
Abstract
The number of older LGBTQ+ adults is growing worldwide. Yet few studies outside of the United States have examined their experiences of aging. Drawing on the Health Equity Promotion Model and contextualized in Canada’s unique socio-political history, our study used multiple, in-depth, qualitative interviews to examine 30 older Canadian LGBTQ+ adults’ (aged 65–83) perceptions and experiences of growing older. Our descriptive thematic analysis identified three overarching categories: “Losses,” “gains,” and “needs.” Losses referred to the changes in the participants’ health, autonomy, and relationships that had occurred with age. Gains entailed positive later life changes, including increased wisdom, flexibility, and social connections. Finally, needs referred to those things that the participants deemed essential for aging well, namely, inclusive health care, meaningful activities, and supportive networks. We discuss the policy and practice implications of our findings for the fostering of health, well-being, and social inclusion amongst this often-marginalized population.
• Our study provides a Canadian example of how older LGBTQ+ adults perceive and experience aging as a time of progressive and inevitable declines and social losses. • Increasing social inclusion and legal protections for gender and sexually diverse individuals in Canada underpinned the participants’ perspectives on positive changes they had experienced as older LGBTQ+ persons. • Participants feared that heightened vulnerability in late old age would make them susceptible to future discrimination and social exclusion.
• Similar to other countries, there is a need for more culturally safe, gender-affirming, and trauma-informed care in clinical, mental health, social service, and long-term care settings in Canada. • Service providers as well as health and social programs in Canada need to more clearly signal and overtly demonstrate that they are inclusive to allay the fears of older LGBTQ+ adults as well as foster opportunities for them to develop and maintain social connections in later life. • Canadian aging-related health and social programs need to be more LGBTQ+ inclusive and those targeting LGBTQ+ persons need to be more age-inclusive.What this paper adds
Applications of study findings
Literature Review
Even as their numbers worldwide continue to grow (Fredriksen-Goldsen & De Vries, 2019), older lesbians, gays, bisexuals, transgender persons, queer individuals, and members of gender and sexually diverse minorities (LGBTQ+) remain largely invisible and under-represented in the research. The bulk of the studies have been conducted in the United States, finding that older LGBTQ+ adults are predisposed to physical and mental illnesses due to discrimination and the accumulation of disadvantage over the life course (Dubois & Juster, 2022; Fredriksen-Goldsen et al., 2023). The research further indicates that systemic discrimination delimits their access to appropriate and culturally competent supports and services (Fredriksen-Goldsen et al., 2018). Consequently, older LGBTQ+ persons report feeling unsafe in health care spaces (Putney et al., 2018) where they are often hesitant to disclose their gender and sexual identities for fear of potential unconscious bias and overt discrimination from health care professionals (Burton et al., 2019), especially in long-term care facilities (Caceres et al., 2020). Older LGBTQ+ adults further worry that they will be pushed back into the closet, (Cummings et al., 2021), outed (Fredriksen-Goldsen et al., 2023), isolated (Putney et al., 2018), neglected (Averett et al., 2020), or mistreated in health care contexts (Kittle et al., 2023). Therefore, the research suggests a need for more LGBTQ+ inclusive and gender-affirming care, which includes a set of behaviors, practices, and interventions that are respectful and supportive of diverse gender identities and sexual orientations (Putney et al., 2018).
At the same time, the predominantly American research has established that older LGBTQ+ adults experience unique social issues as they age. They often report a loss of kinship bonds due to familial rejection and estrangement (Adan et al., 2021). Relying more on their friends than their biological kin for support as compared to their heterosexual counterparts (Hsieh & Wong, 2020), they frequently articulate the fear that declining health might increase their social isolation (Perone et al., 2020). Older LGBTQ+ adults also report feeling excluded from or lacking access to sub-cultural spaces (Cummings et al., 2021). They further describe feeling lonely, isolated, and lacking in social connections, often due to relocation or the death of friends, partners, and family (Perone et al., 2020). Underlying these social issues is the fact that older LGBTQ+ adults are frequently in precarious financial situations with concomitant negative impacts on their housing security (Boggs et al., 2017), end-of-life planning (Boulé et al., 2020), and access to essential health and social services (De Vries et al., 2019).
Some studies have found that older LGBTQ+ individuals experience positive social changes in later life. Cummings et al. (2021) reported that older American LGBT adults tended to share strong connections with each other because of their shared history of oppression. The older American lesbians in Putney et al.’s (2016) study indicated that because of the stigma and discrimination they had faced in their earlier years, they had developed coping strategies that enabled them to be more self-confident and resilient in later life. In interviews with older American lesbian women and gay men, Barbee (2022) found that a history of stigma fueled participants’ motivations to cultivate stronger intergenerational ties, mentor the younger generations, and advocate for LGBTQ+ rights.
To date, the bulk of the gerontology research concerning older LGBTQ+ adults has entailed focus groups conducted primarily in the United States and centered around health and social service issues. Few studies have examined older LGBTQ+ adults’ general experiences of growing older and there has been relatively little attention paid to older Canadians. Yet, Fredriksen-Goldsen and De Vries (2019) have noted that older LGBTQ+ adults’ experiences of aging are shaped and constrained by the unique historical, environmental, and cultural context of the countries in which they reside. Canada is distinctive in terms of its legislation, which has impacted the lives of older LGBTQ+ adults (Boulé et al., 2020). For example, in 1969, Canada decriminalized homosexuality, followed by amendments to the Canadian Human Rights Act to include sexual orientation in 1996 and gender identity in 2017 as prohibited grounds of discrimination (Government of Canada, 2022). In 2005, Canada became the third country in the world to legalize same-sex marriage (Overby et al., 2011). Thus, today’s older Canadian LGBTQ+ adults have faced major socio-political shifts over their lifetimes resulting in unique aging-related experiences and needs (QMUNITY, 2018). Despite progressive legislative changes, a few studies have found that older Canadian LGBTQ+ adults fear they will experience a loss of rights (Boulé et al., 2020) as they age as well as an inability to advocate for themselves and their loved ones (Furlotte et al., 2016). However, questions remain about what it is like to grow older as a Canadian LGBTQ+ adult.
Seeking to understand how older Canadian LGBTQ+ adults perceive and experience aging, we drew upon Fredriksen-Goldsen et al.’s (2014) Health Equity Promotion Model, which considers how health and social outcomes are impacted by behavior, social relationships, psychology, and biology. The model stipulates that health-promoting pathways or “resilience factors” (p. 657), such as community supports and psychosocial coping skills, may positively counteract adverse stressors such as discrimination and marginalization (Fredriksen-Goldsen et al., 2014). Unique combinations of health-promoting pathways and adverse stressors are proposed to explain why health trajectories may differ among LGBT individuals who share similar life experiences (Fredriksen-Goldsen et al., 2014). The framework’s emphasis on the interplay between vulnerability and resilience, as well as the individual- and societal-level factors that shape health and well-being was of particular importance to our research aims. Using the framework and building on the existing research, the purpose of our study was to examine the aging-related perceptions and experiences of older Canadian LGBTQ+ adults. Thus, we sought to gain insights into how older LGBTQ+ Canadians perceive and experience both vulnerability and resilience as they navigate the social and physical realities of growing older as well as the particular needs they identify as being important for their health and well-being in later life.
Methods
Participant Selection and Setting
We recruited 30 participants via a poster campaign in public locations in the Greater Vancouver Regional District, advertisements in older adult and LGBTQ+ organizational newsletters, snowball sampling methods, and the help of community contacts. LGBTQ+ individuals were eligible to participate if they (a) were aged 65 years or over, (b) self-identified as lesbian, gay, bisexual, transgender, queer, or another gender or sexual minority, (c) had spoken proficiency in English, and (d) were community-dwelling. Interested participants contacted the first author either by telephone or email and were subsequently sent an information package. Participants who met the inclusion criteria and provided written informed consent were interviewed twice, approximately four to six weeks apart at mutually convenient times and locations. Recruitment continued until we had obtained a sample that was diverse with respect to the participants’ ages, gender identities, and sexual orientations.
Data Collection
All but one of the participants were interviewed twice, either in person (15 participants), by telephone (10 participants), or by Facetime or Skype (five participants) for between 2.5 and 6 hours (for an average of 4 hours and a total of 113 interview hours). One participant was interviewed three times to accommodate their schedule. No participants withdrew from the study. Ethical approval was received from the Behavioural Research Ethics Board of the University of British Columbia. The first author has a clinical social work background, is a professor (of sociology), and has extensive qualitative research experience with older adults. She conducted 58 of the 61 one-on-one interviews, with the remaining three completed by a graduate trainee under her close supervision. The interviewers established rapport with the participants by introducing themselves and describing the purpose of the study.
Interview Guide.
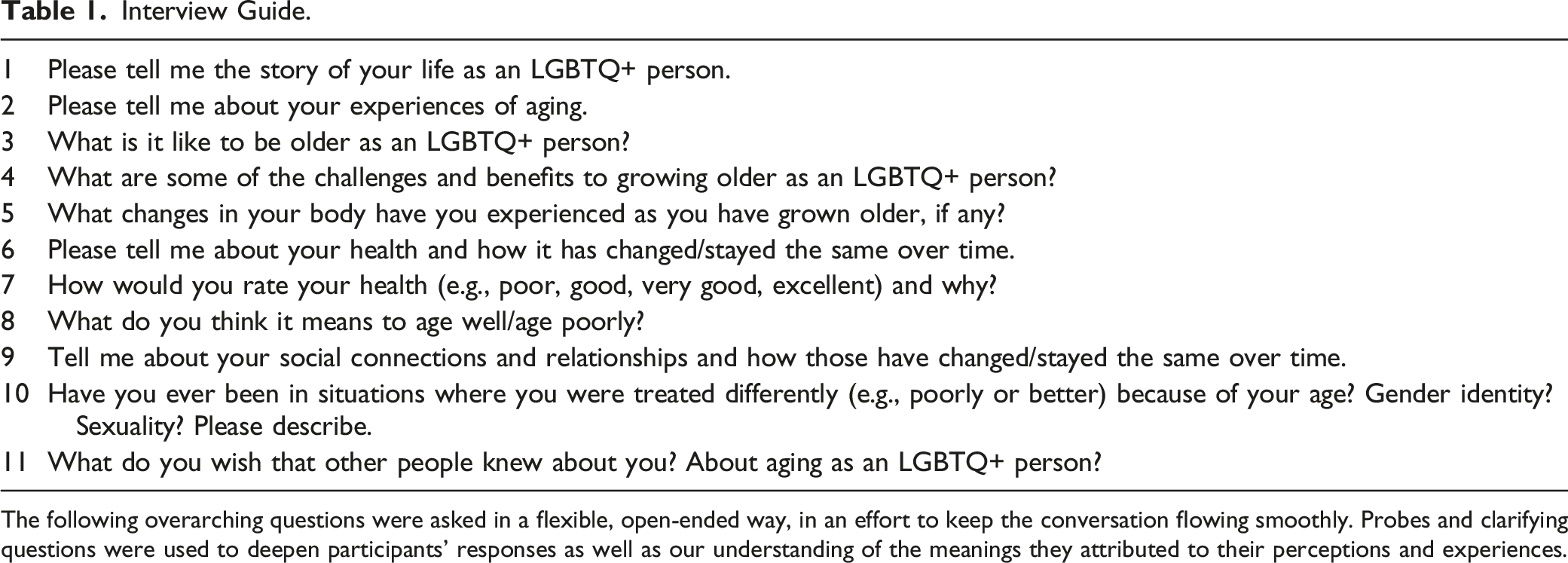
The following overarching questions were asked in a flexible, open-ended way, in an effort to keep the conversation flowing smoothly. Probes and clarifying questions were used to deepen participants’ responses as well as our understanding of the meanings they attributed to their perceptions and experiences.
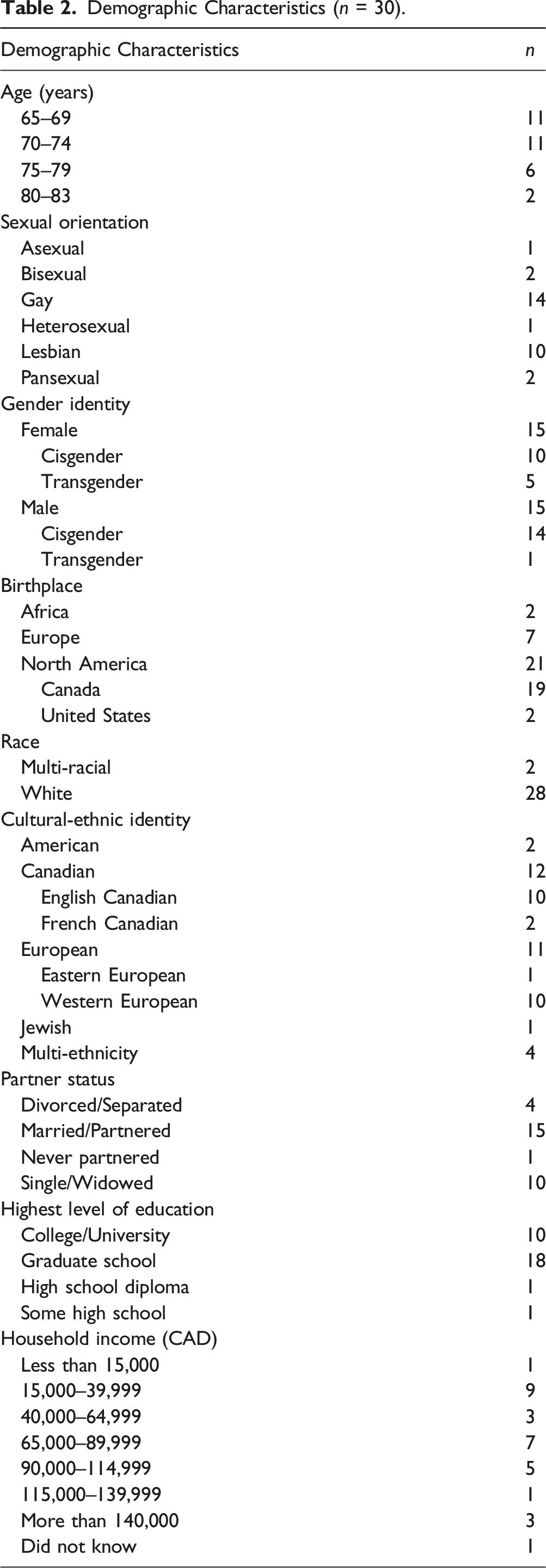
Participant Characteristics
Demographic Characteristics (n = 30).
Data Analysis
Using descriptive thematic analysis (Colorafi & Evans, 2016), the data were analyzed deductively and inductively by the first and second authors, with the support of another research assistant. Guided by our review of the literature and the Health Equity Promotion Model’s focus on the structural, environmental, and individual-level factors that shape minority health (Fredriksen-Goldsen et al., 2014), the deductive codes included individual and societal-level barriers to social engagement and access to health and social resources. The inductive coding process was driven by our data, whereby we repeatedly read the transcriptions, attending to the underlying and readily apparent meanings that the participants attributed to their perceptions and experiences of aging (Fereday & Muir-Cochrane, 2006). The resultant codebook (which can be found in the Supplementary Materials) included the following sub-codes: Health and physical functioning, independence and autonomy, social disconnection, aging-related wisdom, material and non-material freedom, social connection, access to health and social resources, and occupational engagement. We coded our data using NVivo 12 software (QSR International Pty Ltd, 2023) and then subsequently used Microsoft Excel to assist in the process of identifying patterns in our coded data. To establish inter-coder agreement, the first and second authors, as well as the research assistant, independently examined a subset of the coded transcripts. When discrepancies were identified, we considered the text as a group and collaboratively discussed the content until we reached consensus about how to categorize and interpret the data. To ensure that our analysis was trustworthy, we used an audit trail to document analytic decisions and informally sought feedback from our participants to confirm our interpretations (Johnson et al., 2020). Transferability was addressed by providing thick descriptions of the inclusion and exclusion criteria, participant characteristics, study context, and participant reflections on their experiences (Younas et al., 2023). We adhered to the Consolidated Criteria for Reporting Qualitative Research (COREQ) reporting guidelines (Tong et al., 2007). The completed COREQ checklist can be found in the supplementary material.
Findings
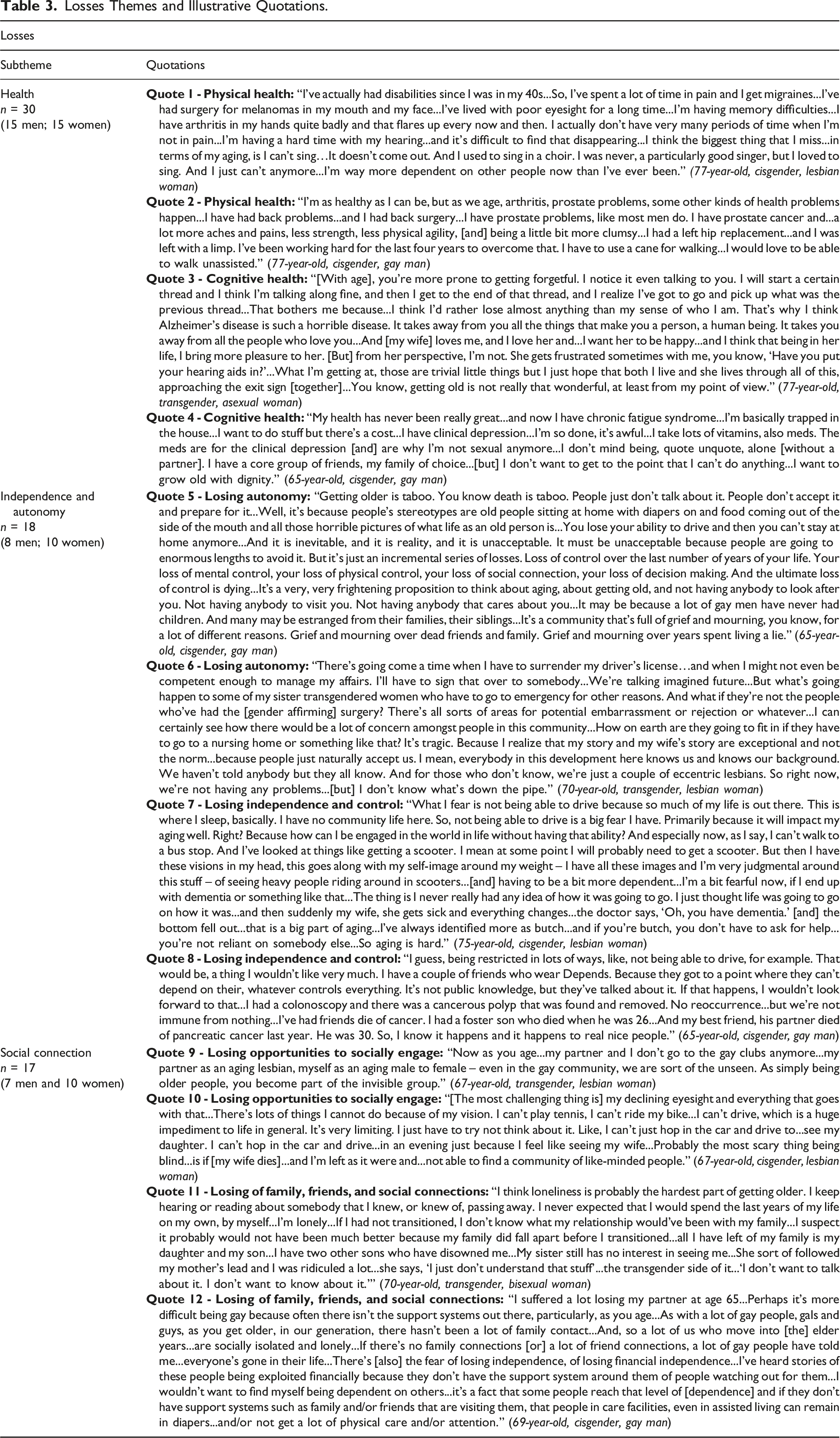
Losses Themes and Illustrative Quotations.
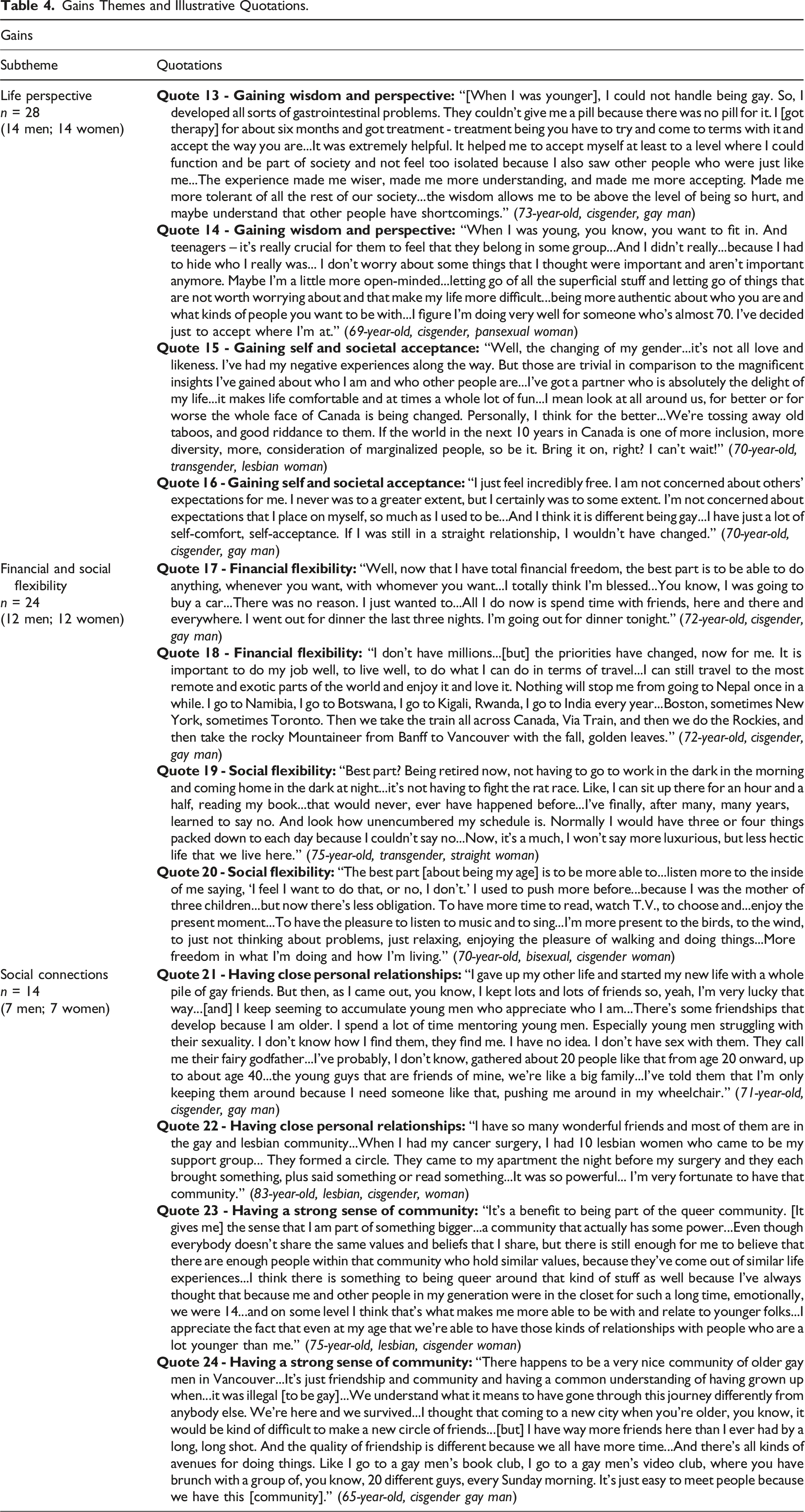
Gains Themes and Illustrative Quotations.
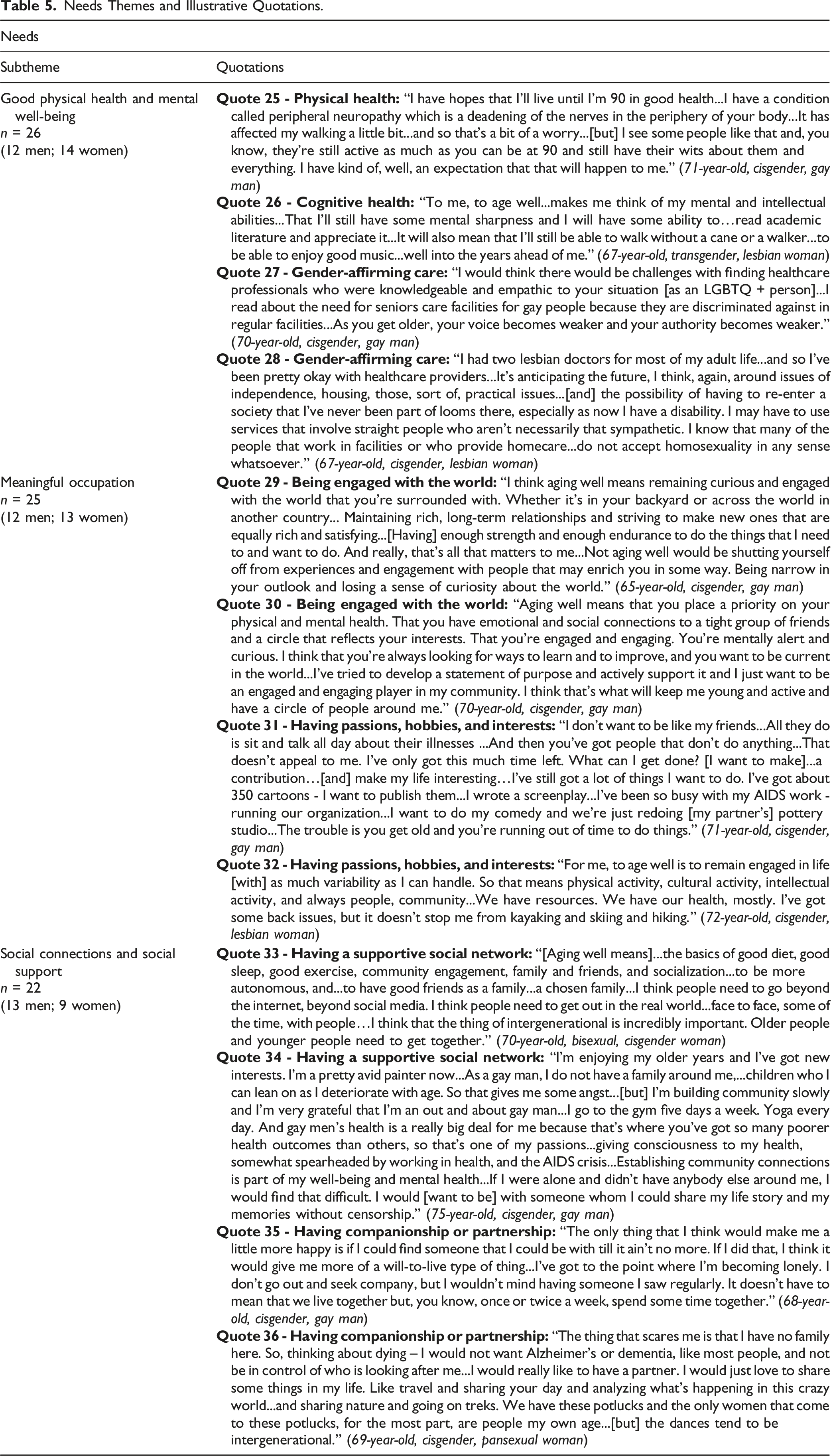
Needs Themes and Illustrative Quotations.
Theme 1: Older LGBTQ+ Persons’ Perceptions and Experiences of Aging-Related Losses
“As We Age...Health Problems Happen”: Physical and Cognitive Health Changes in Later Life
Most participants considered their health to be excellent, very good, or good, with relatively few rating their health as either fair or poor. All of our participants reported one or more physical and cognitive health issues, including cancer, cardiovascular disease, chronic respiratory diseases (e.g., asthma, chronic obstructive pulmonary disease, sleep apnea), HIV/AIDS, metabolic syndromes (i.e., diabetes, high blood pressure), musculoskeletal conditions (e.g., arthritis, sarcopenia), neurological conditions (e,g., Parkinson’s disease, stroke), and mental health issues (e.g., anxiety, depression, suicidal ideation). Many participants also described a variety of functional ability changes, including losses of strength and endurance, chronic fatigue, difficulties with mobility and balance, hearing and vision impairments, and/or chronic pain (Quotes 1–4, 7, 10). Some participants were particularly concerned about current and/or anticipated future cognitive losses, specifically declining memory and mental acuity, as well as the onset of dementia (Quotes 3, 5–8). Asserting that “health problems happen” (Quote 2) with age, the participants contended that their changing health was an inevitable part of growing older.
“An Incremental Series of Losses”: Losing Independence and Autonomy With Age
The participants often reflected on how their changing physical, cognitive, and functional health and abilities had negatively impacted their lives. Many participants described how their physical losses had diminished their abilities to walk, communicate with others, drive, complete household tasks, engage in hobbies, and connect with loved ones and the community more generally (Quotes 1–8, 10). Increasingly aware of their own mortality (Quotes 3, 5, 8), many participants feared that as they neared the end of their lives, they would lose their independence and become “reliant on somebody else” (Quote 7). A few participants also worried that their cognitive declines would heighten their vulnerability to “being exploited financially” (Quote 12) or mean that they “might not even be competent enough to manage [their own] affairs” (Quote 6). The participants perceived and experienced the physical realities of aging as “not really that wonderful” (Quote 3) but rather as “an incremental series of losses” (Quote 5) which undermined their sense of security and well-being and led to feelings of grief over their lost abilities.
“Everyone’s Gone”: Loneliness, Isolation, and Barriers to Social Engagement
Many participants reported a sense that “everyone’s gone” (Quote 12) as aging had been accompanied by a loss of social connections due to the passing of loved ones as well as barriers to social engagement, including the sense that they were invisible and unwelcome in LGBTQ+ spaces (Quotes 1, 4, 7, 9–10, 12). Reflecting on the loneliness that resulted from familial rejection (Quotes 5, 11, 12) as well as the loss of friends (Quotes 5, 8, 12) and partners (Quotes 5, 12, 35), participants stressed the importance of “family of choice” (Quote 4) and raised concerns about the lack of support systems in place for LGBTQ+ older adults who were grieving (Quote 12). Some further worried about the later life consequences of being socially isolated, or as one man put it: “It’s a very, very frightening proposition to think about aging, about getting old, and not having anybody to look after you” (Quote 5). As well as reporting health-related barriers (i.e., low energy, mobility challenges, cognitive declines) to maintaining social connections and participating in preferred activities (Quotes 1, 3, 4–5, 7, 10), participants highlighted a lack of older LGBTQ+ adult inclusive and gender-affirming social services, social supports, and activities that accommodated their unique needs as they aged (Quotes 6, 9, 12).
Theme 2: Older LGBTQ+ Persons’ Perceptions and Experiences of Aging-Related Gains
“Being More Authentic About Who You Are”: Gaining Wisdom and Self-Confidence
Most participants identified positive changes that they had experienced as they aged. Many spoke about having acquired wisdom (Quotes 13–14) or “magnificent insights” (Quote 15) into themselves over time, culminating in a greater sense of “self-comfort, self-acceptance” (Quote 16) of their LGBTQ+ identities in later life. As well as being less “concerned about others’ expectations” (Quote 16), the participants reflected on how changing social norms enabled them to be “incredibly free” (Quote 16) and “more authentic” (Quote 14), particularly as they no longer had to conceal their gender and sexual identities. They further expressed optimism as they envisioned a future society that was increasingly characterized by “inclusion,” “diversity,” and “consideration of marginalized people” (Quote 15).
“I Totally Think I’m Blessed”: Financial and Social Flexibility
Most participants highlighted that greater flexibility was an important benefit of growing older. Some defined this flexibility in terms of financial security and the freedom to engage in preferred pursuits (Quotes 17–20). With greater financial resources, some participants, most of whom were gay men, noted that they were more able to travel locally, nationally, and internationally (Quote 18). Many participants described how freedom from work- and family-related responsibilities meant they had more time to engage in hobbies and interests, such as reading, watching television, listening to music, singing, and spending quality time with family and friends (Quotes 17, 19–20). In this way, aging had fostered an augmented sense of contentment as participants appreciated the increased opportunities to live their lives as they pleased, or as one person stated “more freedom in what I’m doing and how I’m living” (Quote 20).
“I’m Very Fortunate to Have That Community”: Chosen Families and Community Support
Many participants emphasized that gaining a strong sense of community and supportive friendships was another important and positive development that had occurred as they openly embraced their LGBTQ+ identities (Quotes 21, 23–24). Pointing to the tight-knit bonds that they shared with other LGBTQ+ persons, the participants expressed appreciation for the ways that their communities had provided a safe, accepting, and supportive environment as they grew older (Quotes 21–24). The participants also valued their intergenerational relationships, specifically their friendships with younger LGBTQ+ persons (Quotes 21, 23). Having often lacked a support system in their own youths, they contended that mentoring younger LGBTQ+ persons (Quote 21) and building chosen families (Quotes 4, 21) were fundamental to their “sense [of being] part of something bigger” (Quote 23).
Theme 3: Older LGBTQ+ Persons’ Perceptions and Experiences of Aging-Related Needs
“It’s Anticipating the Future”: The Need for Inclusive and Gender-Affirming Care
Given their current and anticipated future health issues, many participants emphasized the importance of striving to manage, if not minimize, additional physical changes and functional declines (Quotes 2, 25–26). One participant summarized this sentiment in this way: “I want to grow old with dignity” (Quote 4). This meant not only being independent and autonomous for as long as possible (Quotes 25–26) but also being treated with respect and compassion (Quotes 6, 27–28). Many participants noted that they often felt simultaneously invisible and vulnerable to mistreatment and discrimination from health care providers due to their LGBTQ+ identities (Quotes 6, 27–28). They worried about their safety and marginalization in a system that lacked sufficient LGBTQ+ inclusive and gender-affirming health and long-term care.
“Remaining Engaged in Life”: The Importance of Meaningful Occupation
Most participants asserted that aging well was equated with remaining physically, socially, and intellectually engaged with the world through meaningful occupation (Quotes 29–32). They contended that having health and independence were essential to their ability to participate in their preferred activities (Quotes 29, 32). At the same time, they described how hobbies and interests fostered their health, well-being, and life satisfaction (Quotes 31–32). In other words, they suggested that physical health and social engagement were mutually influential. They stressed the importance of life-long learning as they emphasized the need to remain “curious and engaged” (Quote 29) and a desire to “learn and improve...[and] be current in the world” (Quote 30).
“Being a Part of a Community”: The Power of Social Connections
The final need that many participants identified as being essential for aging well was strong social connections, described as a “tight group of friends” (Quote 30), “rich, long-term relationships” (Quote 29), and “chosen family” (Quote 33). These social connections were positioned as increasingly important in the face of declines to health (Quotes 4, 36), anxieties over discrimination from health care providers (Quotes 27–28), familial rejection (Quotes 5, 11), and the absence of biological children (Quote 34). Participants contended that supportive social connections were essential to their “well-being and mental health” (Quote 34) and overall “will-to-live” (Quote 35). As such, many participants reported that they were actively and intentionally “building community” (Quote 34) to address their current and future social connection needs in a world that, while improving, was still not free of LGBTQ+ focused hostility and discrimination.
Discussion
Our study examined how older Canadian LGBTQ+ adults perceived and experienced aging. Similar to previous research (Adan et al., 2021; Boulé et al., 2020; Chiaranai et al., 2018; Fredriksen-Goldsen et al., 2018; Perone et al., 2020; Putney et al., 2016, 2018), our participants characterized later life as a time of progressive and inevitable health, independence, and relational losses juxtaposed against personal and social gains. Notably, two of the ways they felt that their lives had improved—being able to live authentically and becoming part of a chosen family and a visible LGBTQ+ community—were partially contingent upon and reflective of changing social norms, specifically the increasing societal acceptance of gender and sexually diverse identities, as well as legal human rights protections in Canada (Boulé et al., 2020; Government of Canada, 2022; Overby et al., 2011). In addition to the influence of changes to the broader Canadian social context and aligning with the Health Equity Promotion Model (Fredriksen-Goldsen et al., 2014), the participants’ perceptions and experiences of aging were shaped by intersections of different pathways to health, namely, those linked to biology, behavior, psychology, and social relationships. Thus, health and functional ability losses resulted in changes in activities, with concomitant deleterious effects on the participants’ sense of isolation and vulnerability as well as their abilities to maintain social connections. Rather than being unidirectional, these intersecting pathways were reciprocal in terms of their influence. For example, social losses such as the death of partners and close friends exacerbated participants’ feelings of loneliness, which, in turn, threatened their emotional and mental well-being. These intersecting pathways also had positive impacts as resilience factors such as the deepening of personal insights and self-confidence combined with the presence of LGBTQ+ inclusive relationships and communities enabled our participants to view their aging futures with increasing optimism, irrespective of the health and social losses they had already endured. In this way, our study adds to the Health Equity Promotion Model and gerontology literatures by illuminating how growing older in Canada as an LGBTQ+ person is shaped by intersecting pathways to health that are themselves embedded in cultural contexts and delimited by institutional policies, social norms and practices, as well as formal legislation.
However, despite their hopefulness for increasing societal acceptance and alongside Canada’s history of progressive legislation supporting LGBTQ+ rights, the participants raised concerns about the potential for discrimination and stigmatization, particularly in healthcare and long-term care settings. As such, our findings support previous calls by Caceres et al. (2020), Fredriksen-Goldsen et al. (2018), and Putney et al. (2018) for more LGBTQ+ inclusive, trauma-informed, and gender-affirming healthcare and social services. Our participants’ perceptions of heightened vulnerability in advanced age in these settings are further related to some of the barriers to social engagement and connection that they were experiencing. Like their cisgender and heterosexual counterparts (Cheng et al., 2022), our participants encountered health and mobility concerns as well as the loss of friends, families, and opportunities to connect with others. However, they also faced unique issues including familial rejection, continued societal invisibility, homophobic and transphobic prejudice, and a lack of inclusive health and social programming. As such, our findings add to the aging literature by underscoring the need for continued education and advocacy to counteract the discrimination and marginalization that older LGBTQ+ persons in Canada currently face and fear as they become increasingly vulnerable with age. Moreover, our study illustrates that not only are there intersections between pathways to health, as per the Health Equity Promotion Model, but also that vulnerabilities themselves intersect and amplify each other, particularly for older LGBTQ+ adults.
Unique to our study was the finding that some participants experienced increasing financial flexibility in later life, which directly contrasts with previous research with older LGBTQ+ adults (Burton et al., 2019; Fredriksen-Goldsen et al., 2018) but is akin to findings from studies with cisgender and heterosexual older adults (Betlej, 2023). We note that financial security was reported more often by gay men, which aligns with previous studies (Carpenter & Eppink, 2017). It is possible that this finding was a product of our sample, which was comprised primarily of middle- and upper-class individuals. It is further probable that unlike those in previous studies in other countries, our participants benefited from Canada’s universal health care system (Martin et al., 2018) and progressive legislation, which collectively may have protected them from some of the accumulated economic disadvantages reported by older LGBTQ+ persons in other countries (Burton et al., 2019; Fredriksen-Goldsen et al., 2018).
Our findings suggest the need for policy and practice changes to ensure that older Canadian LGBTQ+ adults are able to age with dignity. To begin, staff in clinical, mental health, social service, and long-term care settings require more training not only about the unique health issues facing older Canadian LGBTQ+ persons (e.g., living with HIV/AIDS, care for transgender persons who have and have not had gender-affirming surgeries) but also the health and social impacts of the discrimination and marginalization they have faced over their lifetimes (Cummings et al., 2021; QMUNITY, 2018). Similarly, to foster safety and inclusion, it will be important to achieve greater representation of LGBTQ+ identities through improved hiring practices that will lead to more diversity among health care and social service staff (Caceres et al., 2020; Furlotte et al., 2016). Given that many of our participants had been rejected by their biological kin, it is further essential that health care providers recognize and include chosen family members in health care decision-making, even in the absence of formally recognized partnerships (De Vries et al., 2019; Fredriksen-Goldsen et al., 2018). Health care and social service professionals and settings need to do more to both signal and actively demonstrate that they recognize and affirm gender and sexually diverse individuals so that older LGBTQ+ adults will be able to confidently access much-needed care and programming. Additionally, it will be important to develop programs that facilitate the development of meaningful occupations and social connections for and among LGBTQ+ older adults. This may include not only providing programming specific to gender and sexually diverse persons but also addressing transportation and other access issues. Whereas LGBTQ+ programs need to become more responsive to age diversity, aging-related services and programming needs to become more inclusive of and attentive to gender and sexual diversity (QMUNITY, 2018). These programs could not only ensure that older LGBTQ+ persons have the social supports and activities that will enhance their quality of life but could additionally become conduits of access to information about resources such as clinics that provide LGBTQ+ inclusive and gender-affirming care and counselors who are familiar with the challenges faced by older LGBTQ+ populations.
Limitations
There are several limitations to the study. Given our recruitment strategies and resultant use of a convenience sample, our participants were predominantly White, university-educated, and middle-class, disproportionately gay, and limited to English-speakers. Therefore, our participants did not fully represent the diversity of Canada’s older LGBTQ+ population and the losses, gains, and needs that were identified may not be reflective of the unique concerns and experiences of racialized, ethnically diverse, lower income, or otherwise marginalized older LGBTQ+ Canadians. We also acknowledge that despite our best efforts, the participants may not have felt comfortable fully disclosing their perceptions and experiences of aging as LGBTQ+ persons, particularly since many had endured stigmatization, prejudice, and discrimination in the past.
Conclusions
In summary, our study highlights that older Canadian LGBTQ+ persons perceived and experienced later life as a time of inevitable losses, valued gains, and unique needs. Our findings indicate that despite the steps that have been taken in Canada to address homophobia and transphobia through education, policy change, and progressive legislation (Government of Canada, 2022; Overby et al., 2011), there is an urgent and ongoing need to challenge and overcome the bigotry that continues to deny older LGBTQ+ adults the ability to age well and without fear of abuse and marginalization. Future research should further investigate the unique aging experiences and health and social care needs of older Canadian LGBTQ+ individuals who are racialized, ethnically diverse, of lower income, immigrants or refugees to Canada, as well as those who self-identify as gender non-binary and pansexual.
Supplemental Material
Supplemental Material - “I Want to Grow Older With Dignity”: Older LGBTQ+ Canadian Adults’ Perceptions and Experiences of Aging
Supplemental Material for “I Want to Grow Older With Dignity”: Older LGBTQ+ Canadian Adults’ Perceptions and Experiences of Aging by Laura Hurd and Lynda Y. K. Li in Journal of Applied Gerontology
Footnotes
Acknowledgments
The authors wish to thank all of the individuals who took part in the study and shared their time, experiences, and insights with us. They would also like to thank Mara Lewis and Raveena Mahal for their invaluable contributions to the project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada (Insight Grant# 435–2017-0165).
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.