
Abstract
Physical exercise interventions to prevent falls for older adults at risk of falling are widespread in many countries; however, there is insufficient knowledge of the impact of long-term exercise on the fall discriminating ability of existing fall-prediction indicators. This study measured physical and cognitive indicators of the fall risk, including the timed up and go (TUG), walking speed (WS), and plantar tactile threshold (PTT), in 124 community-dwelling older adults with care needs who were continuing an exercise program. Logistic regression analyses were used to determine factors associated with falls in the 87 participants who could adhere to the exercise continuously for 12 months. The PTT was significantly higher in fallers, while the TUG and WS did not differ significantly between fallers and non-fallers. The only index significantly associated with falls was the PTT (OR = 1.20). The fall identification ability was better for PTT (AUC = 0.63), whereas TUG (AUC = 0.57) and WS (AUC = 0.52) were lower than previously reported scores. In conclusion, long-term exercise was found to improve scores on the fallprediction indicators by physical performance, but to decrease their ability to identify future falls. PTT may complement the ability to identify falls in such elderly populations.
Introduction
Life expectancy continues to increase worldwide with both the total number and proportion of older adults growing rapidly. The global population of individuals aged 65 and older was 727 million in 2020 and is projected to reach over 1.5 billion in 2050 (Department of Economic and Social Affairs. Population Division, 2020). However, increased longevity does not necessarily equate to health in later life, with frailty increasingly being recognized as a serious public health concern (Adja et al., 2020). Accordingly, there is a pressing need for the development of comprehensive community-based approaches for preventing decline in older individuals.
The process of becoming frail or care-dependent has been shown to be delayed or partially reversed by the implementation of targeted interventions early in the process of functional decline (World Health Organization, 2017). In Japan, legislated projects for community-dwelling older adults have been provided by all municipal governments since 2006, aiming to prevent long-term care needs and provide support enabling independence in daily living as much as possible (Morikawa, 2014).
Fall prevention and management represents a critical global challenge to delay the process of the older population becoming frail or care-dependent. Exercise programs designed to prevent falls have shown high-certainty evidence of reducing the fall rate and the number of people experiencing falls among community-dwelling older adults (Sherrington et al., 2019). Early identification of people at risk of falling is critical for the appropriate and effective referral of older adults to fall prevention interventions (Lusardi et al., 2017; van Schooten et al., 2015).
Established methods for quantifying fall risk are fall history questions, self-report measures, motor performance-based measures, or a combination of measures (Lusardi et al., 2017). Meanwhile, the gait and balance performance measures have been found to be sensitive to changes in interventions for preventing falls (Montero-Odasso et al., 2023). Gait problems related to muscle weakness can be improved with muscle strengthening exercises, and deficits in balance can be improved with specific balance training (Rubenstein et al., 2001). However, fall prevention programs may improve only gait and balance performance index scores without reducing the frequency of fall events (Haines et al., 2008; Rubenstein & Josephson, 2006). It should be noted that the ability of these measures to distinguish fallers from non-fallers may be diminished in the older adult population participating in fall prevention programs. However, the identity of the test that is appropriately responsive to the fall risk in a population of older adults actively participating in routine physical exercise to prevent requiring long-term care or prevent falls remains unknown.
The purpose of this study was to identify valid predictive indicators of falls for community-dwelling older adults adhering to planned exercise programs for falls prevention. In particular, we focused on the fall predictive capability of measures of exercise performance with higher potential to improve performance from physical exercise interventions and measures of somatosensory function, which were known to be less affected by physical exercise interventions (Yagihashi et al., 2020).
Methods
Study Design and Setting
This prospective observational study of community-dwelling older adults was conducted per the principles of the Declaration of Helsinki, and the protocol was approved by the Medical Ethical Committee of the School of Nursing and Rehabilitation Sciences, Showa University (approval number: 378). The present study comprised community-dwelling older adults who regularly attended four long-term care day service facilities in Japan. These facilities, which are authorized by Japan’s long-term care insurance system, are available to those who have been certified as requiring long-term care or at risk of requiring such care. These four facilities provide service contents that are primarily aimed at ongoing programs to improve physical and mental functioning and prevent long-term care. The major part of the program was physical exercise including exercises in muscular strength, dynamic balance, mobility, and daily activities. The majority of older adults attended the center twice a week, staying for 3.5 hr and participating in a physical retraining program allocated to each individual. There is no limit to the period of facility use, and the program is revised every 3 months based on outcome measures of the exercise program.
Participants
The users of these facilities were directly invited to participate verbally, and all eligible prospective participants gave their written informed consent. One hundred twenty-three older eligible adults were included in the study. Our inclusion criteria were as follows: (1) age ≥ 65 years and (2) ability to walk independently inside the house. Our exclusion criteria during participant recruitment were as follows: (1) a diagnosis of cognitive impairment and (2) a diagnosis of impaired postural control due to vestibular impairment. Additionally, participants with MMSE scores of <23 were excluded at this point because of the reduced reliability of their interview responses. In this study, participants were required to be in continuous adherence to the physical exercise program for at least 12 months from the time of study entry. Therefore, those who did not continue to adhere to the exercise program for 12 months were finally excluded from the analysis. The sample size was estimated by multiplying the number of explanatory variables in the binomial logistic regression analysis by 10, with the number of explanatory variables set at 5. A minimum sample size of 100 participants was determined to be necessary for an adequate analysis.
Baseline Measures
Participants were assessed based on physical and psychological variables that have previously been reported to be effective in predicting falls when participants regularly visited their long-term care day service facility just after they participated in the study. Established physical indicators for predicting falls in this study included the strength of lower extremity muscles, ankle joint range of motion (ROM), hallux valgus severity, maximum walking speed, timed up and go (TUG), and single-leg stance with open eyes. The strength of the lower extremity was measured with a portable dynamometer for maximum voluntary muscle strength of knee extension, ankle joint dorsiflexion, and plantar toe flexion. All muscle strength values were normalized by body weight, and the averages of the left and right values were employed in the study analysis. The ROM of ankle joint dorsiflexion was measured in the sitting position for active ranges, and bilateral averages were used in the study analysis. Hallux valgus severity was measured using the Manchester scale (Menz et al., 2010), with the score on the most affected side being recorded. The maximum walking speed was calculated from the measured time required to pass a 5 m straight walking path with at least 2 m of acceleration and deceleration sections added at each end. The TUG test measured the time taken to get up from a chair, walk a fixed distance of 3 m, turn around, return to the chair, and sit down again. The chair had no armrests and the seat height was 40 cm. The maximum walking speed and the TUG were measured twice, and the faster record was adopted in the analysis. Moreover, participants were asked to stand on a single leg without assistance, and they were timed from the moment they lifted their legs off the floor to the moment they placed the same legs on the floor again. This test was performed once per side with open eyes, and the average of both sides was employed in the analysis.
In addition, cutaneous sensory thresholds on plantar surfaces were measured as a physical variable that was less sensitive to the effects of the exercise program. A newly developed plantar tactile threshold (PTT) testing device (Sato et al., 2015) was used to measure PTTs at the bilateral first metatarsal heads and heels. The testing stimulus of this device employs an automatic single-shear sliding action with a range of 5 to 2,000 µm applied horizontally to the plantar surface through a small mechanical probe located in the center of a measurement platform. The sequence of test stimuli used in this study (shown in Table 1) had an exponentially increasing series, according to Weber-Fechner’s law (Hecht, 1924). Thresholds (µm) were divided by the minimum stimulus intensity of the device and then transformed by the common logarithm to a linear threshold (dB). The lowest thresholds of the four measured sites were employed in the analysis.
Slide Length and Speed in a 14-Step Gradual Increase Sequence of the Test Stimuli for Measuring Plantar Tactile Thresholds Employed in This Study (Constant Time Stimuli Setting: 50 m).

Cognitive and executive functional tests as psychological functions related to falls were performed using the Mini-Mental State Examination (MMSE) and the Trail Making Test part A (TMT-A) (Reitan, 1958). Data on date of birth, gender, medical history, frequency of service use per week, history of service use, and level of certified need for care under the Japanese long-term care insurance system (Tsutsui & Muramatsu, 2005) were abstracted from the care records of each service facility to collect data for all participants. Participants were interviewed about whether they had had one or more falls in the 12 months prior to participating in the study, and in addition, height and weight data were collected.
Prospective Fall Monitoring
Fall events for each participant during the 12-month follow-up period were identified from daily monitoring documentation in day service records. Day service staff always asked participants about the occurrence of falls since the previous service use and documented responses in the day service record. To compensate for the omission of documentation regarding fall events in the day service records, participants were questioned every 6 months regarding the occurrence fall-related events. Participants who experienced one or more falls during the follow-up period were classified as prospective fallers, with others classified as prospective non-fallers.
Statistical Analysis
Descriptive statistics for the fallers and non-fallers were expressed as the mean ± standard deviation for continuous variables or as the percentage for categorical variables. The categorical variables of gender, level of care needs, and severity of hallux valgus were compared between fallers and non-fallers using chi-squared or Fisher’s exact tests. Continuous variables were compared by Student’s unpaired t-test or Wilcoxon rank-sum test according to the homoscedasticity and normality of the two groups.
To identify measured items associated with future falls, a stepwise forward selection procedure was conducted to select variables worthy for model fitting, with fallers/non-fallers as a dependent variable and measured values of physical indicators and cognitive/executive functions as independent variables (predictor variables). Eleven independent variables were entered at this step, with physical measures including the strength of knee extension, ankle dorsiflexion, toe flexion, ROM of ankle joint, severity of hallux valgus, PTT, maximum walking speed, single-leg stance, and TUG, and with cognitive/executive measures (including MMSE and TMT-A). The variables selected in that procedure were entered into a logistic regression model to estimate the odds ratios for each item. Odds ratios for the same items were additionally estimated in a logistic regression analysis to determine the effect of the presence of medical history that may cause neurological disorders (i.e., cerebrovascular disease, diabetes, and spinal cord disease) using forced entry of these data into the analysis. Potential multicollinearity between the measured items was evaluated using the variance inflation factor (VIF).
In addition, the abilities to predict future falls for variables found to be strongly associated with falls was evaluated by the optimal cut-off value, sensitivity, specificity, area under the curve (AUC) of the receiver operating characteristic (ROC) curve, positive predictive value (PPV), negative predictive value (NPV), and Youden Index. The threshold for statistical significance was set at p < .05. Statistical analyses were performed using JMP Pro 14.0 (SAS Institute Inc, Cary, NC, USA).
Results
Four participants who withdrew their consent and nine participants who were identified to have MMSE scores of less than 23 after enrollment were excluded from the study. A further 23 participants who dropped out of the day service during the follow-up period were also excluded. Descriptive characteristics of the 87 participants included in the study analysis as older adults who continued to adhere to a regularly scheduled exercise program are summarized in Table 2. The percentage of participants with falls during the 12-month follow-up period and with a history of falls in the 12 months prior to study entry was 50.6% and 49.4%, respectively. Fallers had a significantly larger ratio of males (p = .034) and were significantly greater history of falls in the past 12 months prior to study entry than non-fallers (p = .001). Fallers had higher PTT (that means reduced sensation) than non-fallers (p = .046). No significant differences in physical and psychological measures were observed between prospective fallers and non-fallers other than PTT values. The female percentage and mean age of the dropouts were 75.0% and 83.0 ± 6.3 years, respectively, with both parameters being similar to those of our study population. Other demographic data for the dropouts were not collected. Most of the 23 participants who dropped out of day service facilities were hospitalized, while the other reasons were physical condition deterioration and relocation.
Demographic Factors and Measured Variables of Participants.
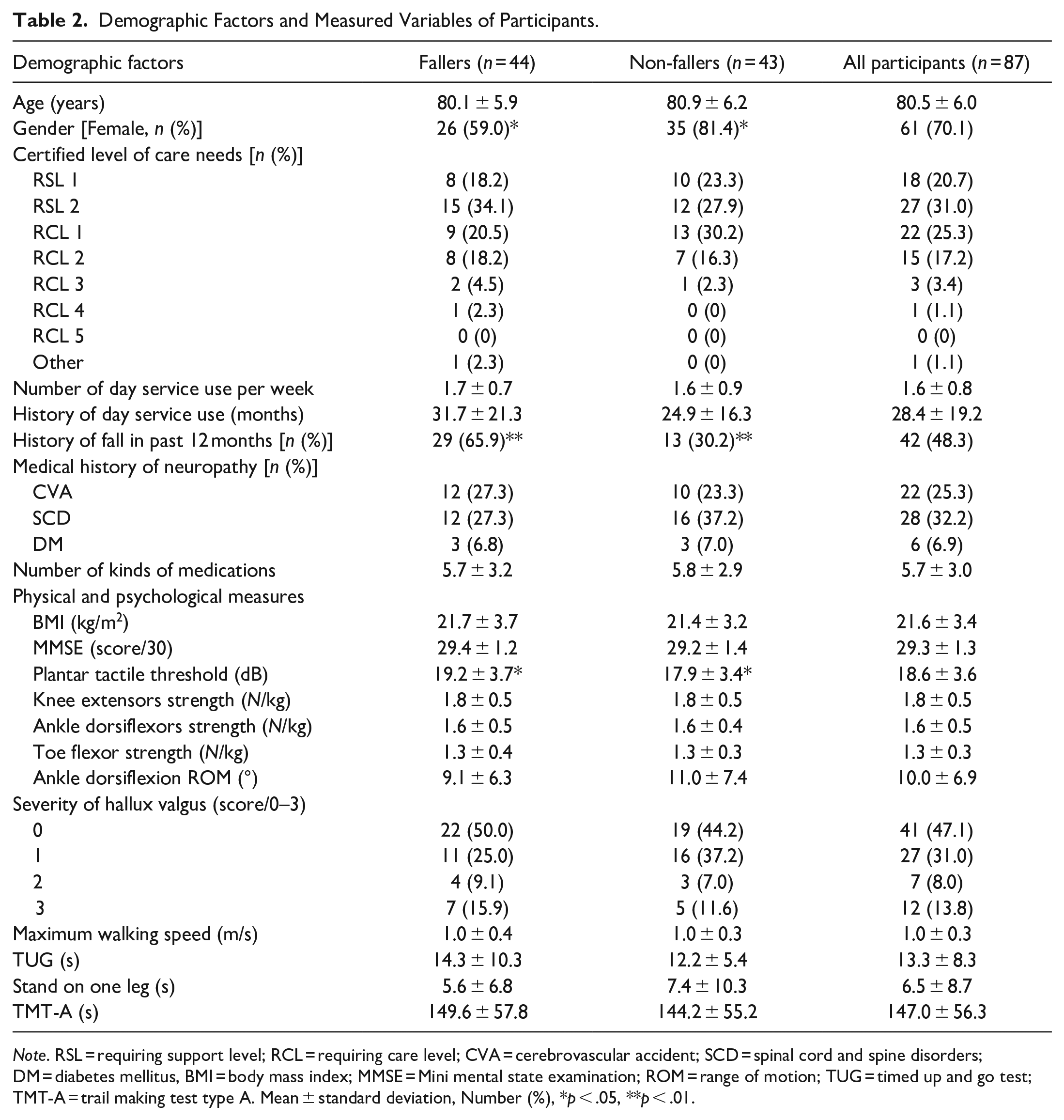
Note. RSL = requiring support level; RCL = requiring care level; CVA = cerebrovascular accident; SCD = spinal cord and spine disorders; DM = diabetes mellitus, BMI = body mass index; MMSE = Mini mental state examination; ROM = range of motion; TUG = timed up and go test; TMT-A = trail making test type A. Mean ± standard deviation, Number (%), *p < .05, **p < .01.
Then, to identify physical and psychological factors that can predict future fall events in an older adult population currently participating in physical exercise routinely, a stepwise procedure was conducted for 11 measured values of physical and cognitive/executive function. As a result, three items were selected with fallers/non-fallers as a dependent variable: PTT, MMSE, and ROM of ankle dorsiflexion. Table 3 shows the results of a logistic regression analysis with those three items as inputs for the independent variables. PTT was the only item that demonstrated a significant association with future falls which occurred during the 12-month follow-up period. Odds ratios and confidence intervals for PTT, MMSE, and ROM of ankle dorsiflexion adjusted for a history of cerebrovascular disease, diabetes, and spinal cord disease were similar to the unadjusted results. The VIF as an indicator of potential multicollinearity among the measured items was 3.19, which is considered an acceptable value (O’brien, 2007).
Significant Physical and Psychological Indicators for Falls Obtained From Stepwise Multivariate Logistic Regression Analysis.

Note. OR = odds ratio; CI = 95% confidence interval, PTT = plantar tactile threshold; MMSE = mini mental state examination; ROM = range of motion.
The results of the optimal cutoff value, sensitivity, specificity, PPV, NPV, AUC, and maximum Youden index of PTT for predicting falls during the 12-month follow-up period are shown in Table 4. Furthermore, using the two items of sex and history of falls in the past year (for which significant differences were identified between fallers and non-fallers), we defined predictive models consisting of sex and PTT and consisting of fall history and PTT as Model 1 and Model 2, respectively. The measured values of TUG and walking speed were independently highlighted as previously established indicators of fall prediction. The results of calculating the optimal cutoff values, sensitivity, specificity, PPV, NPV, AUC, and maximum Youden index for the four models including the two indicators are also shown in Table 4. The AUC of the ROC curve for PTT in older adults who regularly participate in physical exercise was 0.63. The AUCs for Models 1 and Model 2 were 0.66 and 0.70, respectively, which were superior to those of just only PTT. The sensitivity of the PTT measures alone was the highest at 0.80. Model 2 had the best combination of sensitivity and specificity, reflecting higher Youden index values. In contrast, the AUCs for the TUG and walking speed measures processed separately had relatively low values of 0.57 and 0.52, respectively.
Summary of Predictive Accuracy Statistics for Fall Risk Assessment Using Plantar Tactile Thresholds.

Note. Mean (95% confidence interval), PPT = plantar tactile threshold; Model 1 = PPT and gender; Model 2 = PPT and history of fall; TUG = timed up and go; PPV = positive predictive value; NPV = negative predictive value; AUC = area under the curve.
Discussion
The present study identified independent predictors of falls among community-dwelling older adults with ongoing care needs participating in regular exercise programs. The results demonstrated that PTT was more associated with falls risk than physical and cognitive variables commonly used in fall risk assessments used in elderly populations and remained an independent predictor of falls risk after adjustment for the presence of neurological disorders.
The TUG test and gait speed were reported to be effective predictors of falls in a frail and elderly population (Montero-Odasso et al., 2023); however, both measures had poor ability to predict falls in frail and elderly individuals who participated in a regular exercise program. The cutoff point for TUG as a predictor of falls in older adults is reported to be <13.5 s (Shumway-Cook et al., 2000), and this value is <15 s in frail persons (Nordin et al., 2008; Shimada et al., 2009). The frail elderly participants in the study, who were more or less in need of care, had better TUG records of 12.2 s on average for non-fallers and 14.3 s on average for fallers. Also for the walking speed, various cutoff values for predicting falls have been reported, including <1, <0.8, and <0.6 m/s (Beck Jepsen et al., 2022). The results of the walking speed in this study were also better than those reported in previous studies (1.0 m/s on average in fallers and non-fallers). The ability to walk and balance in older adults can be improved through certain balance training programs (Rubenstein et al., 2001). The participants of this study have been regularly attending a daycare facility and exercising continuously for more than 2 years on average. An exercise program focused primarily on fall prevention may have improved the TUG and walking speed of this study’s participants who were frail individuals with an average of 80 years and a fall rate of about 50%.
The predictive ability of PTT, the only variable among the 11 physical and psychological indicators measured in this study that met the p < .05 requirement for predicting future falls, was evaluated with a numerical value of 0.63 on the AUC. In addition, the AUCs for Model 1 and Model 2 were 0.66 and 0.71, respectively. A recent systematic review estimated the AUC values of future falls for the TUG and walking speed to be 0.54 to 0.73 and 0.54 to 0.77, respectively. Those for the Berg balance scale, Tinetti test, and Functional Reach test, which are commonly used to determine fall risk, were also in approximately the same range (Meekes et al., 2021). Comparisons of our findings with the results of those previous studies provide an interpretation that the predictive ability of the PTT to predict falls is an available value. In contrast, the AUCs for the TUG and walking speed in this study were 0.57 and 0.52, respectively, which are poor values at or below the lower end of the estimated range. The results of the study suggest that exercise intervention programs to prevent frailty may reduce the ability of physical indicators such as TUG and walking speed to distinguish fallers from non-fallers for older adults.
Several previous studies have reported a relationship between falls risk and PTT in older adults. It has been suggested that somatosensory information from the lower limb appears to play a dominant role in the task of maintaining an upright standing posture in humans (Lord et al., 1991). In recent years, evidence has been accumulated suggesting that cutaneous receptors on the sole may act as a source of essential somatosensory information. The sole is the only surface in contact with the ground during bipedal walking and perceives forces from the ground that contribute to the control of balance and maintaining an upright posture. Diminished cutaneous sensation in the plantar surface of the foot results in postural instability (Hafström, 2018; Peters et al., 2016), altered stepping reactions to unpredictable perturbations (Meyer et al., 2004; Perry et al., 2000), and changes in foot pressure distribution during gait (Nurse & Nigg, 2001).
Increased PTT often occurs in combination with other functional impairments. Elderly populations at high risk of falling often include individuals with widespread impairment of motor and sensory function in the lower extremities due to diseases such as cerebrovascular disease or peripheral neuropathy. Among the participants in the present study, 42.5% had a diagnosis of cerebrovascular disease, diabetes, or scoliosis (20 fallers and 17 non-fallers). For these participants, extensive and combined motor and sensory impairments in peripheral regions may contribute to fall events. Even after adjusting for the presence of these neurological disorders, there was no clear difference in the odds ratio of the PTT explaining future falls. These results suggest that PTT of itself is an independent risk factor for future falls, even in those with a prevalence of these neurological disorders. Further, increased PTT may by representative of the influence of neuropathy on falls risk in individuals with extensive peripheral nerve dysfunction.
There were several limitations in this study. First, the method of fall monitoring in this study could be criticized as not accurately measuring the incidence of falls. As the day service records might not contain complete information on fall-related events, we interviewed the participants to identify self-reported falls every 6 months. The sensitivity and specificity of recalling at least one fall in the past 12 months were reported to be 87% and 93%, respectively, and especially with MMSE scores of 27 or higher, the sensitivity increases to 91% (Ganz et al., 2005). The mean MMSE score of our participants exceeded 29 points; however, the possibility that under- or overestimation of fall risk may influence the study results cannot be excluded.
Second, as noted above, if the PTT reduction is a consequence of peripheral neuropathy in the lower legs and feet, then its association with falls may have resulted from extensive somatosensory and motor dysfunction in the peripheral regions. The percentage of people aged 75 years or older with a severe decline in any of the plantar sense, toe position sense, vibration sense of the internal capsule, and triceps tendon reflexes reaches nearly 40% (Mold et al., 2004). Although PTTs can be potentially effective variables for detecting the prevalence of neuropathy, and since no variables related to peripheral neuropathy except the PTT were measured in this study, the relationship between the decline of other sensorimotor functions and falls cannot be directly mentioned.
Furthermore, because this study did not control for the duration of the physical exercise intervention, it is not possible to directly address the time sequence of the exercise intervention’s effect for fall predictors. Given the results of this study, further studies that increase the sample size to segment into groups by intervention period or that are inclusive of participants at the beginning of the exercise intervention appear to be worthwhile. The demand for reliable prediction of future falls among older adults under prolonged exercise intervention will grow when policies to actively prevent care-requiring conditions spread across countries in the future. Further research is warranted to determine the association between plantar tactile thresholds and future falls in older adults with various health statuses and states of intervention.
Conclusions
In summary, the continuous provision of exercise programs for fall prevention to older adults improved the results of existing physical indicators for fall prediction; however, it reduced their ability to predict falls. In contrast, the PTT was identified as a useful complementary index of the fall predictive ability for older adults who adhere to a long-term physical exercise program. Updated findings on the efficacy of fall prediction indicators will be required as the system of policies develops to provide physical activity interventions to a larger number of older adults.
Footnotes
Acknowledgements
We thank Shinichi Yoshimura for technical support of the newly developed plantar tactile threshold testing device.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Japan Society for the Promotion of Science (JSPS) KAKENHI Grant Numbers JP15K01339, JP18K12161, and JP22H03995. The funding agency had no role in design of the study, data collection and analysis, interpretation of results, and writing the manuscript.
Ethical Approval
The Medical Ethical Committee of the School of Nursing and Rehabilitation Sciences, Showa University, approved the protocol (No. 378).