
Abstract
Older adults have a high burden of chronic diseases but are underrepresented in research. Researchers with geriatric or gerontology expertise have developed frameworks to recruit and retain older adults but these have not been widely adopted by the broader research community. We developed or adapted seven Age-Friendly research tools and invited research team members with no aging training to pilot test them. We consented 21 research team members and asked them to share strengths, limitations, and areas for improvement for each tool for up to 4 months via REDCap surveys. Sixteen participants (76%) completed at least one survey. The communication guide and Age-Friendly research checklist were the most utilized tools among participants. Key barriers to implementation were lack of time and lack of age-appropriate populations. Facilitators of tool implementation were accessibility and ease of use, webinar training, and supportive teams. Participants found the tools valuable to encourage Age-Friendly research studies. Adoption of Age-Friendly research tools could improve the experience for research team members and older adults alike.
Older adults, especially those over 80, are vastly underrepresented in research on diseases prevalent in that age group (Lockett et al., 2019). Underrepresentation has been attributed to assumed challenges and complexities with this population such as navigating cognitive impairment, medication interactions, transportation, and comorbidities (Nguyen et al., 2022). In 2021, only 19% of National Institutes of Health (NIH)-funded research participants were 65 years and older (Bowling et al., 2023). Research studies often have exclusion criteria that inherently exclude older adults including arbitrary age limits, multiple comorbidities, cognitive status, and medication use (Hunold et al., 2022). This limits the applicability of research findings from younger populations that have a lower disease burden and less complications to older adults in whom the condition being studied might be highly prevalent (Hunold et al., 2022). The NIH noted this growing disparity and implemented the Inclusion Across the Lifespan policy in 2019 to increase inclusion of older adults in research (National Institutes of Health, 2017). Despite these efforts, many research team members who study conditions common in older adults but who have no specific geriatric or gerontologic training still lack the skills and resources to confidently recruit and retain older adults in their studies.
The Institute for Healthcare Improvement and John A. Hartford Foundation designed the Age-Friendly Health Systems initiative focused on the 4Ms—What Matters, Mentation, Medication, and Mobility—to improve evidence-based and goal-aligned clinical care and has shown promising results for improved outcomes for older adults that receive Age-Friendly care (Breda et al., 2023; Mate et al., 2021). The 4Ms Framework has been applied in education to prepare learners for the needs of older adults but has yet to be implemented in research (Greenberg et al., 2022; Johnson et al., 2023; Severance et al., 2023). Duke and Emory University created the 5Ts Framework—Target population, Teams, Time, Tips, and Tools—to support research teams without expertise in aging by offering practical strategies to encourage inclusion of older adults in research (Bowling et al., 2019). The 5Ts Framework can help anticipate research participation barriers among older adults and suggest possible solutions (Thomas et al., 2023). We utilized the 4Ms Framework, the 5Ts Framework, and the Inclusion of Older Adults in Clinical and Translational Research toolkit, which was developed by a group of aging experts across the Clinical and Translational Research Award (CTSA) Network to guide translational researchers in inclusion of older adults (CLIC-CTSA, 2021).
These frameworks guided our development of what we consider an “Age-Friendly research environment”: ensuring that all older adults aged 65 and older have equitable access to research enrollment and the necessary accommodations to fully participate in research. Features of Age-Friendly research include committing to include older adults, especially older adults from diverse backgrounds, in research; using age-appropriate language (e.g., avoid othering terms such as “elderly”); attending to specific needs (cognitive impairment, hearing impairment, visual impairment, mobility impairment); and designing institutional policies and infrastructure to optimize the older adult experience, among others.
Our team conducted an Age-Friendly research pilot study for research members. The primary goal was to create an Age-Friendly research environment at our institution by sharing knowledge, strategies, and tools. This paper focuses on the development and pilot testing of Age-Friendly research tools. We assessed the feasibility and acceptability of utilizing these tools in the older adult population and identified facilitators, challenges, and potential suggestions for improvement.
Methods
Study Population
We reached out to research members employed at our institution through personal connections and institution-wide sources such as newsletters and networks. Potential participants were ineligible if they claimed to have gerontology or geriatric expertise including training, degree or certification, and practice experience. This allowed us to assess feasibility and acceptability of tools for the general research population. Participants chose to (1) attend an educational, interactive webinar series and/or (2) pilot test Age-Friendly research tools. Eighteen participants consenting to pilot test the tools simultaneously participated in the webinar series (De Lima et al., 2023).
Interested participants agreed to test the Age-Friendly research tools on their study populations for 4 months and complete monthly online surveys in Research Electronic Data Capture (REDCap, Vanderbilt University), a database tool developed within the CTSA network. Survey questions included what tools were implemented so far and how, facilitators and barriers to implementation, recommended changes, requested support, and if tools were valuable or feasible and why (Supplemental File 1). Participants attended three video calls for an introduction of tools and survey questions and check-ins throughout the study. To encourage diversity and welcome research members of all levels, no demographic or research experience data were collected. Participants received a $1,000 stipend in recognition of the many hours of their time and expertise they were contributing. All participants provided written informed consent. The study was approved by our Institutional Review Board. (#24539).
Tool Development
We consulted with an institution-wide advisory board of expert researchers to identify potential tools that could assist research members to recruit and retain older adults. From these conversations and the three frameworks that guided our project, we developed three research tools and adapted a fourth research tool to address common challenges and support the research community in including older adults in research. These tools were a communication guide for older adults, an Age-Friendly research checklist, a geriatric assessment tool, and a knowledge check to assess capacity to consent to a research study. Study participants were invited to suggest additional tools, and we created three additional tools at their request including a condolence card template for families of research participants who died during a research trial, a guide to help make industry-sponsored trials more Age-Friendly, and a tip sheet addressing common barriers to inclusion of older adults.
Each tool was created or adapted from evidence-based resources to benefit research members in the inclusion of older adults. Participants were trained on the purpose and how to use each tool during a video call and encouraged to pilot test as many of them as possible in their study population. All tools were shared via email and posted on a cloud-based OneDrive folder. See Supplemental File 2 for the comprehensive toolkit. The tools are briefly explained here with their purpose and impact on the inclusion of older adults in research.
Knowledge Check to Assess Capacity for Informed Consent. This tool was based on the Capacity for Informed Consent document from the SAGES study at Hebrew SeniorLife and Harvard Medical School designed by Sharon K. Inouye, MD, MPH and Eva Schmitt, PhD and used with their permission. The short, 5-question knowledge check is meant to be administered after potential study recruits review the consent form with the study team. The assessment checks the potential recruit’s understanding of the study (e.g., what are the main risks of participation in this study?) and suggests a legally authorized representative if capacity to consent to the study is in question. The knowledge check recognizes study participants with cognitive impairment. The research team can then modify processes such as informed consent and scheduling visits.
Analysis
Participants completed up to four monthly REDCap surveys on their experience with the tools. Frequencies were calculated for the tools implemented and value and feasibility of them in R version 4.1.3 (R Core Team, 2022). Open-ended survey responses were uploaded into Dedoose version 9.0.107 (SocioCultural Research Consultants, 2023) and analyzed for themes by study team members using conventional content analysis (Hsieh & Shannon, 2005).
Results
Survey Participants
Twenty-one research members consented into our tool development pilot study and 17 (81.0%) were female. Sixteen (76.2%) completed at least one survey. Nine participants completed all four surveys and 11 completed three. Participants were from Cancer (66.7%) and Neurology (28.6%) departments with roles such as research assistant (33.3%), research coordinator (28.6%), or other (38.1%).
Survey Results
Participants had the most success implementing the communication guide and the Age-Friendly research checklist with their study populations (Figure 1). Participants shared they now “send emails in larger font sizes (size 14) to the participants in the studies rather than the size 11 or 12 font,” “allow more time and speak more slowly,” and “keep the checklist in mind” to be more Age-Friendly. Five participants were unable to implement the tools in their research studies. Some challenges that they identified were no time, recruitment ended, study population base not appropriate, industry-sponsored projects, and remembering to use them. By the end of the study, most participants found the tools valuable (n = 14) and feasible (n = 13) to implement in their research studies

Frequency of tool utilization among participants.
Qualitative Themes
We identified six themes related to facilitators and suggestions for tool implementation (Table 1). The three facilitators of tool implementation were accessibility and ease of use, webinar training, and supportive teams. Six participants shared that the availability of the tools on OneDrive helped with implementation. The three areas for suggested improvement were tool modification, more applicable for industry-sponsored studies, and education. Participants suggested minor changes to the Age-Friendly checklist, communication guide, and knowledge consent check. Incorporating social work for care coordination, increased accessibility, and IRB pre-approval of tools were identified as ways to help disseminate Age-Friendly research and increase the use of these tools in research studies.
Themes and Representative Quotes for Implementing and Improving Age-Friendly Tools.
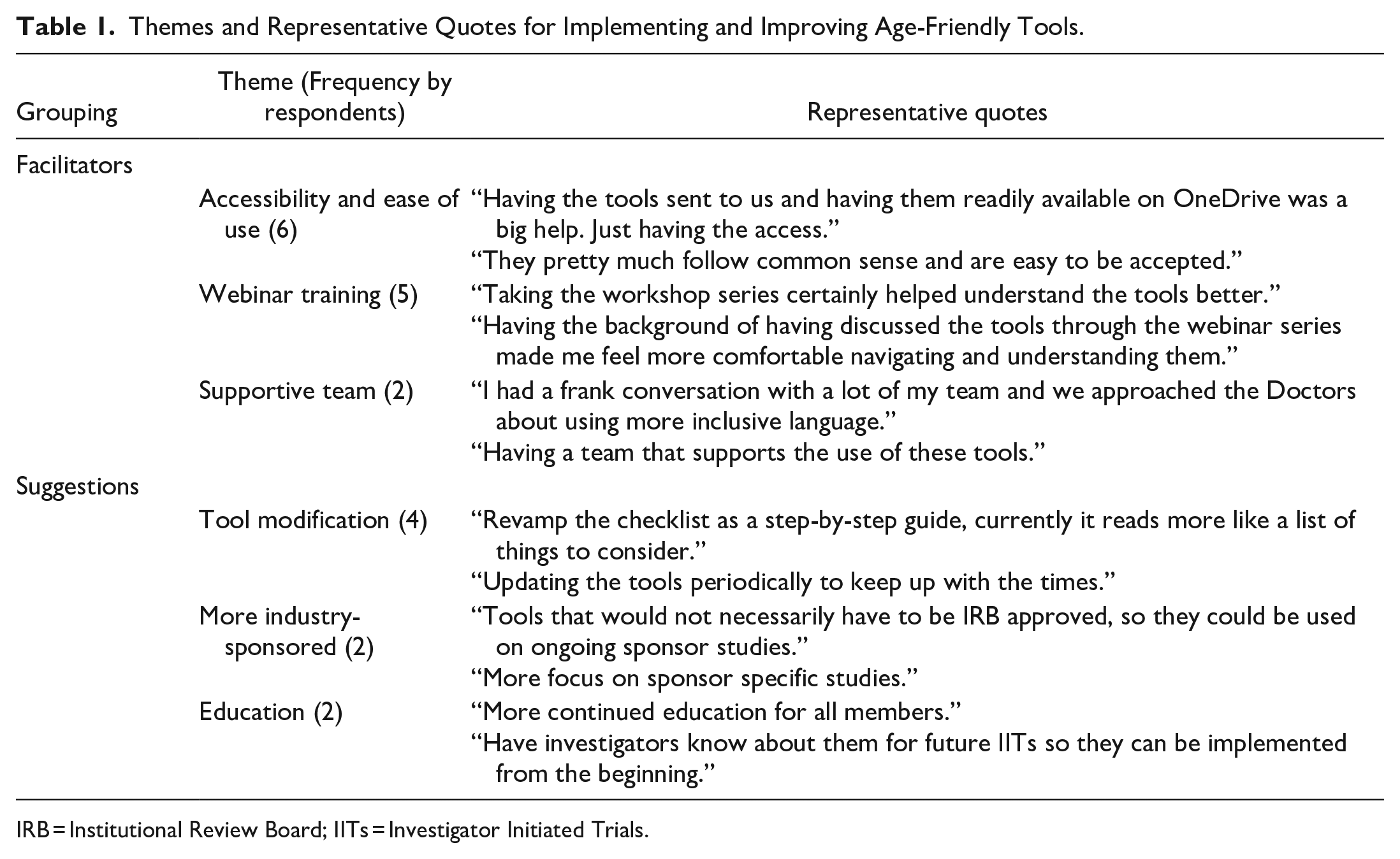
IRB = Institutional Review Board; IITs = Investigator Initiated Trials.
Discussion
This is the first pilot study to our knowledge that adapted frameworks and initiatives developed by aging-trained research members for use by the general research community to create a more inclusive and Age-Friendly research environment. Our team developed or adapted seven tools to increase the inclusion of older adults in research. While only 11 participants (68.9%) reported that they tested a tool in their study population, over 81.3% felt the tools would be valuable and feasible to implement. Participants felt the tools were easy to use and accessible but slight modifications and continued education would improve their utility. These tools helped fill a gap—often one that the participant did not even know existed.
Our Age-Friendly tools aimed to tackle well-known barriers to inclusion of older adults in research highlighted by Nguyen et al. (2022) and Hunold et al. (2022). Tools such as the communication guide and research checklist address some of the 14 best practice recommendations for including older people in research related to individual, interpersonal, and community factors (Goodwin et al., 2023). These include tailoring communication to the needs of older adults; removing exclusion criteria based on age, comorbidities, and cognitive impairment; involving advocates and peers when designing research; and considering the involvement of caregivers. Small changes such as increasing font size on recruitment material and allowing extra time for study visits can improve experiences and lead to better representation of older adults in research.
Limitations and Future Directions
This study has all the limitations of a pilot study—one institution, relatively small sample size, and inability to track study recruitment and enrollment to see if more older adults were truly included. Our advisory board included translational scientists and researchers from cancer and other specialties, and included some with and some without expertise in clinical trials and aging, as well as members whose focus is on diversity, equity and inclusion, helping to ensure our trainings would be feasible and generalizable.
This study offers tools that are potentially feasible and useful for any research team aiming to match the demographics of their enrolled population to the demographics of the disease or condition of interest, and any research center or institute that hopes to ensure their research environment is Age-Friendly and can support inclusion of the oldest adults in trials of diseases that are highly prevalent in people in their 80s, 90s, and 100s. Future studies could implement these tools on a larger scale and with more robust outcome measures so they could be more widely disseminated across the research community to improve the experience for everyone. We encourage research teams who study diseases and conditions in older adults to expand the age categories of studies, so rather than having one age group for “65+,” divide groups into 65 to 74, 75 to 84, and over 85 (or similar) (Zauflik & Eckstrom, 2020). We also encourage all research teams to reach out to geriatric and gerontology-trained colleagues and invite them to be part of research teams when the disease or condition they are studying includes older adults. Funders could encourage or mandate inclusion of aging experts in studies of heart disease, cancer, and other conditions prevalent in older adults. Together, we can ensure that even the oldest members of our population have the ability to contribute meaningfully to advances in medical research.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214241236037 – Supplemental material for Age-Friendly Research: A Pilot Exploration of Tools to Facilitate Inclusion of Older Adults in Research
Supplemental material, sj-docx-1-ggm-10.1177_23337214241236037 for Age-Friendly Research: A Pilot Exploration of Tools to Facilitate Inclusion of Older Adults in Research by Bryanna De Lima, Allison Lindauer and Elizabeth Eckstrom in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-2-ggm-10.1177_23337214241236037 – Supplemental material for Age-Friendly Research: A Pilot Exploration of Tools to Facilitate Inclusion of Older Adults in Research
Supplemental material, sj-docx-2-ggm-10.1177_23337214241236037 for Age-Friendly Research: A Pilot Exploration of Tools to Facilitate Inclusion of Older Adults in Research by Bryanna De Lima, Allison Lindauer and Elizabeth Eckstrom in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We would like to thank Meredith Zauflik, MPA, for her advising on the tool development process. We would like to acknowledge Karen Bandeen-Roche, PhD; Cynthia Boyd, MD, MPH; C. Barrett Bowling, MD; and Mark Supiano, MD for their contribution to the Age-Friendly research environment definition. We would also like to acknowledge the wisdom and practical suggestions offered by our Age-Friendly Research Advisory Committee: David Dorr, MD; Jackie Shannon, PhD; Kerri Winters-Stone, PhD; Eneida Nemecek, MD; Deanne Tibbitts, PhD; Kitt Swartz, MPH; Gabrielle Meyers, MD; and Lindsey Zimmerman, PhD. The study is not pre-registered and data and materials are available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Inter-NIA Center/CTSA Hub Grants For Implementation Activities in Support of Inclusion of Older Adults in Clinical Trials through the Research Centers Collaborative Network (RCCN) of the National Institute on Aging, National Institutes of Health. The RCCN is managed by Wake Forest University School of Medicine and the American Federation for Aging Research and funded by the National Institute on Aging, National Institutes of Health Award Number [U24AG058556]. This work was also supported by the National Institute on Aging [P30-AG066518].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.