually with religious affiliations. They are also often lacking in the type and quality of personnel and resources needed to provide the specialized care and setting associated with ALFs in high-income societies. However, with the continuous explosive increase in the population of older adults especially in developing countries like Nigeria (United Nations, 2013), the negative attitude toward these facilities would hopefully change in no distant time. It is therefore imperative to increase the focus on these facilities, with a view to highlighting their areas of needs. We therefore hypothesized that residents of ALFs would report poorer health outcomes than their community-dwelling counterparts in terms of social support, life accomplishments and social participation. This study was undertaken to explore and compare social support, social participation and life accomplishment between older adults living within communities and those in ALF.
Materials and Methods
Ethical approval was obtained from the Ethical Committee of Nnamdi Azikiwe University Teaching Hospital (NAUTH/CS/66/VOL.8/098). One hundred twenty consenting older adult residents of the ALFs in Nnewi (St. Joseph Home for the Elderly, Uruagu Nnewi), Onitsha (Immaculate Heart of Mary Elderly Home, Oguta Road, Onitsha), and Enugu (Mother of Perpetual Help Home, Enugu) and their adjoining communities participated in the study. The directors of the ALFs and leaders of the communities gave permission and also helped mobilize the residents. Informed consent (written and verbal) was obtained from the participants after adequate information regarding the research had been explained and understood by the participants. Convenience sampling technique was used to recruit consecutive volunteering older adults living in the purposively selected assisted-living facilities and their surrounding communities.
The Multidimensional Scale of Perceived Social Support (MSPSS), Participation Scale (PS), and Life Habits Scale (LHS), were used to measure participants’ level of perceived social support, severity of restrictions, and life habits/accomplishments, respectively. The MSPSS was developed by Zimet et al. (1988) for assessing the perceptions of social support from three sources: family, friends and significant others. It is a 12-item multidimensional scale and each item is scored on a scale of 1 to 7 (Very Strongly Disagree = 1, Strongly Disagree = 2, Mildly Disagree = 3, Neutral = 4, Mildly Agree = 5, Strongly Agree = 6, Very Strongly Agree = 7). The scores of all the items are summed to get the total score. Higher score indicates high social support (69–84), moderate scores indicate moderate social support (49-68), and lower scores indicate low social support (12–48). The scales and its domains reportedly have good psychometric properties (Cronbach’s coefficient alpha = 0.85–0.91, test-retest reliability = 0.72–0.88; Zimet et al., 1988).
The PS measures the severity of participation restrictions. It is an 18-item test with each item scored from 0 to 5. The highest score is 90 while the lowest score is 0. The total score is then categorized into levels of participation restrictions as: 0 to 12 = no significant restriction, 13 to 22 = mild restriction, 23 to 32 = moderate restriction, 33 to 52 = severe restriction and 53 to 90 = extreme restriction). Its items exhibited excellent internal consistency (Crohnbach’s alpha = .92) while its intra-tester and inter-tester reliabilities were 0.83 and 0.80, respectively (Van Brakel et al., 2006).
The LHS assesses participants on 77 life habits from daily activities to social participation across 12 categories (nutrition, fitness, personal care, communication, housing, mobility, responsibilities, interpersonal relationships, community life, education, employment, and recreation). It is a self-report based on one’s perception of difficulty and assistance required. It is composed of two scales: the first assesses accomplishments rated across two dimensions (the degree of difficulty experienced and the kind of assistance required), while the second assesses the patient’s satisfaction with daily activities or social roles. The patient’s satisfaction can range from 1 to 5 (with 5 indicating a high level of satisfaction) (Noreau et al., 2004), while the level of accomplishment are scored as: 9 = No difficulty, No assistance; 8 = No difficulty, Assistive device (or adaptation); 7 = With difficulty, No assistance; 6 = With difficulty, Assistive device (or adaptation); 5 = No difficulty, Human assistance; 4 = No difficulty, Assistive device (or adaptation) and human assistance; 3 = With difficulty, Human assistance; 2 = with difficulty, Assistive device (or adaptation) and human assistance; 1 = Accomplished by a proxy; 0 = Not accomplished; and N/A = Not applicable (Noreau et al., 2004). The intraclass correlation coefficients (ICC) computed for intra-rater and inter-rater reliabilities were >.75 and <.89 respectively (Noreau et al., 2004). The domain of education was removed entirely because the questions in the domain were not applicable to the older adults. This corresponds with what was obtained in previous studies (Desrosiers et al., 2004; Noreau et al., 2004) in which the categories of ‘education and employment’ were removed because of their irrelevance among older adults.
The instruments for this study were self-administered for literate older adults and interviewer-administered for the non-literate older adults. The participants were asked to answer the questionnaires as sincerely as possible. Data analysis was done using the Statistical Package for Social Sciences (version 21). Descriptive statistics of frequency, percentage, mean, and standard deviation were used to summarize participants’ socio-demographics and questionnaire scores. Chi-square test was used to compare socio-demographic variables, social support and participation of older adults resident in the communities and assisted-living facilities. Mann Whitney-U test was used to compare the levels of social support, social participation and life accomplishment of the older adults in the assisted-living facilities and those resident within the surrounding communities. Spearman-rank order correlation was used to determine the relationship between social support, social participation and life accomplishment among each group of older adults. Alpha level was set at 0.05.
Results
A total of 120 older adults participated in this study. Fifty-four (Male = 6; Female = 48) were from assisted living facilities, while 66 (Male = 30; Female = 36) were community-dwelling (CD) individuals. The two groups had significantly different gender proportions (χ² = 16.68, p ≤ .0001) with fewer males in the ALF. Participants from the ALF were significantly older (80.06 ± 10.65 years versus 71.71 ± 7.85 years, t = 4.933, p ≤ .0001), less literate (χ² = 10.38, p ≤ .0001), occupationally inactive (χ² = 31.29, p = .00) and were more likely to be widowed or divorced (χ² = 32.65, p ≤ .0001; Table 1). A significantly higher proportion of older adults in the ALFs suffered some degree of participation restriction compared to those in the communities (χ² = 12.74, p = .01), but the two groups proportionately enjoyed comparable levels of social support (Table 2).The mean MSPSS score however suggested better social support for the community dwelling participants who also had significantly higher life accomplishment and lower participation restriction scores (Table 3).
Socio-Demographics Distributions of Participants.
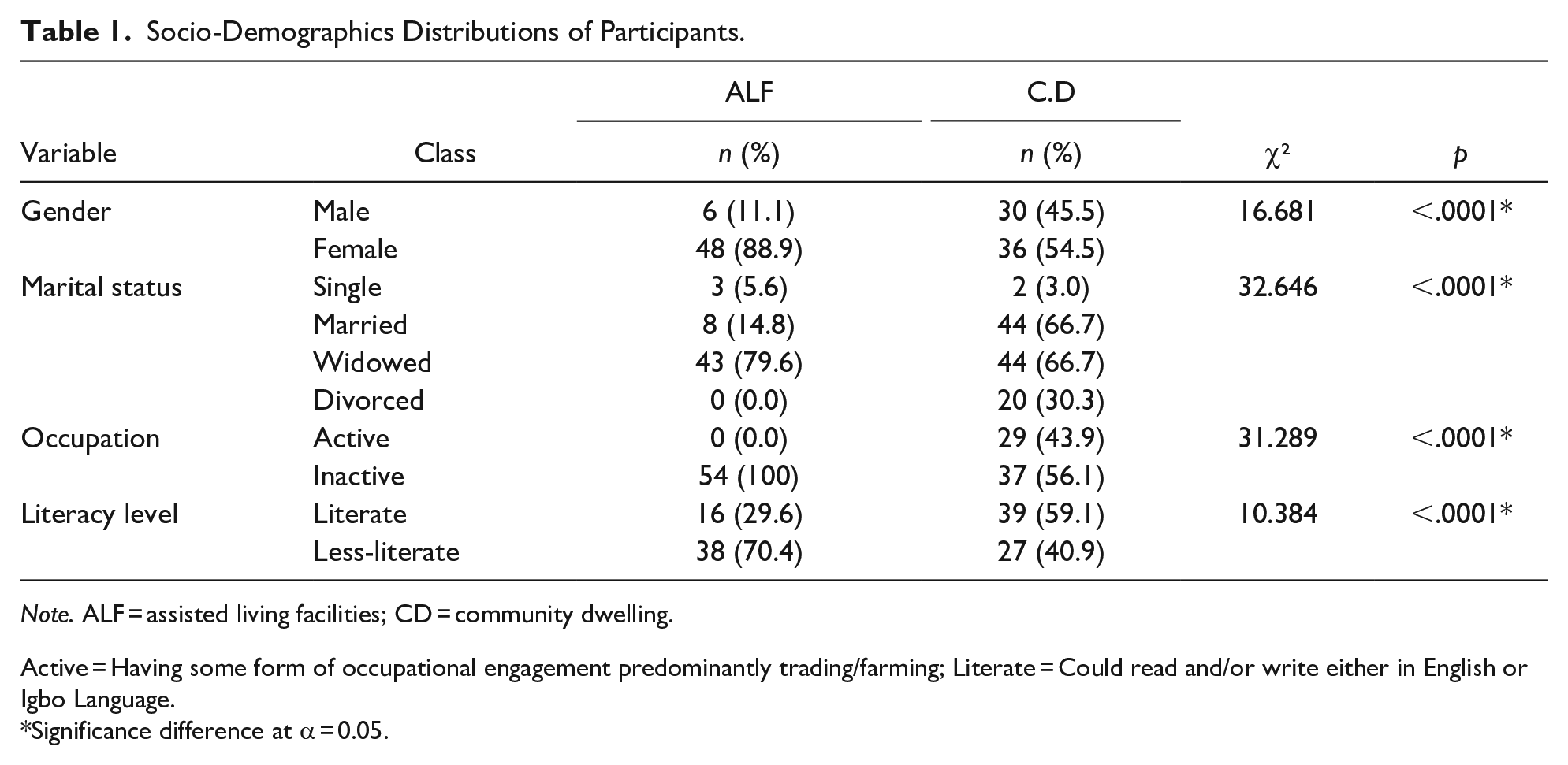
Note. ALF = assisted living facilities; CD = community dwelling.
Active = Having some form of occupational engagement predominantly trading/farming; Literate = Could read and/or write either in English or Igbo Language.
Significance difference at α = 0.05.
Chi Square Table Comparing Levels of Social Support and Participation Between Participants in Assisted Living Facilities and Their Community-Dwelling Counterparts.

Note. MSPSS = multidimensional scale of perceived social support; PS = participation scale; ALF = assisted living facilities group; CD = community dwelling group.
Mann–Whitney Test Comparing Social Support, Social Participation and Life Accomplishment Between ALF and CD.

Note. ALF = assisted-living facilities; CD = community dwelling; PS = participation scale; MSPSS = multidimensional scale of perceived social support; s.d = standard deviation.
When the individual domains of social support and life accomplishment were considered, significant differences between the two groups existed in the family social support domain only and in the life accomplishment domains of fitness, personal care, communication, responsibility and interpersonal relationship (p < .05; Table 4). Life accomplishment had negative and significant correlations with participation restriction for older adults in the assisted-living facilities (r = −.44, p ≤ .0001) and their community-dwelling peers (r = −.62, p ≤ 0.0001). However, no significant relationship was found between social support and life accomplishment and between social support and social participation for either group of participating older adults (Table 5).
Mann-Whitney Test Comparing Domains of Social Support and Life Accomplishment Between ALF and CD.

Note. ALF = assisted living facilities; CD = community dwelling; Life H = life habit scale; MSPSS = multidimensional scale of perceived social support.
Spearman Rank Correlation Testing the Relationship Among Social Support, Social Participation, and Life Accomplishment in Assisted Living Facilities and in Community Dwelling.

ALF = assisted living facilities; CD = community dwelling; SS = social support; SP = social participation; LA = life accomplishment.
Discussion
This study explored and compared the levels of social support, social participation and life accomplishments among CD older adults and their counterparts’ resident in ALFs. The study also explored the relationships between these variables in each of the two groups of older adults. The findings of this study demonstrated that residents of the ALFs had significant poorer levels of social support, social participation and accomplishment of the life habits compared to those dwelling within communities. Social participation and life accomplishment was the only construct pair with significant correlation among participants in both study groups.
Results revealed a significantly lower level of social support in older adults in ALFs, with a good proportion receiving moderate support while majority of their counterparts in the community received high support. The fact that older adults residing in ALFs were significantly older and had more widowed participants than their counterparts in the communities might explain the lower social support in the former. Studies have suggested that available social support dwindles with increasing age as disabilities or physical frailties (Frady, 2014). Being widowed had equally been reported to associate with a feeling of loss of social support (Dai et al., 2016; Frady, 2014). Even though the influence of marital status on social support was not explored in the present study, it could be assumed that higher proportion of widowed older adults in ALFs compared with their peers residing in the community could have contributed to their poorer social support status. Results of the present study also revealed that older adults in the ALFs received a significantly lower amount of support from their family but showed no significant difference in social support from friends between the two groups of participants. Family and friends are reportedly major sources of support and act independent of each other (Sato et al., 2008). It may be possible that the support available to ALF groups from their families did not meet their needs. It has been previously suggested that while people (who have to function outside their home environment) tend to appreciate more whatever form of support or solidarity is offered by friends and significant others, higher expectations from family members may make the support they offer to be undervalued (Akosile et al., 2018). This is more likely the case for ALF residents who may already perceive their placement in such facilities as neglect of responsibility by family members. Lack of significant difference in social support from friends between the two groups could stem from the fact that participants in the ALFs usually cultivate new friendship with their caregivers and fellow residents (Ziemba et al., 2008) who provide them with the required social support thereby masking the loss of support from their former friends. A recent local study had also reported a high level of social support among community-dwelling older adults (Okoye et al., 2022).
This study revealed a significantly higher level of participation restriction among older adults in ALFs. The mean age for participants in this group was significantly higher than that of the CD group. A previous study by Desrosiers et al. (2004) found social participation to significantly decrease with advancing age. Furthermore, even though the prevalence of depression was not investigated in this study and thus was not compared between groups, other authors have reported this also increase with advancing age (Gureje et al., 2008).Samus et al. (2006) opined that persons with behavior problems or depression were not likely to participate in activities often. The possibility does exist that depressive symptoms may be more prevalent in the ALFs group (not just because they are in the facilities but because they are much older) and may have contributed to their reduced social participation. Akosile et al. (2017) had actually reported strong correlations between depression and reduced social participation and also functional disabilities in social activities and quality of interactions among a community-dwelling sample of Nigerian older adults.
Older adults in ALFs had significantly lower scores in accomplishment of life habits. This corresponds with Desrosiers et al. (2004) findings that scores of older adults in long term facilities were lower in accomplishment of life habits than that of older adults in communities and private care homes. The fact that older adults in ALFs were significantly older than their CD peers in the present study might have contributed to the differences in their life accomplishments. Limitations in physical function in the older adults have been reported to be linked to aging, and a decrease in performance of activities of daily living (ADL) which may contribute to the lower levels of accomplishment of life habits (Akosile, Odidika et al., 2014). The social aspects of living in ALFs have been found to be central to the residents’ quality of life (Esliker, 2015), a construct that is closely related to life accomplishment. Having a good social network along with good social support and ability to accomplish life habits may individually and corporately influence the well-being of older persons (Sato et al., 2008).
Among all the domains of life habit, older adults in both groups had their lowest scores in the communication domain. Also, items in this domain assessed literacy levels. The lower literacy level among sampled older adults may have contributed to the lower levels of communication. Dai et al. (2016) opined that older people who have a higher educational level may have better communication ability and interpersonal skills and may be able to utilize support resources more actively. Participants’ score in the fitness domain was significantly lower for the ALFs group. This may be due to the fact that older adults in ALFs were significantly older and had more female and occupationally inactive participants than CD older adults. Older age has been associated with poor physical health (Janssen et al., 2011). Occupational inactivity along with female gender have been shown to be strongly associated with fear of falling (Akosile, Odidika, et al., 2014; Akosile, Agu et al., 2014; Akosile, Anukam, et al., 2014) and its attendant negative consequences on fitness-related variables. These variables may include limitation and/or reduction in the performance of activities of daily living, mobility, physical and balancing activities, quality of life, and increased institutionalization among older adults (Akosile, Odidika, et al., 2014).
ALFs group performed significantly worse than their CD counterparts in personal care, interpersonal relationships and responsibility domains of life accomplishment. This result is logical as personal care and interpersonal relationships are respectively closely related to participation and social support which were equally worse in the former group. Functional dependency had also been reported to be a predictor of nursing home placement among older adults (Smith et al., 2001). Hence, the observed difference in personal care and responsibility among the two groups might have been from a baseline difference rather than being orchestrated by institutionalization. The older age of the ALFs group and the fact that institutionalized older adults are highly prone to behavioral symptoms may account for the poorer personal care, interpersonal relationships and responsibility domains of life accomplishment recorded in this group in the present study (Horowitz & Vanner, 2010). The lack of significant differences in the nutrition and housing domains of life accomplishment between the two groups of older adults may be suggesting that ALFs provide housing and nutrition comparable to what older adults receive in the communities. Education and employment domains of life accomplishment were not considered in the present study as they were considered as having negligible importance among older adults.
There was a direct significant relationship between social participation and life accomplishment, with participation restriction hindering accomplishment of life habit. This is similar to a previous report (Desrosiers et al., 2004). This result is not surprising as restricted participation in life activities can logically mitigate one’s accomplishment in life. There was no significant relationship between social support and each of life accomplishment and social participation in either of the two groups of older adults in the present study. This opposes a previous report of significant relationship between social support and accomplishment of life habits among older adults (Ahmad, 2011). No previous study seemed to be readily available on the relationship between social support and social participation. However, increased social support had been reported to improve quality of life (a construct similar to life accomplishment) among older adults (Perissinotto et al., 2012; Wicke et al., 2014). The lack of significant relationship between social support and social participation corroborates results of an unpublished local study among older adults. These results may suggest that sampled older adults were able to have meaningfully socially participation and accomplish their life activities irrespective of the level of social support available to them.
The study has some limitations which must be acknowledged. The cross-sectional design of this study does not allow for ascertaining cause and effect relationships among the variables. The small size of the study necessitated by the number of available residents in the ALFS also means generalizing the findings has to be done with some caution. However, this study is one of the very few providing an African perspective on the studied constructs and hopefully may be useful for international comparison.
Conclusions
Older adults in ALFs received moderate social support, had low life accomplishment, and a high participation restriction, while CD older adults received a high social support, had a high life accomplishment and had no participation restriction. There were significantly poorer scores of social support, social participation and life accomplishment in older adults in ALFs in comparison to their community dwelling counterparts. Social participation and life accomplishment significantly correlated directly with each other but not with social support in both groups. This study therefore recommends that older adults in the ALFs who are not too physically strong should be encouraged to have some level of independence and responsibilities within the facilities, and that managers of ALFs should improve areas of social activities and vocational engagements in the facility in order to decrease the levels of participation restriction among them. Families of older adults in ALFs and CD should strive to improve on the level of support they give to their older adults in order to improve their quality of life.
Footnotes
Acknowledgements
None.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The Ethical Committee of Nnamdi Azikiwe University Teaching Hospital (NAUTHEC) gave approval for this cross-sectional survey.