
Abstract
Background:
Live-in migrant caregivers play a critical role in supporting older adults with dementia in Israel but often experience significant emotional strain. Interventions to support their mental health remain scarce.
Objective:
To pilot-test a brief virtual reality (VR)-based mindfulness intervention for live-in migrant dementia caregivers and to explore its impact on caregiver burden, state mindfulness, and subjective experience.
Methods:
In a mixed-methods pilot conducted at a dementia day center, six live-in migrant caregivers participated in four 10-min VR mindfulness sessions. Quantitative measures included pre–post caregiver burden and post-session state mindfulness. Semi-structured interviews explored perceived relevance and impact.
Results:
Caregiver burden decreased post-intervention and State mindfulness ratings indicated high present-moment awareness. Qualitative findings described VR as a source of brief relief, emotional recalibration, and as a bridge to identity and belonging, suggesting preliminary benefits for stress reduction and coping among live-in migrant dementia caregivers.
Introduction
The global rise in life expectancy has increased the number of older adults living with dementia (WHO, 2025). In Israel, where most people with dementia remain in the community, live-in migrant caregivers have become a core pillar of support (Cohen-Mansfield & Golander, 2023). Similar reliance on live-in migrant care is evident in Mediterranean countries, parts of Asia, and North America (Cangiano, 2014; Michel & Peng, 2012), amid demographic shifts that have reduced the availability of unpaid informal caregivers (Freedman et al., 2024). While this arrangement provides essential support and can ease family burden (Grenz & von Kutzleben, 2024), it may also place caregivers in vulnerable circumstances with significant stressors (Ulitsa et al., 2025). The present pilot examines whether a brief virtual-reality-based mindfulness intervention can support the psychological well-being of these caregivers.
Stress and Coping Among Live-in Migrant Dementia Caregivers
Migrant caregivers live with the care-recipient and provide continuous physical and emotional support, often coping with behavioral symptoms such as aggression or unfounded accusations (Ayalon et al., 2025). Their work is compounded by restrictive employment conditions that limit job mobility and increase vulnerability to exploitation, discrimination, and emotional abuse (Ayalon, 2012; Green & Ayalon, 2018; Shamir, 2013). Prolonged separation from family and challenges of cultural adaptation further contribute to distress (Carlos & Wilson, 2018; Ulitsa et al., 2025). These chronic stressors may lead to significant burden, which in turn can result in adverse psychological outcomes (Pearlin et al., 1990; Zarit et al., 1986). Among migrant caregivers, documented symptoms include depression, anxiety, and suicidal ideation (Ayalon, 2012).
To promote the psychological well-being of migrant caregivers, this study draws on the transactional model of stress and coping (Lazarus & Folkman, 1984), which views stress as a process shaped by appraisal and coping resources. Coping may be problem-focused, aimed at changing the stressor, or emotion-focused, aimed at managing emotional responses. Because migrant caregivers often have limited control over their circumstances, emotion-focused strategies are especially relevant (Iavarone et al., 2014; Shinan-Altman & Ayalon, 2019). Within this context, mindfulness may help caregivers regulate emotions and enhance well-being.
Mindfulness-Based Interventions: Benefits and Barriers to Implementation
Mindfulness refers to consciously attending to present-moment experiences with open awareness and a non-judgmental attitude toward thoughts, feelings, and body sensations (Bishop, 2004; Davis & Hayes, 2011). Originally developed as a therapeutic practice to manage stress and chronic pain (Kabat-Zinn, 1982), mindfulness training typically involves focusing attention on the present moment, such as through the breath. Mindfulness-based interventions have been shown to improve psychological well-being and reduce stress in both clinical and non-clinical populations (Chiesa & Serretti, 2009; Khoury et al., 2015).
Among family caregivers of people with dementia, a meta-analysis found that mindfulness led to significant reductions in depression and perceived stress, along with improved mood (Liu et al., 2017). These outcomes may be explained by two emotion-focused coping mechanisms. First, present-moment, non-judgmental awareness helps interrupt automatic reactions to sustained stress and strengthens emotion regulation. Second, it encourages acceptance of difficulties that cannot be changed, lowering reactivity and enabling more adaptive coping with ongoing, uncontrollable stressors (Lindsay & Creswell, 2017; Mackenzie & Poulin, 2006).
Despite these benefits, several barriers limit participation in traditional mindfulness programs. Maintaining focus can be effortful, especially for novices, and may evoke frustration, boredom, or distress (Anderson et al., 2019). Structurally, standard programs require substantial time: eight weekly sessions, daily home practice, and a full-day retreat (Kabat-Zinn, 1990). This intensity reduces accessibility (Ma et al., 2023), especially for live-in migrant caregivers of persons with dementia, who face continuous care demands and have little time to engage in lengthy structured programs.
A Virtual Reality-Based Approach to Mindfulness Practice
To address barriers to traditional mindfulness programs, virtual reality (VR) has emerged as a promising tool to support mindfulness practice (Cawley & Tejeiro, 2024; Ma et al., 2023). VR uses a headset that displays a 360° audio-visual environment, creating an immersive experience for the user. In a typical VR mindfulness session, participants are transported to calming natural landscapes, such as a beach, forest, or river, with soothing music and guided instructions. These sensory cues act as attentional anchors that help users stay present and reduce mind-wandering (Chandrasiri et al., 2020; Ma et al., 2023; Navarro-Haro et al., 2017; Seabrook et al., 2020).
Empirical evidence indicates that VR-based mindfulness increases open, receptive awareness of present-moment experience (Chandrasiri et al., 2020; Navarro-Haro et al., 2017). In addition, studies report improvements in well-being and reductions in perceived stress, including after a single session (Cawley & Tejeiro, 2024; Ma et al., 2023; Seabrook et al., 2020). Most effects were observed in the affective domain, including reductions in negative emotions like anger and sadness, and increases in positive states such as relaxation and improved mood (Navarro-Haro et al., 2017; Seabrook et al., 2020).
VR also offers structural advantages: it eases attentional demands typically required during mindfulness practice, supports shorter interventions, and allows sessions to be repeated anytime, improving accessibility and standardization (Chandrasiri et al., 2020; Lutz et al., 2008; Mrazek et al., 2019). Reported drawbacks, such as mild simulator sickness or headset discomfort, are generally rare and minor (Kennedy et al., 1993; Ma et al., 2023; Seabrook et al., 2020).
The Current Study
VR technology offers a promising approach to enhance mindfulness practice and support psychological well-being. While most VR-mindfulness studies target community samples (Cawley & Tejeiro, 2024; Chandrasiri et al., 2020; Navarro-Haro et al., 2017; Seabrook et al., 2020); evidence in at-risk groups is still limited (e.g., Fonseca et al., 2024). To our knowledge, no study has examined the use of VR mindfulness among live-in migrant caregivers of persons with dementia. VR-based mindfulness, with its immersive and guided delivery, facilitates present-moment engagement within the constraints of continuous caregiving and is readily adaptable to cultural context. This pilot tested a brief VR-based mindfulness intervention for live-in migrant dementia caregivers in Israel. We examined session-to-session changes in state mindfulness, estimated a preliminary effect size for caregiving burden, and qualitatively explored perceived relevance and benefits in daily life.
Methods
Study Design
This study employed a mixed-methods design, integrating quantitative measures of caregiver burden and state mindfulness with qualitative interviews exploring participants’ experiences of the VR intervention.
Participants
This study was conducted with “Melabev”, a nonprofit organization operating four adult day care centers for community-dwelling individuals with dementia in Israel. Most attendees are accompanied by their live-in migrant caregivers, who remain on site during programing. Participants were recruited at one center; six live-in migrant caregivers enrolled. Eligibility required ≥6 months of dementia-care experience; exclusions were limited English proficiency, relevant visual/hearing impairments, or prior motion/simulator sickness. All participants provided written informed consent, and the protocol received Institutional Review Board approval of Bar-Ilan University, Israel (approval no. 270325532). All participants provided written informed consent prior to participation.
Procedure
The study was conducted on-site at the day center and coordinated with the center’s management to ensure that participation did disrupt the center’s routine operations.
Quantitative Procedure
At the start of the study, participants completed a short demographic questionnaire and the caregiver burden scale. They then engaged in four VR mindfulness sessions, scheduled twice per week. After each session, participants completed the meta-awareness questionnaire to assess their state of mindfulness. Upon completion of all four sessions, participants repeated the caregiver burden scale.
Measures
Caregiver burden was assessed with the four-item screening version of Zarit Burden Interview (ZBI-4; Bédard et al., 2001). Items are rated 0 to 4 (“never” to “nearly always”) and summed to 0 to 16; higher scores indicate greater burden. Scores ≥ 8 suggest high burden. State mindfulness was assessed with four items adapted from the State Mindfulness Scale (SMS; Tanay & Bernstein, 2013) by Hadash et al. (2016) rated 1 to 5 (“not at all” to “to a large extent”). Items indexed attention to physical sensations, emotions and thoughts, and noticing pleasant and unpleasant internal experiences during the VR session. Because each item reflects a distinct component of state mindfulness, mean scores per session were calculated for each item across all participants. We also calculated mean scores of all four items.
Qualitative Procedure
Following the final VR session, each participant took part in a semi-structured interview focusing on their experiences with the intervention and its perceived impact in the context of live-in caregiving. Interviews were conducted on-site in English, lasted approximately 30 min and were audio-recorded with participants’ consent. Recordings were transcribed verbatim and anonymized before analysis. All participants gave consent to publish the findings of the study.
VR Mindfulness Intervention
Participants completed four 10-min VR mindfulness sessions using a Meta Quest 2 headset. Session 1 used a pre-existing 360° guided meditation across natural landscapes. Sessions 2 to 3 presented an underwater dive and a beach-sunset environment, accompanied by soft ambient music and voice-over scripts adapted from mindfulness guidelines (Kelly et al., 2022). Session 4 repeated the participant’s preferred environment. The three formats (varied landscapes, dynamic underwater, calmer beach) enabled exploration of differential engagement and preferences. Researchers assisted with headset setup, and participants completed each session seated and unaccompanied to minimize distractions. For more details, see Appendix 1.
Data Analysis
Quantitative Analysis
For caregiver burden, pre- and post-intervention means and standard deviations were computed. Effect sizes (d) were calculated as the pre–post change score divided by the pretest standard deviation. For state mindfulness, item-level means were calculated for each session across participants and plotted over the four sessions to visualize trajectories; we also summarized the mean across all four items.
Qualitative Analysis
Transcripts were analyzed using reflexive thematic analysis (Braun & Clarke, 2006, 2021). The process involved repeated reading, inductive coding of meaning units, and iterative refinement of themes capturing shared experiences and interpretations. Both manifest and latent meanings were considered. To enhance trustworthiness (Lincoln & Guba, 1985), we ensured reflexivity, transparent documentation, and team discussions. Two researchers independently reviewed the coding and resolved discrepancies by consensus. Quotations were lightly edited for clarity while preserving meaning.
Results
Results are presented in three parts: baseline sample characteristics; quantitative outcomes; and qualitative interview findings on caregivers’ experiences with the VR-mindfulness intervention.
Sample Characteristics
The sample included four women and two men, originating from the Philippines (n = 4) and India (n = 2). Mean age was 46.0 years (SD = 6.84; range = 40–56). Participants had an average of 9.0 years of dementia-care experience (SD = 5.14) and 5.1 years with their current care-recipient (SD = 2.69). Average residence in Israel was 10.5 years (SD = 4.23), and mean self-rated health was high (M = 4.67, SD = 0.52, on a 1–5 scale).
Quantitative Results
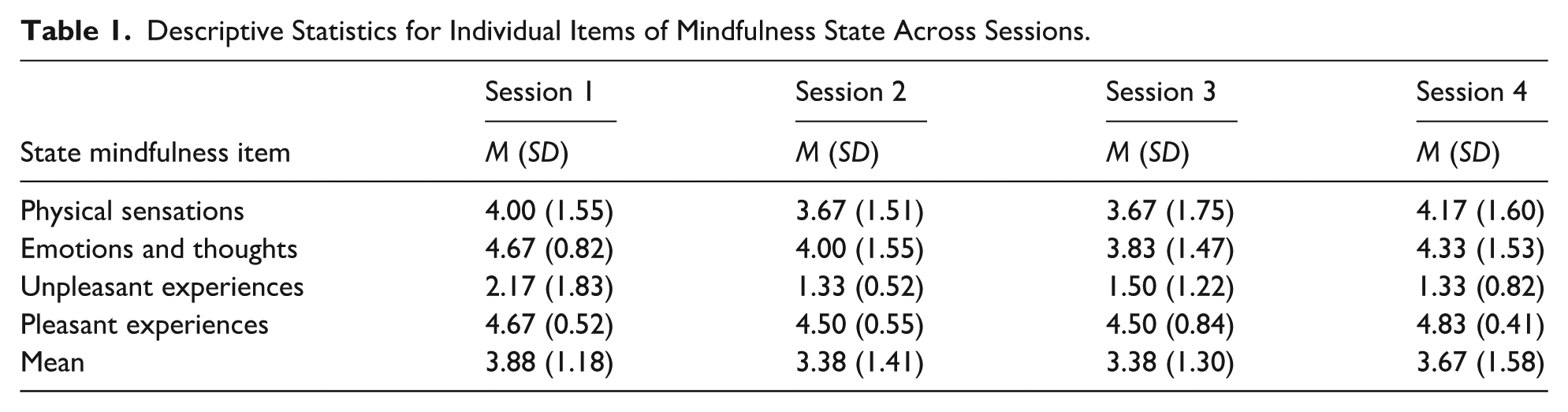
Caregiver burden decreased from 6.00 (SD = 1.90) pre- to 3.50 (SD = 2.43) post-intervention (d = 1.14). State mindfulness item means are presented in Table 1. Figure 1 presents trajectories across sessions. Item 1 (awareness of physical sensations) and Item 2 (awareness of emotions and thoughts) were relatively high and fluctuated without a clear pattern. Item 3 (unpleasant experiences) remained lowest and declined slightly. Item 4 (pleasant experiences) remained highest with a small late increase. As shown in Figure 2, the overall mindfulness mean was highest at Session 1 (M = 3.88, SD = 1.18), dipped at Sessions 2 to 3 (M = 3.38; SDs = 1.41, 1.30), and rose at Session 4 (M = 3.67, SD = 1.58).
Descriptive Statistics for Individual Items of Mindfulness State Across Sessions.
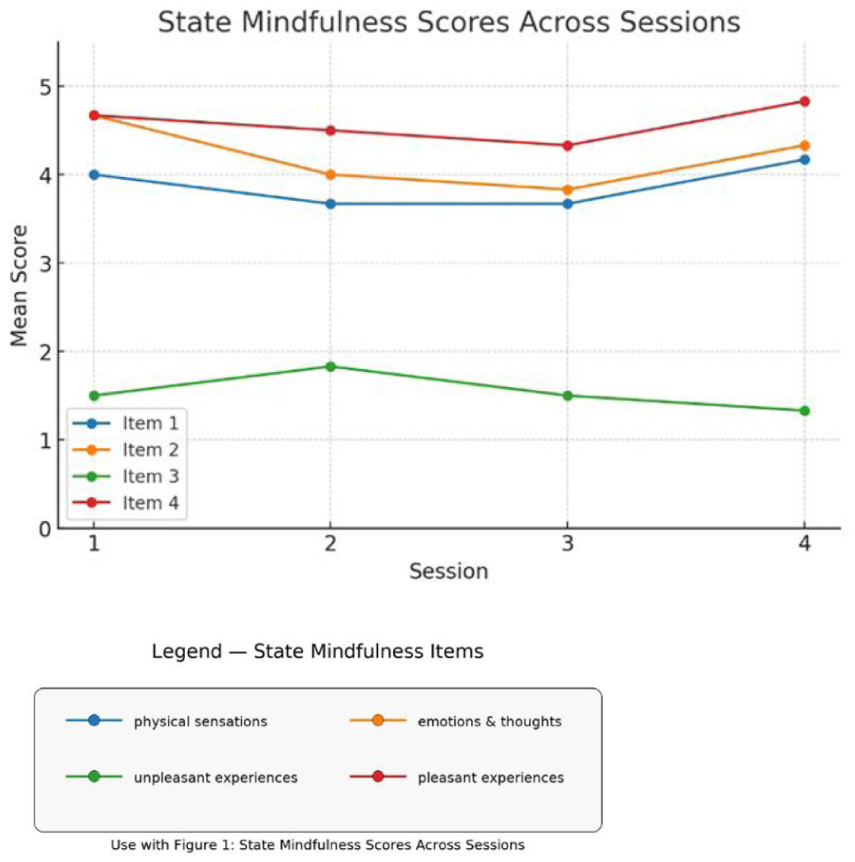
Trends in mean state mindfulness item scores across four VR mindfulness sessions.

Trends in Mean mindfulness state items over four VR-mindfulness sessions.
Qualitative Results
Three themes emerged: (1) VR as relief from care pressures, (2) VR as emotional recalibration, and (3) VR as a bridge to identity and belonging.
Theme 1: VR as a Space of Relief and Escape from Care Pressures
For live-in migrant caregivers, the VR mindfulness sessions offered rare relief from the unrelenting demands of dementia care. Participants described the immersive experience as calming and restorative, allowing them to “switch off” mentally and reconnect with themselves:
For ten minutes, I relaxed my mind. . . I am not thinking about my employer, I am not thinking about anything. I am mentally totally relaxed. . . I can forget everything and start [with] a new good mood. (Interview 1) When you listen to the video or you see the nature, it seems like you're connected with God. . . and then mentally [you] uplift yourself [. . .] sometimes it's better to relax for a few minutes, thinking about yourself because as a caregiver it's very hard to make a meditation [. . .] you have to follow the routine every day. . . so sometimes you forget yourself. (Interview 5)
The immersive nature of VR created a powerful sense of “being elsewhere”, offering both sensory and emotional escape. One caregiver likened it to watching a film in a theater, something otherwise out of reach, while another described it as freedom from the confines of live-in caregiving:
This (VR) is like a theater. I can't get a chance to go to the theater every day. . . VR is very comfortable for me because I can see near and very clearly. (Interview 1) Sometimes you’re stressed at home. You feel like home is a prison. . . VR is immersing yourself in whatever you are. (Interview 3)
For some, the sessions also provided a quiet moment to pause and refocus inward:
Even though I have a lot of things happening. . . after this (VR session), I felt that I have to stop and just be, like, for a couple of minutes to have some time with me, myself. (Interview 3)
Although one participant mentioned mild dizziness in the deep-ocean scene, she enjoyed the other sessions:
It was a deep ocean. I'm afraid of deep water. I don't know how to swim. (. . .) I enjoyed the latest video, the beach, and the sunset. . . it’s relaxing. (Interview 4)
Overall, this experience was perceived as a temporary sanctuary, allowing caregivers to step away briefly from continuous caregiving and regain balance and calm.
Theme 2: VR as a Tool for Emotional Recalibration in Caregiving
Caregivers framed VR as a practical coping aid that “reset” emotional balance, supporting patience, calm, and more positive interactions. Several reported feeling “more relaxed” or “at peace”, which improved day-to-day care:
My employer has dementia, and he needs more time. You need more patience, more caring. . .after this session I feel more confident handling her because it lessens my stress. . . It's not really totally removed, but at least it decreases my stress. (Interview 5).
Others viewed VR as a short intervention that prevented stress from spilling over into caregiving interactions:
Stress. . . leads you somewhere else. I think these VR sessions might help because stress is in our mind. [. . .] It will temporarily help you to reduce the stress that you [are] having. (Interview 3)
Participants also reported that the benefits often lasted beyond the session, reflected in greater patience, calm, and energy. Some felt that short, regular sessions could help maintain this balance:
Every day we [could] do 10 minutes like this. It is very helpful for our life because it is stress going down. (Interview 1) Caregivers viewed VR as a complement to, not a replacement for, other coping strategies such as community support, faith, or outdoor breaks. Still, they described it as a uniquely accessible tool that could be integrated into daily routines: “Even 10 minutes. . .to make [this] mind relax and the body relax.” (Interview 2) One participant described VR as a kind of companionship: “It seems that somebody's talking to you, somebody is listening to you [. . .] it’s relaxing, and at the same time you just feel like talking together.” (Interview 5)
Taken together, these accounts show that caregivers experienced VR as a way to lower stress, regain composure, and sustain their demanding caregiving roles.
Theme 3: VR as a Bridge to Identity and Belonging
Beyond immediate stress relief, VR evoked powerful memories of home, family, and cultural belonging. For live-in migrant caregivers separated from loved ones, it bridged their caregiving realities with personal histories. Natural landscapes stirred memories of childhood and family life:
I feel like I'm. . . in my place. . . going [to] the beach early in the morning with my family, with my children [. . .] [hearing] all the sounds of the beach, and [seeing] the sunrise. . . some people coming from fishing [. . .] I want to bring it to my home. (Interview 2)
For some, these experiences evoked deep nostalgia and homesickness. Yet this longing was often restorative, helping caregivers reconnect emotionally with a world they missed:
Sometimes I feel, like, homesick [. . .] we're far away from home. Especially from your family. (Interview 2). While I'm looking [at] the video, the sea, the bridges, the trees, I feel relaxed. [. . .] When I was a kid. . . we had oceans, rivers, nature, so I feel related to that video. (Interview 5) Caregivers described these moments as more than memories; they provided a sense of continuity and emotional grounding. The same caregiver expressed both joy and longing when recalling her childhood environment: “I feel I miss my past life. I wish I [could] go back there [laugh], but this is impossible. But anyway, through that video, I feel relaxed. And I say, ‘oh, such a beautiful video!’” (Interview 5). At times, these memories were so vivid they brought tears, yet participants viewed the release as positive and healing: “I felt longing and missing. [. . .] It helped me to refresh again, even in simple things like this. [. . .] ‘Wow, this is amazing. . . how I can recall everything’. I'm very happy to be part of this.” (Interview 2)
Overall, VR served as a portal cherished spaces of identity and belonging, reminding caregivers of who they are beyond their caregiving roles.
Discussion
This pilot evaluated one of the first VR-based mindfulness interventions for live-in migrant dementia caregivers in Israel. Using a mixed-methods design, we combined quantitative measures of burden and mindfulness with qualitative interviews to illuminate participants’ experiences. Quantitatively, participants reported high present-moment awareness, frequent positive and infrequent negative experiences, and a large preliminary reduction in perceived burden. Qualitative analysis identified three impact themes: (1) brief respite from continuous caregiving, (2) support for emotional recalibration, and (3) reinforcement of identity and belonging.
The findings suggest that the intervention activated emotion-focused coping (Lazarus & Folkman, 1984), a set of strategies especially relevant to live-in migrant caregivers who have limited capacity to modify stressors such as round-the-clock care and prolonged family separation (Ayalon, 2012; Carlos & Wilson, 2018; Shamir, 2013; Ulitsa et al., 2025). In particular, caregivers described
These qualitative insights were supported by the quantitative findings. Within the four items adapted from the State Mindfulness Scale (Hadash et al., 2016), the item reflecting pleasant experiences consistently scored higher than the item assessing unpleasant experiences. Although mindfulness is not primarily intended to induce positive mood, creating pleasant affective states may reduce barriers to engagement and enhance emotional accessibility, particularly for novice mindfulness practitioners (Seabrook et al., 2020).
A second emotion-focused coping strategy evident in this study was
Taken together, distancing and emotional regulation appear to have functioned as complementary strategies. Distancing, while potentially detrimental if relied upon persistently (e.g., linked to depression or burnout), can be adaptive in contexts of intense stress, providing short-term relief from emotional strain and creating space to mobilize other coping resources (Folkman & Moskowitz, 2004; Holahan et al., 2005). Emotional regulation, by contrast, is consistently associated with reduced psychological distress (Chiesa & Serretti, 2009; Creswell, 2017) and with the enhancement of adaptive responses to stress (Hölzel et al., 2011). The observed reduction in caregiver burden suggests that the intervention may have alleviated strain both by providing moments of escape and by strengthening caregivers’ capacity for more balanced engagement in daily care.
A unique finding of this study was participants’ reports of connection to their identity and sense of belonging. For example, one caregiver described how the beach scene vividly reminded him of family routines in his homeland. This extends beyond immediate emotion regulation and aligns with meaning-focused coping, a later extension of the transactional model of stress and coping (Park & Folkman, 1997). Meaning-focused coping involves reappraising stressors in ways that foster a sense of purpose, continuity, and inner strength. This interpretation is further supported by the relatively high scores on state mindfulness scale items related to attentional awareness of bodily sensations, thoughts, and emotions, which may have created a “window into the self” (Morganti et al., 2024). Some participants described the need “to just stop and be with myself for a few minutes,” highlighting rare introspection amid demanding routines. For others, the experience felt spiritual, evoking connection to God or a guiding presence. Together, these moments suggest that VR-based mindfulness may open deeper layers of identity and meaning, extending its impact beyond immediate stress relief toward lasting resilience.
Limitations
This pilot study has several limitations. First, the small sample size and lack of a control group limit generalizability, and findings should be viewed as exploratory. Second, the four-session format may not have allowed participants to develop deeper mindfulness capacities such as acceptance. Third, qualitative responses may have been influenced by social desirability, given caregivers’ vulnerable status. Fourth, although most participants experienced the natural VR environments as calming, one reported discomfort. Future designs should account for personal preferences, cultural relevance, and potential triggers by allowing for greater individualization or content selection.
Conclusions
This pilot shows that brief VR-based mindfulness is feasible and perceived as beneficial for live-in migrant dementia caregivers. Beyond emotion-focused coping (e.g., distancing and emotional regulation), participants also described experiences of meaning-focused coping, such as renewed connection to identity and belonging. Given its flexible and adaptable delivery, larger controlled studies are warranted to develop culturally sensitive, accessible, and scalable programs for caregivers’ well-being. As language and cultural barriers may prevent migrant home care workers from seeking assistance in the host culture, VR mindfulness-based interventions have the potential to offer an easy and cost-effective solution.
Footnotes
Appendix 1
Acknowledgements
We are very grateful to the six caregivers who participated in this study. We thank Dr. Zeev Friedman, CEO of Melabev, for his cooperation and encouragement and for his strong commitment to supporting caregivers, and Tomer Azulay for his valuable assistance with the VR sessions.
Ethical Considerations
This study was approved by the Institutional Review Board of Bar-Ilan University, Israel (approval no. 270325532).
Consent to participate
All participants provided written informed consent prior to participation.
Consent for Publication
Not applicable.
Author Contributions
L.C. led the conceptualization, study design, data collection and analysis, and manuscript drafting. A.S., P.S., N.U., and S.R. contributed to the conceptualization, data collection, analysis, and manuscript writing. L.A. supervised all stages of the project. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.