
Abstract
Introduction
People with dementia are at risk of transition to residential aged care due to functional decline and caregiver stress (Paradise et al., 2015; Richardson et al., 2013). Frailty contributes to this functional decline (Pedone et al., 2005) and risk of transition to residential aged care, hospitalization (Milte & Crotty, 2014), and premature mortality (Lehmann et al., 2018). Robust anabolic exercise [(progressive resistance training (PRT)] is considered the most potent strategy to treat frailty (Dent et al., 2017), combined with balance training for falls risk (Dent et al., 2017; Singh et al., 2012). The benefits of PRT include cognitive function, as well as many other conditions relevant to dementia: depression, sarcopenia, osteoporosis, cardiovascular disease, hypertension, diabetes, falls, and other co-morbidities (Escriche-Escuder et al., 2021; Hordern et al., 2011; Sharman et al., 2019; Sherrington et al., 2019; Singh et al., 1997; Song et al., 2018; Vanhees et al., 2012).
Recent Australian government policy is targeted toward supporting informal caregivers and their loved ones with dementia to remain living at home for as long as possible, with the overall aims of improving health outcomes and reducing healthcare costs (Australian Health Ministers Advisory Council, 2015). This is not only a government policy but also best practice as supporting “aging in place” for people with dementia is the preferred option for most older adults (Australian Institute of Health Welfare, 2013). Aging in place aims to support older adults to live in their homes in order to delay or prevent transition to residential aged care for as long as possible.
Aging in place often requires informal caregivers who provide unpaid care to their loved ones, in addition to formal services in the home. However, informal dementia caregivers are susceptible to poor health outcomes, isolation, depression, and anxiety due to the challenging behaviors and the functional decline of their loved ones (Mahoney et al., 2005). They are also reported to be significantly more stressed than caregivers for those who are cognitively-intact (Pinquart & Sörensen, 2003) and present with more severe psychological and physical symptoms (Cheng, 2017). Thus, stress-reduction interventions are of particular interest for these individuals. One of the most studied of such interventions for caregivers is mindfulness-based stress reduction (MBSR) developed by Jon Kabat-Zinn in 1979 (Kabat-Zinn, 2003), which has been used in family caregivers of people with dementia (Han, 2022; Kor et al., 2018; Li et al., 2016; Liu et al., 2018), cancer (Birnie et al., 2010), and developmental disabilities (Bazzano et al., 2015). The focus of MBSR is to increase mindfulness which is a skill of being present in the moment, particularly with sustained awareness of perceptible mental states and processes (Grossman et al., 2004). Mindfulness can be practiced through many meditation forms such as body awareness, mindful movements, yoga postures, and being mindful in daily situations. There are promising results reported with MBSR in reducing informal caregiver psychological symptoms such as symptoms of depression, anxiety, stress, and burden (Jaffray et al., 2016; Li et al., 2016; Liu et al., 2018), as well as associations with higher levels of life satisfaction and mindfulness wellbeing with mindfulness practice (Bhattacharyya et al., 2023).
Although exercise has been used in dementia dyads (prescribed either together or separately) with some benefits for both members of the dyad (Doyle et al., 2021), to our knowledge, there are no studies assessing the combined effects of mindfulness training for dementia caregivers in addition to robust exercise for their loved ones. Exercise for older adults with dementia is adaptable to the home environment and is efficacious in delaying functional decline (Doyle et al., 2021; Heyn et al., 2004; Nelson et al., 2004), however this may be limited by the capacity of the caregiver to deliver these interventions effectively without experiencing an increase in burden and stress. Therefore, a novel and effective program supporting the physical and mental health of older adults with dementia and their informal caregivers could reduce the personal and societal burden of dementia significantly.
We designed “HOMeCARE: Caring for Informal Dementia Caregivers and their Loved Ones via the HOMeCARE Exercise and Mindfulness for Health Program.” The HOMeCARE study implemented MBSR for informal dementia caregivers combined with resistance and balance exercise for people with dementia living at home. The study aimed to not only train the caregiver in the delivery of an effective exercise program to improve the functional capacity of those living with dementia, but to also provide a mindfulness intervention for caregivers to reduce their stress and to increase the sustainability of the intervention. We hypothesized that a dyadic intervention of progressive, home-based resistance and balance training and mindfulness training would improve informal dementia caregivers’ mindfulness state, reduce caregiver burden, and improve their loved one’s functioning mobility.
Methods
Study Design
The HOMeCARE study was a two arm, randomized, controlled, single-blinded, parallel-group trial of MBSR for informal dementia caregivers and home-based PRT and balance training for their loved ones. The protocol was prospectively registered with the Australian Clinical Trials Registry (ACTRN12617000347369) and adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines. Ethical approval was obtained from the University of Sydney Human Research Ethics Committee on 27/01/2017 and written informed consent was obtained from both members of the dementia dyad. Primary and secondary outcomes were collected at 0, 4, 8, and 12 weeks by a blinded assessor. No follow-up assessments were completed.
Participants
The participants consisted of a dyad composed of one informal caregiver and one person with dementia. The participants were recruited from dementia carer support groups, volunteer databases from previous trials, advertisements in newsletters, Dementia Australia website, dementia café groups, and dementia care centers.
Informal caregivers were included if they could sufficiently access and navigate the electronic resources developed for the study, were a family member currently living with the participant with dementia, and/or providing some portion of their daily care including activities of daily living in an informal capacity without pay. Their loved ones with dementia were included if they were ≥ 65 years in 2016; living in the community with at least one informal caregiver; had a diagnosis of mild-moderate dementia of any type, except for Parkinson’s disease dementia, Mini-mental State Exam (MMSE; Folstein et al., 1975) score 12 to 24/30; had at least mild deficits in functional mobility, defined as a Short Physical Performance Battery (SPPB; Guralnik et al., 1994) score <10/12. Parkinson’s disease dementia was excluded as it may require a different approach to exercise than just addressing frailty and mobility or falls risks as intended with the intervention.
Informal caregivers were excluded if they had prior experience with or current use of MBSR. Their loved ones with dementia were excluded if they were currently participating in exercise at moderate-to-high intensity for three or more days a week. Behavioural and psychological symptoms of dementia were not exclusionary. All participants were excluded if they were unable to commit for the full study duration or had an unstable medical condition.
Screening
Potential informal caregivers were interviewed on the telephone by the research assistant who assessed eligibility. Once reviewed and approved by the study physician, the participants were invited to the study site at the University of Sydney, Cumberland Campus, Australia. The study physician interviewed all informal caregivers to obtain a complete medical history and performed a physical examination of all participants with dementia at the study site to ensure eligibility. Baseline assessments were then conducted by the research team.
Interventions
HOMeCARE was a remotely supervised intervention, supported by an initial home visit and weekly video calls. Dyad participants were randomized to either an intervention group or a waiting list group involving usual care. A research assistant demonstrated the intervention in a home visit to each dyad in the intervention group. An iPad was then supplied pre-loaded with mindfulness training material and instructional home-based exercise videos and images, as well as PRT equipment for the exercise component. Comprehensive details of the intervention and control groups are described in Supplemental Materials 1, 2, 3, and 5.
MBSR
The 8-week mindfulness training course for the informal caregivers utilized a modified version of the Palouse Mindfulness Based Stress Reduction (MBSR) course (Kabat-Zinn, 2013). The mindfulness practice was performed for the first 4 weeks before their loved ones started their exercise program. The MBSR practice continued until week 8 and self-selected formal and informal practices were continued until week 12. Formal practices were suggested for approximately for 30 minutes each day and informal practices were integrated in the informal caregivers’ daily lives.
PRT and Balance Training
The person with dementia started their exercise program at week 4, via a home visit with the research assistant, and subsequently facilitated by their informal caregiver. Informal caregivers were instructed to administer the exercise interventions 3 days/week for at least 45 minutes. Every week, a video call was planned to provide supervision and support to the dyad by the research assistant, while viewing an exercise session, if possible, to give feedback and reinforce appropriate progressions of weights and levels of balance, with additional phone calls as needed.
Control Group
The control group dyads were placed on a waiting list to receive the full intervention at the end of the 12-week trial. Both groups continued to receive usual medical care during the intervention.
Outcomes
At baseline, all outcomes were measured by the same research assistant prior to randomization. All follow-up assessments were performed by a blinded assessor not otherwise involved in the intervention.
Details of the three primary outcomes are presented in Supplemental Material 2. Caregiver burden was assessed via the Zarit Burden Interview (ZBI; Zarit et al., 1980), caregiver mindfulness state via the State Mindfulness Scale (SMS; Tanay & Bernstein, 2013), and the loved one’s functional mobility via the SPPB (Guralnik et al., 1994).
Sample Size
The sample size was calculated based on previous studies using the same primary outcome measures and similar interventions. These calculations were based on (1) reduction in caregiver burden via ZBI (OR 0.18; Lowery et al., 2014) and (2) improvement in function in participants with dementia via the SPPB (ES 0.83; LIFE-P, 2006) with alpha .05 and beta .20. This was estimated at 48 dyads (24 control and 24 experimental).
Randomization
The participants were randomized after their baseline assessments and were stratified by level of SPPB (<7 and 7–9) and MMSE (12–19 and 20–24). A research assistant not otherwise involved with the study, generated the stratified randomization sequence via a computerized random number generator (accessed at www.randomization.com; created by Gerard E. Dallal, Ph.D.) and concealed the allocations in sequentially numbered envelopes for the research assistant to open with the participants after the completion of all baseline testing.
Blinding
The HOMeCARE study was single blinded (assessor blinded). Both participants and assessors were blinded to the study allocation until completion of the baseline assessments. It was impossible to blind the participants to the interventions due to awareness of receiving the exercise program and mindfulness training. Participants were asked not to inform the blinded assessor to which group they were allocated.
Adherence
Adherence was captured on a questionnaire and reviewing the MBSR and exercise logs during the weekly status checks via video calls. Adherence was defined as completing the scheduled formal and informal practices for the MBSR course and the exercise sessions with the planned exercises and intensity.
Adverse Events
Adverse events were defined a priori, including exacerbation of underlying diseases, onset of new musculoskeletal, cardiovascular, or metabolic abnormalities. Adverse events were captured via a questionnaire during the weekly video calls.
Statistical Methods
Full statistical methods are detailed in Supplemental Material 2. The primary analytic strategy was intention-to-treat, with all randomized participants included, regardless of dropout or adherence level. The primary outcomes data at each time point were inspected for normality through descriptive statistics, histograms, and Shapiro-Wilk tests. Repeated measures linear mixed models with an unstructured repeated covariance type (for the SMS and SPPB) and AR(1; first-order autoregressive; for the ZBI) repeated covariance type were used to determine changes over time in both members of the dyad, in separate mixed models for each primary outcome. Baseline ZBI data was used as a covariate in its mixed model due to the imbalance in baseline scores between groups. Hedges’ g relative effect sizes (ESs) were determined for each primary outcome using the pooled baseline SD as the denominator and the between group mean difference as the numerator to calculate ES. The analyses were performed on IBM SPSS Statistics version 27 and 28 (IBM Corp. Armonk, NY).
Results
Recruitment and Retention
Figure 1 displays the flow of participants through the study. Thirty-four dyads were assessed for eligibility and nine were randomized to the intervention group or the waiting list control group. The less than planned sample size was due to funding limitations and the advent of the COVID-19 restrictions prior to the completion of recruitment. One dyad in the control group did not complete their week 4 and 8 follow up assessments, there was no week 8 primary outcome data for one informal caregiver in the intervention group and one dyad in the intervention group did not complete their week 12 in-clinic physical performance assessments due to COVID-19. There were no drop-outs in the study.

CONSORT participant flow diagram.
Participants
Participant baseline characteristics are reported in Tables 1 to 3; informal caregiver baseline psychological assessments are provided in Supplemental Table 1. The loved ones were primarily female older adults who presented with four chronic conditions and up to eight prescribed medications. Informal caregivers were mainly older adults, who were not experienced in exercise facilitation and were a spouse/partner of the loved one except for one participant who was a daughter aged 40 years. Six informal caregivers presented with controlled chronic conditions.
Loved One With Dementia: Baseline Sociodemographic and Health Status.

Presented as mean (standard deviation).
Data from three participants.
Confirmed dementia diagnosis with unconfirmed dementia type.
Medications included prescribed, not prescribed, over-the-counter, nutritional, and herbal supplements.
Defined as ≥5 medications.
Estimated volume from packs per day multiplied by years of smoking.
Informal Caregiver Baseline Sociodemographic and Health Status.

Data from two participants.
Presented as mean (standard deviation).
Estimated volume from packs per day multiplied by years of smoking.
Categories as per The Australian Guidelines to Reduce Health Risks from Drinking Alcohol were used at the time of the study, low lifetime risk is ≤2 standard drinks per day or ≤14 standard drinks per week and high lifetime risk is ≥3 standard drinks per day or ≥21 standard drinks per week, lifetime risk regarding lifetime risk of alcohol-related injury (National Health and Medical Research Council, 2009).
Loved One With Dementia: Baseline Body Composition and Physical Performance.

A participant’s height was estimated due to an inability to stand upright for a stretch stature measurement.
Presented as median (range).
Data from three participants were missing for this measure.
Bioelectrical impedance measures derived by the following equations: skeletal muscle mass = 0.401 (height in cm2/resistance in Ohms) + 3.825 (sex: male = 1; female = 0) + age in years (−0.071) + 5.1021, skeletal muscle index = skeletal muscle mass/(height in metres2), fat free mass = −4.03 + 0.734 (height in cm2/resistance in Ohms) + 0.116 (body mass in kg) + 0.096 (reactance in Ohms) + 0.984 (sex: male = 1; female = 0)2, fat mass = body mass in kg–fat free mass.
Values were used from the European Working Group on Sarcopenia in Older People’s age-related sarcopenia diagnostic criteria (Cruz-Jentoft et al., 2010) because they were derived from a validated bioelectrical impedance analysis measurement method.
Higher scores indicate better lower extremity physical performance (Guralnik et al., 1994).
Values were used from the updated European Working Group on Sarcopenia in Older People’s aged-related sarcopenia diagnostic criteria (Cruz-Jentoft et al., 2019).
Adherence
Adherence to MBSR
Adherence to the formal practices was median (range) 36% (0%–55%) and adherence to the informal practices was median 64% (25%–76%).
Adherence to PRT + Balance Training
Adherence to the exercise sessions was median (range) 58% (28%–78%).
Adverse Events
One adverse event was reported for a loved one in the intervention group who had an injurious fall while gardening in her backyard. She was briefly admitted to hosptial overnight, had bruising on her face requiring stitches with no musculoskeltal injuries. This was adjudicated as unrelated to the study and her exercise intervention was re-commenced 2 weeks later. There were no adverse events attributed to the MBSR or exercise intervention itself.
Primary Outcomes
The primary outcomes (ZBI, SMS, and SPPB) are reported in Table 4 and displayed in Supplemental Figures 1 to 3.
Repeated Measures Linear Mixed Model Analyses Mean Scores (95% CIs) and Relative Effect Sizes for all Primary Outcomes.
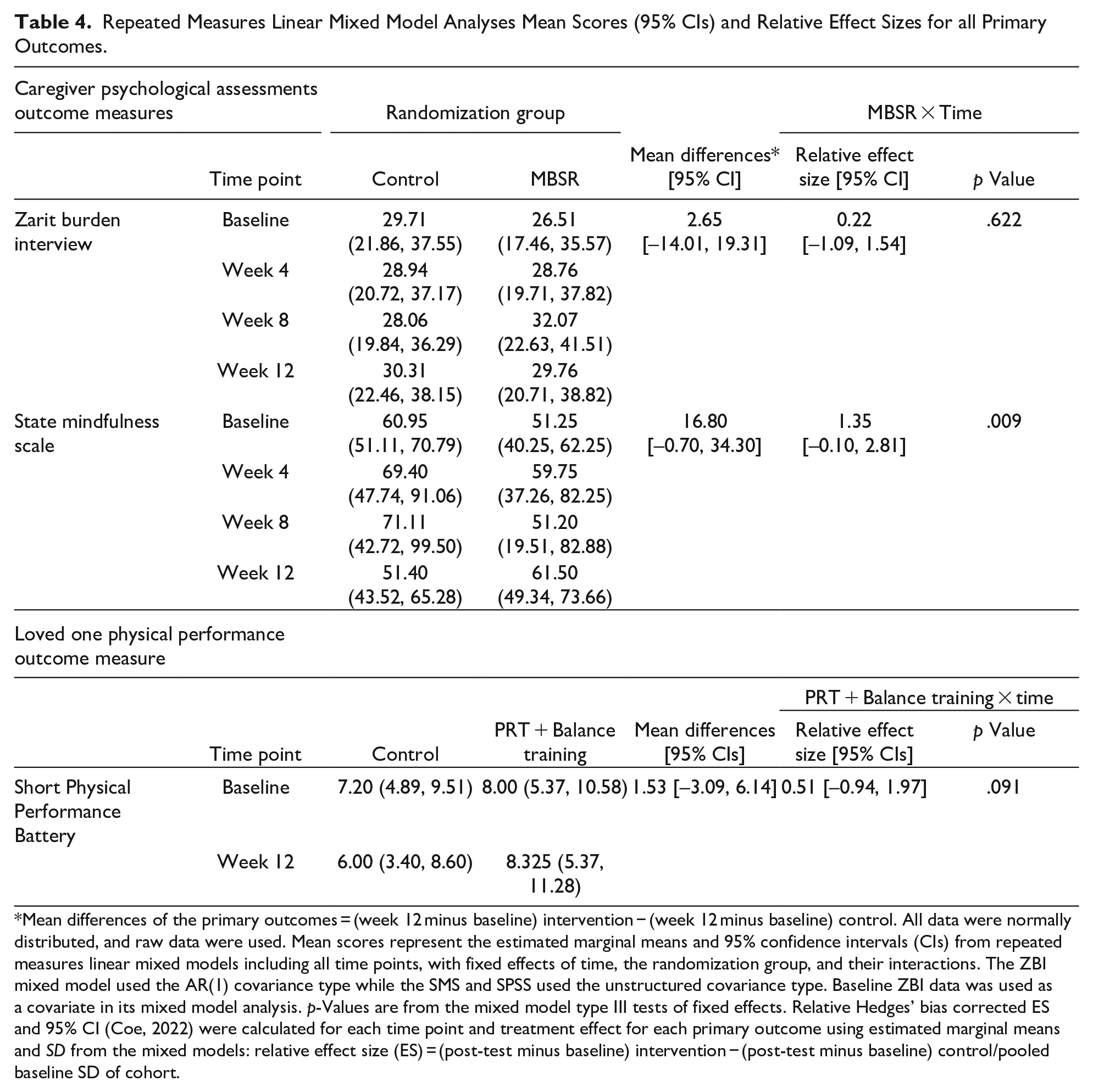
Mean differences of the primary outcomes = (week 12 minus baseline) intervention − (week 12 minus baseline) control. All data were normally distributed, and raw data were used. Mean scores represent the estimated marginal means and 95% confidence intervals (CIs) from repeated measures linear mixed models including all time points, with fixed effects of time, the randomization group, and their interactions. The ZBI mixed model used the AR(1) covariance type while the SMS and SPSS used the unstructured covariance type. Baseline ZBI data was used as a covariate in its mixed model analysis. p-Values are from the mixed model type III tests of fixed effects. Relative Hedges’ bias corrected ES and 95% CI (Coe, 2022) were calculated for each time point and treatment effect for each primary outcome using estimated marginal means and SD from the mixed models: relative effect size (ES) = (post-test minus baseline) intervention − (post-test minus baseline) control/pooled baseline SD of cohort.
Caregiver Burden: ZBI
The intervention group reported a higher baseline ZBI score which was therefore used as a covariate in the mixed model analysis. There was no change in the ZBI related to group assignment (small ES = 0.22; p = .622) and no significant change over time in the overall cohort (F = 0.164, p = .92). The mean difference was less than 3% between both groups. We did not find literature reporting the MCID for the ZBI, but in two studies of MBSR in dementia family caregivers that used the ZBI, the ZBI scores were reported to reduce by a mean difference of 5% to 11% (Brown et al., 2016; Epstein-Lubow et al., 2011).
Mindfulness State: SMS
As hypothesized, there was a statistically significant improvement in mindfulness in the intervention group relative to the control group, a mean difference of 16.8 (30.7%), with a large effect size (ES = 1.35; p = .009). We did not find literature reporting the MCID for the SMS. However, an uncontrolled trial (UCT; Bazzano et al., 2015) of MBSR for family caregivers of people with developmental disabilities reported a mindfulness increase of 15%, assessed by a different mindfulness measure, which is smaller than the increase we saw.
Physical Performance: SPPB
As hypothesized, there was a clinically meaningful improvement in the intervention group, a mean difference of 1.53 points, with a moderate effect (ES = 0.54), and a trend for the group × time effect (p = .091). A SPPB change greater than 1.0 point indicates a clinically meaningful change (Perera et al., 2006).
Discussion
We have reported the primary outcomes of HOMeCARE, the first remotely-supervised trial of MBSR for informal dementia caregivers combined with provision of PRT and balance training for their loved ones with dementia. As hypothesized, the intervention significantly improved the informal caregiver’s mindfulness state and the functional mobility for their loved ones by a clinically meaningful amount. Although it did not improve the informal caregiver’s perceived burden, notably it did not worsen it despite the demands of both learning mindfulness and facilitating exercise sessions.
Our first key finding was that the functional mobility of the loved ones with dementia improved meaningfully. Importantly, the informal caregivers had minimal exercise experience and facilitated the exercise intervention to their loved ones as opposed to an exercise professional, with only weekly remote supervision by a research assistant. To our knowledge, only three RCTs of home-based exercise in people with dementia used SPPB as an outcome and one RCT is currently pending results (Cezar et al., 2021). The two completed RCTs (Callahan et al., 2017; Pitkälä et al., 2013) reported no improvements in the SPPB. The first study described approximately 15 minutes of strength and balance exercises per session for up to 24 sessions over 2 years as part of their occupational therapy intervention, but did not describe the exercise type, intensity, and planned progressions (Callahan et al., 2017). The second study described an hour of endurance, strength, balance, and executive functioning exercises twice a week for 12-months, but did not describe the intensity and planned progressions (Pitkälä et al., 2013). This suggests that the exercise prescriptions were insufficient in terms of progression and/or intensity. Our study progressed the exercise intensities when the participant reached a specific exertion level with safe technique and progressed the balance exercises after mastering their prescribed levels. The provision of exercise by the informal caregivers appeared to be safe as there were no adverse events attributed to the study, although the small sample size precludes any definitive conclusions in this regard. Therefore, the provision of robust, evidence-based exercise to a loved one after physician screening appears adaptable to the home environment. Notably, among the 34 dyads screened, only 1 of the 25 excluded were ineligible because of medical instability, suggesting the potential generalizability of this intervention to patients with dementia and multiple comorbidities living at home with an informal caregiver.
Our second key finding was a significant increase in the informal caregiver’s mindfulness state. An increase in caregiver mindfulness state reduces the risk in developing stress, anxiety, and depression (Li et al., 2016). A systematic review of five RCTs implementing MBSR for dementia family caregivers reported reduced symptoms of depression and levels of anxiety (Fjorback et al., 2011), but the RCTs did not report mindfulness as an outcome. However, a systematic review (Li et al., 2016) of MBSR for dementia family caregivers included three UCTs and two RCTs, but mindfulness was not significantly increased in the studies. Our study suggested that MBSR was able to be undertaken in informal dementia caregivers without prior experience, and only one face-to-face training session supported by digital and written materials.
Our third key finding, contrary to our hypothesis, was that caregiver burden did not change differentially in response to the intervention. Over time, there was a small and non-significant (F = 0.164, p = .92) change of 2.65 points on the ZBI across both groups. We are uncertain whether this change is clinically meaningful as the MCID is not known. Other trials implementing MBSR have reported mixed outcomes for caregiver burden in this cohort. An RCT (Brown et al., 2016) and an uncontrolled trial (Epstein-Lubow et al., 2011) reported a small reduction in caregiver burden, as measured by the ZBI. However a systematic review of three RCTs (Shim et al., 2021) reported an improvement in caregiver burden in only one RCT (Liu et al., 2018), and a review (Liu et al., 2018) of five RCTs was uncertain whether MBSR reduced caregiver burden.
Our novel trial involved the provision of exercise by the informal caregivers in addition to completing the MBSR course, which has never been published to our knowledge. The lack of benefit on perceived burden in the intervention group, despite their improved mindfulness and improved function of their loved ones, could have been due to the commitment of completing the MBSR intervention in addition to the provision of the exercise program for their loved ones, which included learning how to facilitate the exercise program by older adults with health concerns of their own. Thus, it is an important finding that caregiver burden was not differentially increased despite the many demands of learning two entirely new tasks: mindfulness and exercise supervision.
Limitations
The primary limitation of this study is the smaller than planned sample size of 48 dyads due to limitations of funding and the advent of the COVID-19 restrictions prior to the completion of recruitment. This reduced the statistical power of the primary outcomes and resulted in wide confidence intervals. Post-hoc power analyses (Faul et al., 2009) indicated that a sample size of 55/group would have been needed show statistical significance for the SPPB, given the ES of 0.54 suggesting the possibility of a type II error.
Second, the exercise adherence was less than expected which reduced the opportunities for exercise progression and full adaptation of strength, balance and mobility. This may have been due to the increase in time and demand for the informal caregivers to facilitate the exercise sessions in addition to attending to their activities of daily living. Exercise adherence may increase if informal caregivers completed the exercises together with their loved ones which will also likely improve informal caregiver psychosocial and physical health (Doyle et al., 2021).
Finally, the adherence to the MBSR program was also sub-optimal, particularly for the formal practices. The higher adherence to informal practices suggests that it was more feasible to integrate into the informal caregiver’s activities of daily living than to schedule personal time to complete the formal practices of 30 min/day. Given that the informal caregivers experienced a large and statistical improvement in mindfulness even with their low-to-moderate adherence rate, future trials should test the feasibility and efficacy of a more abbreviated mindfulness intervention. One that could be incorporated directly into their caregiving tasks and exercise facilitation, rather than as a separate practice of its own, would be of great relevance.
Conclusion
The HOMeCARE study was the first trial combining MBSR for informal dementia caregivers and caregiver-provision of PRT and balance training for their loved ones. The study appeared acceptable, feasible and adaptable to the home environment with no safety issues identified, despite the remote supervision. The HOMeCARE program resulted in a statistically significant improvement in informal caregiver mindfulness state which has yet to be reported in this cohort, as well as a clinically meaningful improvement in functional mobility for their loved ones. There were no significant effects on caregiver burden. However, it is notable that the extensive requirements of the informal caregivers in the intervention group to learn not only how to practice mindfulness, but also how to supervise moderate-high intensity PRT and challenging balance exercises in their frail loved one with dementia for the first time - were substantial. The fact that these requirements did not increase burden relative to waiting list control informal caregivers is an extremely novel and important finding. Further large-scale trials are warranted to confirm and extend our findings to optimize adoption, adherence, and adaptation to this dyadic intervention, and ultimately to support ageing in place and quality of life for older adults with dementia and their informal caregivers.
Supplemental Material
sj-doc-9-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-doc-9-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-1-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-10-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-10-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-2-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-2-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-3-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-3-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-4-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-4-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-5-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-5-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-6-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-6-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-7-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-7-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-8-ggm-10.1177_23337214231203472 – Supplemental material for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial
Supplemental material, sj-docx-8-ggm-10.1177_23337214231203472 for Caring for Informal Dementia Caregivers and Their Loved Ones Via the HOMeCARE Exercise and Mindfulness for Health Program (HOMeCARE): A Randomized, Single-Blind, Controlled Trial by Tommy Lang, Kenneth Daniel, Michael Inskip, Yorgi Mavros and Maria A. Fiatarone Singh AM in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
The authors would like to thank the caregivers and their loved ones with dementia who contributed their valuable time and efforts to make the HOMeCARE study possible. The authors would also like to thank Prof. Sharon Naismith and Dr. Milena Simic for their contributions to the grant application.
Author Note
The results were partially presented at the American Geriatrics Society 2023 Annual Scientific Meeting. The analysis and publication of the study was completed in partial fulfillment of Tommy Lang’s Honors degree.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Dementia Collaborative Research Centers’ (DCRC) national grant round in 2016. The DCRC had no role in the design, methods, subject recruitment, data collections, analysis, and preparation of this paper.
Institutional Review Board
The University of Sydney Human Research Ethics Committee, approval number 2016/795.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.