
Abstract
Food insecurity impacts the lives of 7.6 million U.S. adults aged 60 and older and is linked to numerous life challenges. This study examined the nature of food insecurity among community-based participants ≥65 years in a north Florida county and conceptualized food insecurity as encompassing the lack of food and individual adaptability. Thus, food insecurity was measured using three dependent variables: (1) worrying that food would run out, (2) cutting meal size or skipping meals, and (3) food not lasting. Logistic regression revealed that older participants, those with better-perceived health status, and those who were confident that they could find solutions to their problems had lower odds of reporting food insecurity. However, respondents who lived in low-income, low-access zip codes and those who received food assistance were more likely to report food insecurity. To improve outcomes and reduce healthcare disparities, solutions to food insecurity must vary in focus and approach.
Introduction
The prevalence of food insecurity is a critical public health concern in the United States (US) and is associated with numerous poor outcomes. In 2021, 7.6 million adults 60 and older were food insecure, lacking sufficient access to food resources to support an active, healthy lifestyle (Coleman-Jensen et al., 2013; Ziliak & Gundersen, 2023; Ziliak et al., 2022). Melani et al. (2020) found that 42% of adults ≥65 reported having to reduce the quality or quantity of food consumed in their households due to scarce resources. Saint Ville et al. (2019) and Coleman-Jensen et al. (2021) also found that as food insecurity increases, it is common for individuals to describe eating smaller portions, skipping meals, or going without food and not having sufficient resources to buy more food. Hake et al. (2023) document that 8 out of 10 high food insecurity counties are in the Southern US. Florida ranked eighth on the list of top 10 states with the highest rates of senior food insecurity in 2021 (Ziliak & Gundersen, 2023). Ziliak and Gundersen (2023), also reported a 35% increase in food insecurity among seniors between 2001 and 2021 amid a 40% growth in the US senior population of the same period. Among older adults in Florida, food insecurity increased from 11.3% (2015–2016) to 13% (2018–2019) (FLHealthCHARTS, 2019). In 2019, 16.4% of the Leon County population was food insecure, higher than the state average of 12% (FLHealthCHARTS, 2019). Considering the projected 50% increase in the adult US population ≥65 years by 2030 (Kim et al., 2021), food insecurity among older adults becomes an even more critical public health issue.
This study explores the nature of food insecurity among a predominately African-American population of older adults within Leon County, Florida. It examines the relationship of food insecurity to demographic, personal characteristics, and external factors. This study’s hypotheses are (1) an inverse relationship between food insecurity and socioeconomic status exists; (2) a correlation would be found between accessing community food resources, higher levels of self-efficacy, and food insecurity.
Background
The extant literature demonstrates an association between food insecurity and several demographic and individual characteristics. Coleman-Jensen et al. (2013) indicate that people of color are more susceptible to experiencing food insecurity, mainly Black and Hispanic seniors. Findings by Phojanakong et al. (2019) (p. 2) reported that “in 2018, 21.2% of African American or Black households and 16.2% of Hispanic households reported food insecurity, compared to 8.1% of white households.” Ziliak and Gundersen (2023) found that food insecurity among older adults remains higher than before the 2007 “great recession.” Jackson et al. (2019) found that compared to food-secure participants, low-income older adults aged 60 and above were more likely to experience marginal, low, or very low food security.
Regarding gender, families with women as the head of the household had increased odds of food insecurity (Facchini et al., 2014). Socioeconomic factors are similarly linked to food insecurity. For example, Facchini et al. (2014) and Mavegam Tango Assoumou et al. (2023) report that low maternal education, family income, and receipt of income assistance positively correlated with food insecurity.
Given the association between nutrition and health, as expected, food insecurity is associated with greater impairment as measured by activities of daily living (Gundersen & Ziliak, 2015) and poorer health status (Seligman et al., 2010). For example, the Tucher et al. (2021) study revealed that food-insecure older adults had higher rates of multiple comorbidities, depression, and frailty.
Research also documents that food insecurity is negatively associated with the ability to find solutions to problems (Schwarzer & Fuchs, 1996), which Bandura (1977) defined as self-efficacy. When self-efficacy is high, individuals believe they can execute behaviors necessary to achieve their goals. When setbacks occur, they will recover quickly (Schwarzer & Fuchs, 1996). Thus, these individuals may be better equipped to solve the dilemma of food insecurity than individuals with lower self-efficacy.
The guiding principles underpinning this study are from the Health Belief Model (HBM) (Conner & Norman, 1996; Rosenstock, 1974), which is used to explain health-related behaviors (Glanz et al., 2008). According to Glanz et al. (2008), HBM contains several primary concepts that predict why people will act to prevent, screen for, or control illness conditions; these include susceptibility, seriousness, benefits, and barriers to a behavior, cues to action, and self-efficacy.
Perceived susceptibility refers to beliefs about the likelihood of getting a disease or condition; perceived severity is individuals’ feelings about the seriousness of contracting an illness or leaving it untreated, including medical, clinical, and social consequences (Glanz et al., 2008). The combination of susceptibility and severity has been labeled as a perceived threat. Even if a person perceives personal susceptibility to a serious health condition, whether this perception leads to behavior change will be influenced by the person’s beliefs regarding the perceived benefits of various actions for reducing the threat (Glanz et al., 2008). Thus, how an individual experiences food insecurity is associated with personal characteristics (e.g., demographics, perceived threat, self-reported health status, self-efficacy) and external factors, for example, transportation access to healthy foods, income, and affordability.
In our exploratory analysis, we used the HBM not to prove the theory, but to examine components which significantly predict behavior in relation to food insecurity. As such, the regression analysis examines perceived severity and perceived susceptibility, measured by participants’ beliefs and opinions. We anticipated associations between the beliefs of susceptibility and severity and likelihood of behaviors. Participants who perceive themselves to be at one or more levels of food insecurity will be more likely to act to alleviate the perceived threat by accessing food assistance and exhibiting higher levels of self-efficacy by finding solutions to problems, thereby lessening their vulnerability to food insecurity.
Methods
This study uses purposive sampling to explore the factors associated with food insecurity within a population of older adults in Leon County, Florida. Researchers obtained a list of food distribution sites in the county from the food bank covering the Big Bend region of Florida. Participants were recruited from locations on the list, including churches, independent living housing for older adults, the eldercare service center, a city senior center, and other community-based organizations. Surveys were also collected in individual neighborhoods and among attendees at a popular local festival. Participants had the option of completing paper surveys or electronic surveys via Qualtrics. Each participant who completed the survey received a $10 grocery store gift card. Consent was obtained from all subjects involved in the study. Excluded were persons not living in Leon County and persons under the age of 65 years. The project received institutional review board approval.
To ensure that the data collection included individuals who potentially experience food insecurity, the researchers targeted adults residing in five Leon County zip codes: 32301, 32303, 32304, 32305, and 32310. These zip codes were selected based on 2019 internal data from the county health department, which indicated that individuals living in those zip codes are at the greatest risk for food insecurity. The survey instrument was derived from three sources: (1) the USDA Adult Food Security Module 2012 (USDA Economic Research Service, 2022), (2) the USDA Food Security Supplement December 2020 version (USDA Economic Research Service, 2023), and (3) the CDC Health-Related Quality of Life, (HRQOL) module (CDC & HRQOL, 2019). The instrument consisted of 28 quantitative questions.
The study sample size was 464 respondents. The data were reviewed for completeness and to address errors. For example, errors we identified were incorrect zip codes where numbers were transposed, surveys completed by persons under age 65, etc. In cases where we could ascertain the correct answer, the data was corrected; however, for those who failed to provide an answer or those whose correct answer could not be ascertained, their entire response was thrown out. The final sample was 355.
Prevalence of Food Insecurity
This study conceptualizes food insecurity as multi-dimensional and encompasses the social and economic context that may lead to the lack of food and how individuals adapt. Thus, food insecurity was measured using three questions about behaviors and experiences associated with difficulty meeting food needs. Adapted from the typology used by the USDA to categorize the continuum of food insecurity (USDA Economic Research Service, 2022a, 2022b), our dependent variables represent two levels of food insecurity. Households with the least severe food insecurity were measured by our variable, “I worried whether my food would run out before I got money to buy more in the last 12 months.” Respondents could indicate if the statement was always true, sometimes true, or never true. Midrange food insecurity was measured by our variable “In the last 12 months, did you ever cut the size of your meals or skip meals because there was not enough money for food?” for which respondents could answer yes/no, and “The food that I bought just did not last, and I did not have money to get more in the last 12 months,” for which response choices were always true, sometimes true, or never true. The responses to these questions were dichotomized to be true (coded as “one”) or never true (coded as “zero). Yes and no responses were coded as “one” and “zero” for no.
In this study, demographic characteristics, quality of life, food quality, and self-efficacy represent the constructs related to our independent variables.
Demographic Characteristics
Seven questions measured demographic characteristics: zip code, race, gender, age, education, retirement status, and receiving food assistance. Zip codes were dichotomized into low-income/low-access (LILA), coded as “one” versus all other zip codes (coded as “zero”). The choices for race were American Indian, Black/African American, Native Hawaiian, white, and other. Race was dichotomized into Black/African American (coded as “one”) versus all other races (coded as “zero”). Gender was dichotomized as female (coded as “one”) versus male (coded as “zero”). Age was measured as a continuous variable. For education, respondents could indicate the level of education attained along an eight-level continuum, which started at eighth grade or less and ended at the doctoral level. Respondents were asked, “Are you retired?”. The response choices were “Yes, fully retired,” “Yes, but I work part-time,” “No, I am employed full-time,” “No, I am employed part-time,” and “I have never worked.” This variable was dichotomized as “Yes, I am working” (coded as “one”) or “No, I am not working, or I have never worked” (coded as “zero”). The final measure, food assistance, was determined by the question, “Please indicate what food assistance you receive, if any.” The choices were “SNAP” (Supplemental Nutrition Assistance Program), “Food pantries/community food giveaways,” “Other,” or “None.” This variable was dichotomized as receiving food assistance (coded as “one”) or not receiving assistance (coded as “zero”).
Quality of Life
Two questions were included in the model to explore the association between health and food insecurity: perceived health status and physical limitations. For perceived health status, respondents could indicate they categorized their health status as poor (coded as “one”), fair (coded as “two”), good (coded as “three”), and excellent (coded as “four”). Respondents were asked if they had a physical limitation; response choices were “yes” and “no.”
Food Quality
The respondents’ satisfaction with the cost of fresh fruits and vegetables operationalized food quality. The five-level Likert scale responses allowed respondents to indicate very unsatisfied, coded as “one,” to very satisfied, coded as “five.”
Self-efficacy
Finally, respondents were asked to what extent they agreed with the statement, “I can find solutions to most problems.” The response choices were strongly disagreed (coded as “one”) to strongly agree (coded as “five”).
Analysis
This cross-sectional study used chi-square analysis and logistic regression in Stata version 16 (StataCorp, 2019). We conducted chi-square analyses comparing each dependent variable to LILA to assess our primary hypothesis of a relationship between food insecurity and socioeconomic status. Logistic regression models that provide odds ratios for each dependent variable were developed to test our secondary hypothesis of food insecurity and its relationship to personal and external factors.
Results
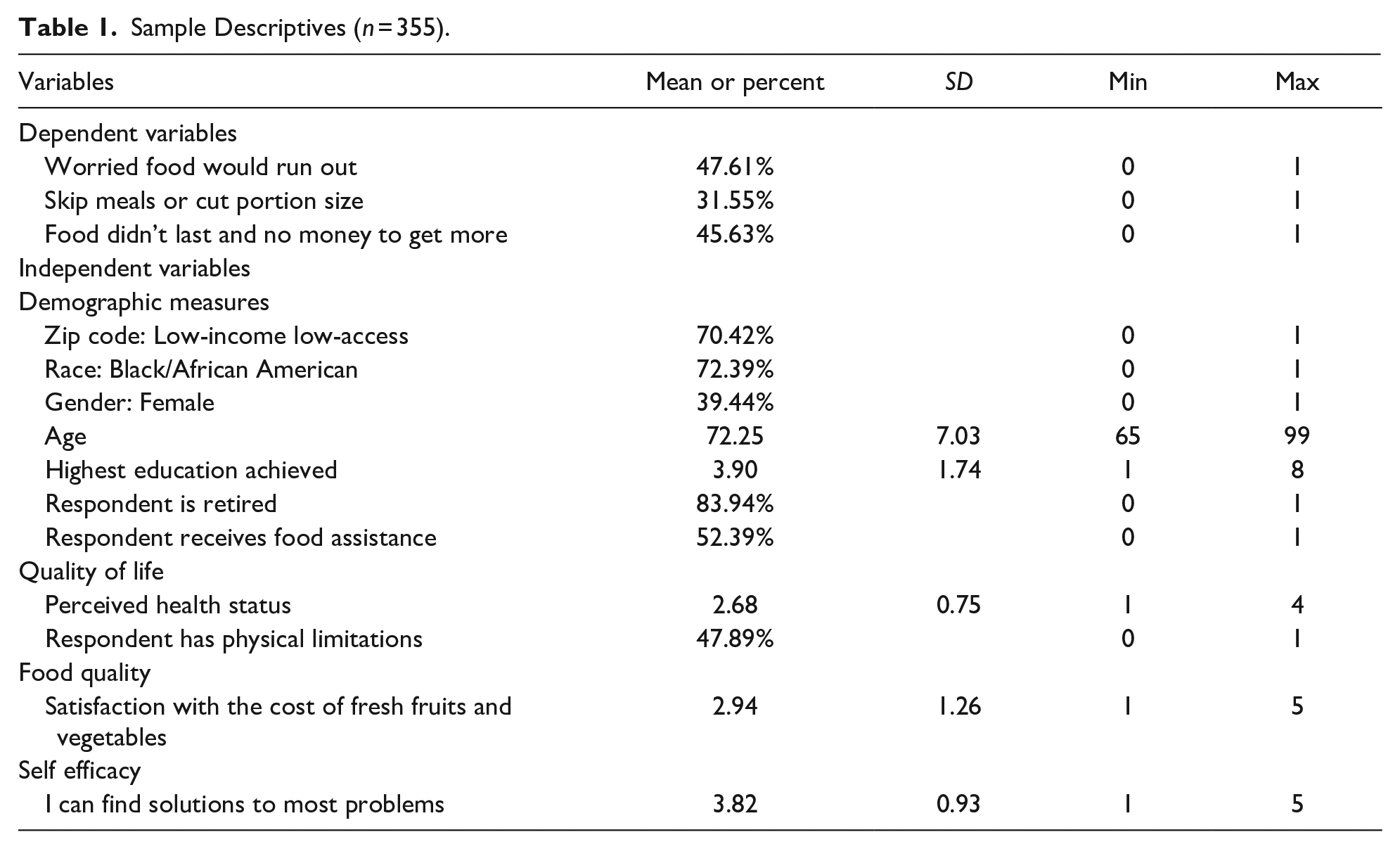
Table 1 provides the sample descriptives. Approximately 48% of the sample reported worrying that their food would run out, compared to 32% who said they skipped meals or cut portions and 46% who said that food didn’t last and they had no money to purchase more. Most respondents lived in low-income, low-access zip codes (70%), were Black/African American (72%), were retired (84%), and 52% received food assistance.
Sample Descriptives (n = 355).
Chi-square tests of independence were performed to examine associations between the three dependent variables and residence in LILA zip codes. Significance was found at each level of food insecurity: worried food would run out (χ2 = 12.1765 p = .000), skipping meals (χ2 = 5.2163 p = .022), and running out of food and having no money to purchase more [χ2 = 13.8078 p = .000].
As shown in Table 2, Model 1, as respondents increased in age, they were less likely to report worrying about running out of food (OR = .92, 95% CI [0.89, 0.96]). Those who received food assistance (OR = 2.72, 95% CI [1.62, 4.58]) were more likely to report being worried that their food would run out than those who did not receive it. Additionally, those who had poorer perceived health status (OR = 0.61, 95% CI [0.42, 0.88]) and those who were less confident about their ability to find solutions to their problems (OR = 0.68, 95% CI [0.52, 0.90]) were more likely to report concerns that their food would run out as compared to those with better health status and those who felt empowered to find solutions to problems.
Logistic Regression Analysis (n = 355).

Note. Model 1: Worried food would run out; Model 2: Skip meals or cut portion size; Model 3: Food did not last and no money to get more. OR = odds ratio; CI = confidence intervals; Bold text = significant findings.
Similar to Model 1, Model 2 shows a negative association between age and the odds of reporting the need to cut meal size or skipping meals (OR = 0.94, 95% CI [0.91, 0.98]). However, those who received food assistance (OR = 2.40, 95% CI [1.39, 4.14]) were more likely to report having cut or skipped meals than those who did not receive food assistance. Finally, those who reported satisfaction with fresh fruits and vegetables (OR = 0.80, 95% CI [0.65, 0.98]) were less likely to report they had to cut the size of their meals or skip meals compared to those who were unsatisfied with fresh produce.
The final model in Table 2, Model 3, revealed that persons who resided in LILA zip codes (OR = 1.79, 95% CI [1.04, 3.08]) were likely to report experiencing food not lasting and not having money to get more, similar to the association found in the chi-square. Age has an inverse relationship (OR = 0.94, 95% CI [0.91, 0.98]) with experiencing a lack of food and having no funds to purchase. Conversely, respondents who received food assistance (OR = 2.22, 95% CI [1.33, 3.71]) were more likely to report experiencing food not lasting compared to respondents who did not receive food assistance. Finally, those who were confident that they could find solutions to their problems (OR = 0.57, 95% CI [0.43, 0.76]) were less likely to report experiencing food not lasting and not having money to get more as compared to those who were not confident in their ability to find solutions to problems.
Discussion
This study explored the nature of food insecurity among adults ≥65 years old in Leon County, FL. Our hypotheses were (1) an inverse relationship exists between food insecurity and socioeconomic status; (2) a positive correlation would be found between accessing community food resources, higher levels of self-efficacy, and food insecurity. Food insecurity was modeled using three dependent variables. The results of this study confirmed our hypotheses that food insecurity is associated with demographics, other individual characteristics, and external factors. We found a relationship between the beliefs of susceptibility and severity and behaviors. All study participants identified as being at one or more levels of food insecurity. A strong relationship exists between the perceived threat of food insecurity and the behavior of receiving food assistance (models 1 and 3). Over half of the study participants access food assistance (community pantries/food giveaways), demonstrating both the perceived benefits and self-efficacy in their ability to solve problems of food insecurity as demonstrated in all three models. In our regression model, low perceived health status was significantly associated with worrying food would run out, a perceived threat; therefore, they were more likely to receive food assistance and find solutions to problems to lessen their likelihood of food insecurity.
Models 1 and 2 of our regression analyses were unexpectedly not statistically significant for an association between LILA and food insecurity, while model 3 showed an association. Additionally, our chi-square tests of independence demonstrated a strong relationship between LILA areas of residence across the three dependent variables and food insecurity, consistent with the literature that LILA is associated with food insecurity among low-income older adults. For example, Bengle et al. (2010) found that among a community sample of older adults in Georgia, low-income older adults were at increased risk of cutting back on basic needs, including food and medication. Carter et al. (2014), in their systematic review of place and food insecurity, discovered that residents in urban areas deemed less desirable (low social capital, poor housing quality, low income, and perceived as unsafe for both businesses and residents) were more likely to be food insecure. Bartfeld et al. (2010) found associations between increased risk of food insecurity and urban area zip codes that lacked access to transportation and were far from supermarkets and grocery stores.
In our study, the relationship between race and food insecurity, while not statistically significant, indicates that African Americans are less likely but not significantly less likely to report food insecurity across the three levels of food insecurity in the models. This is not consistent with the literature, which has found that food insecurity is more prevalent among African Americans/Blacks and Hispanics and is highly associated with race, differences in socioeconomic factors (income, wealth, level of education), and other underlying variables not considered in the models (Bowen et al., 2021; Odoms-Young & Bruce, 2018). The use of non-probability sampling and the unbalanced sample across race/ethnicity may have contributed to the study’s logistic model results, conveying that for the observed study participants, race was not a significant factor in predicting or explaining food insecurity.
This study demonstrated an association between increasing age and decreased odds of running out of food or food not lasting. (Older adults ≥65 years, are further categorized as youngest-old, middle-old, and oldest-old, (Lee et al., 2018)). Several studies found similar results. For example, Mavegam Tango Assoumou et al. (2023) found that among older adults, food-insecure respondents tended to be younger. Berning et al. (2022) found that older households are more food secure than younger households. The research of Jung et al. (2010) suggests that the availability of public resources mandated by the Older Americans Act of 1965, which led to the creation of senior centers, provides older adults with access to nutritious meals, thereby reducing food insecurity within this population. However, as Ziliak and Gundersen (2023) noted, adults over 65 face an ongoing threat of hunger daily. Unlike food insecurity, which public resources can alleviate, hunger is more challenging to quantify and address. Per the USDA, “. . .although hunger is related to food insecurity, hunger is a different phenomenon (USDA Economic Research Service, 2023).” Thus, while our study found decreased odds for food insecurity, the prevalence of hunger within this sample is unknown and of concern.
Study findings indicate that participants who reported accessing food assistance were more likely to face food insecurity. This outcome is consistent with prior research (Coleman-Jensen et al., 2019) that found individuals who experience higher food insecurity may lack the financial resources to purchase additional food; therefore, accessing community food pantries may be a viable option for supplementing household food supplies. Participants in policy initiatives such as SNAP had higher food insecurity (Goldberg & Mawn, 2015; Lee et al., 2011). Therefore, as Bhargava and Lee (2017) postulate, public assistance programs and meal services for older adults may help alleviate food insecurity and enable access to healthcare services. Although food assistance is critical for controlling food insecurity, data from the USDA (Jones, 2022) indicates that only about 48% of eligible older adults participate in SNAP. Low participation in food assistance programs and environmental challenges such as economic downturns may increase food insecurity if seniors lose access to these public resources. Thus, as and Ziliak and Gundersen (2023) note, ongoing monitoring of food insecurity within this population is essential.
This present study also found that participants who reported good or excellent health status were less likely to report food insecurity. The literature supports the association between food insecurity and health status (Leung et al., 2015; Petersen et al., 2019). For instance, lower self-care capacity, functional impairment, certain chronic conditions (diabetes and coronary heart disease), and depression were associated with higher levels of food insecurity (Bengle et al., 2010; Jung et al., 2019; Tang & Blewett, 2021). These conditions may cause food-insecure persons to make tradeoffs between food and healthcare, housing, and other essential needs (Schroeder et al., 2019). Although the study did not explore the participants’ ability to acquire food and prepare meals, it may be reasonable to assert that acquiring and preparing meals is associated with health status. Thus, older adults with fewer impairments may have a greater capacity for managing their daily food needs.
Results indicated that respondents who reported satisfaction with the cost of fruit and vegetables were less likely to skip meals. In this study, the cost of produce may act as a proxy for household income. Thus, higher-income households can purchase preferred produce (Coleman-Jensen et al., 2021; Martin et al., 2016). Food-secure households spend more on food than food-insecure households (Coleman-Jensen et al., 2021). A study by Mook et al. (2016) reported that among adults who were classified as food secure, the cost of fruit and vegetables influenced their purchase. Conversely, cost concerns were less significant among those who were food insecure. In other words, if the adult cannot purchase food, the cost of fruits and vegetables is less relevant.
Finally, respondents who could find solutions to most problems were less likely to report food running out or that their food did not last. This finding was supported by Martin et al. (2016), who found significant evidence that self-efficacy increased food security among disadvantaged populations. Similarly, Jomaa et al. (2020) found that caregivers with high self-confidence in food resource management were less likely to experience household food insecurity. Feeling confident or empowered may enable an older adult to seek solutions to life challenges and decrease adverse outcomes actively. Martin et al. (2016) noted that self-efficacy can be taught in a community-based setting, and improvement in self-efficacy can be observed. They further assert that “when individuals build their self-efficacy to become more food secure, it also requires that community resources are available to support them.” Therefore, societal support (partnerships with existing social service agencies) becomes essential for food security if self-efficacy is to be sustained.
Limitations
There are limitations in this study that must be considered. First, the use of non-probability sampling limits generalizability. Thus, it is not known how well the findings reflect the experiences of older adults nationally. Second, the study is cross-sectional; thus, causality cannot be determined. Third, the study did not tease out the impact of financial resources on food insecurity beyond employment status. Future research should explore this association.
Despite these limitations, as an exploratory study, this project contributes to the literature by expanding our understanding of the factors influencing food insecurity among an older, predominately African-American sample.
Conclusion
By testing the effect of personal and external factors on food insecurity among community-based participants ≥65 years, this study established that socioeconomic and environmental factors indeed impact food insecurity. Because place of residence is associated with food insecurity among older adults, public health interventions are needed for those living in low-income, low-access communities. The study also suggests that food insecurity varies along the aging continuum of those ≥65; therefore, interventions must be stratified by age groups and context. While food assistance programs provide availability, access to these resources is facilitated by self-efficacy. Poverty, rising food prices, and recent rollbacks of COVID-19 assistance policies threaten the stability of food access and availability for this population. Thus, self-efficacy initiatives tailored to the older adult community are necessary for reducing food insecurity.
Qualitative studies are needed to examine the lived experiences perpetuating food insecurity among older adults. Future research should identify self-efficacy approaches to decrease feelings of threat and promote behavioral changes that reduce food insecurity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the National Institute of Minority Health and Health Disparities of the National Institute of Health through Grant Number U54 MD 007582.
IRB Protocol/Human Subjects Approval Number
The Institutional Review Board of Florida A&M University provided approval for this research project. Approval Number: 1551252.