
Abstract
Keywords
Introduction
The Coronavirus (COVID-19) pandemic has deeply and disproportionately affected older adults’ mental health and well-being (Magesh et al., 2021). One reason for this is that the severity of the disease and risk for death, especially in the first year of the pandemic, was significantly higher for older adults, with 81% of COVID-19 deaths in the US in 2020 occurring among adults aged 65 or older (Schöley et al., 2022; Tejada-Vera & Kramarow, 2022). Several health and wellbeing-related areas of life were negatively impacted by the pandemic and the policies instituted to decrease disease spread, such as social distancing and isolation in quarantine (Bann et al., 2021; Hausman et al., 2022; Silva et al., 2023). For example, during the first year of the pandemic, the National Poll on Healthy Aging Survey found that one-fifth of adults aged 50 to 88 experienced worse depression or sadness (Gerlach et al., 2021). Depression is one of the most prevalent mental disorders and a common cause of increased risk for physical problems, self-neglect, suicide, decreased social functioning, decreased cognitive functioning, reduced life satisfaction in old age, and increased mortality among older adults (Maier et al., 2021; Sjöberg et al., 2017). In a study using telephone survey data from 126 older adults aged 60 or older in a Colorado community, Scott et al. (2021) found that participants experienced decreased mental and physical health, reduced health service access, lower social engagement, and increased coping behaviors during the COVID-19 pandemic.
Potential contributing factors to decreased mental health in older adults during the pandemic may include worsened health behaviors (Harrison et al., 2021) and increased financial difficulties (Hayashi et al., 2022). Harrison et al. (2021) used an online survey and found that adults aged 40 or older across four U.S. census regions decreased physical activity during the pandemic. Hayashi et al. (2022) examined social frailty and depressive symptoms among 1,103 community-dwelling adults aged 65 or older in Japan in 2020 and used financial difficulties in their assessment. They also studied home exercise, finding that it may buffer the association between frailty and depressive symptoms, given the decrease in physical activity related to the pandemic. In another study focusing on health behaviors during the pandemic, Knell et al. (2020) used a convenience sample of 1,809 adults residing in the U.S. who completed a 15-min self-report questionnaire in April and May 2020. They investigated how health behaviors changed at the early stages of the pandemic and examined participant characteristics associated with health behavior changes and why these changes may have occurred. They found that the social distancing and travel restrictions due to the COVID-19 pandemic impacted individuals’ positive health behaviors (sleep, physical activity) and negative health behaviors (alcohol consumption, drug use, and tobacco use) (Knell et al., 2020). In a study conducted in Spain, García-Esquinas et al. (2021) used data from 3,041 participants in four cohorts of community-dwelling individuals aged 65 years or older and collected through interviews just before and after the COVID-19 lockdown. They found that the COVID-19 confinement was not associated with a deterioration in lifestyle risk factors (smoking, alcohol intake, diet, and weight), except for decreased physical activity and increased sedentary time, which reversed with the end of confinement. However, chronic pain worsened, and there were moderate declines in mental health which did not seem to reverse after restrictions were lifted.
Disparities in COVID-19 Outcomes by Gender and Race
Research indicates that gender disparities in COVID-19 outcomes exist, and gender-related factors may increase the impact of the pandemic on vulnerable populations globally (Galasso et al., 2020; Gausman & Langer, 2020; Marik et al., 2021). However, mixed findings exist about the relationship between gender and COVID-19 outcomes (Gausman & Langer, 2020), with some studies showing greater risk for women (Ausín et al., 2021; Galasso et al., 2020) and other studies showing greater risk for men (Danielsen et al., 2022). Research also indicates women constitute a disproportionately high percentage of both formal and informal caregivers which may further increase their risk of exposure (Fisher & Ryan, 2021). In the United States, 65% of family caregivers are estimated to be women, and 80% of their care is for someone aged 50 years or older (Gausman & Langer, 2020). Caregiving during the pandemic proved especially difficult and negatively impacted caregivers’ mental health (Hughes et al., 2021). In addition, women were more likely to experience job loss during the pandemic (Fisher & Ryan, 2021). In summary, all these factors increased the risk of experiencing adverse mental health outcomes during the pandemic among women in the US.
Race and ethnicity have been associated with disparities in COVID-19 disease severity (Hamler et al., 2022; Lopez et al., 2021). In addition to being at a higher risk for infection and mortality (Centers for Disease Control and Prevention [CDC], 2020), older adults from minority race and ethnicity groups have been shown to be more vulnerable to negative economic, behavioral, and social impacts related to the pandemic (Gauthier et al., 2020; Magesh et al., 2021; Wang et al., 2021). Previous studies have found that COVID-19 infection rates in racial and ethnic minority groups are associated with low socioeconomic status (SES) and income (Samuel et al., 2021). Using the Census Bureau’s nationally representative pooled Household Pulse Survey from April 2020 to May 2021, Lee and Singh (2021) examined monthly trends and disparities in health status by race and ethnicity and SES. They used logistic regression models and disparity indices and found that disparities in health status based on race and ethnicity and socioeconomic status increased during the pandemic.
Current Study and Contribution
Much of the research examining health behavior change and financial difficulties during the pandemic focuses on the general adult population in the U.S. or older adults in other countries (García-Esquinas et al., 2021; Hayashi et al., 2022; Knell et al., 2020). There is a lack of studies examining health behaviors and financial difficulties and their relation to mental health outcomes in older adults in the U.S. during the pandemic. Understanding the changes in health behaviors, financial difficulties, and mental health outcomes and how these intersect will inform health professionals designing programs to help improve the health of older adults post-pandemic. Therefore, this study aimed to explore the interrelationships between health behaviors, financial difficulties, and depressive symptoms among older adults during the COVID-19 pandemic across various demographic backgrounds in a large sample of older adults using a national dataset. Specifically, we tested the following hypotheses:
H1: Health behaviors of older adults changed during the pandemic compared to before the pandemic;
H2: The impact of COVID-19 on health behaviors and financial difficulties among older adults varied across gender and race;
H3: Older adults who experienced financial difficulties were more likely to have negative health behaviors during the pandemic than before the pandemic;
H4: Older adults who had more negative health behaviors during the pandemic compared to before the pandemic were more likely to experience a higher level of depressive symptoms;
H5: Older adults who experienced financial difficulties are more likely to experience a higher level of depressive symptoms during the pandemic.
Methods
Data and Sample
The data used were from Round 1 (conducted in 2010), Round 5 (conducted in 2015), and Round 10 (conducted in 2020) of the National Health and Aging Trends Study (NHATS) and the supplementary survey on COVID-19 which was also administered in 2020. NHATS is led by the Johns Hopkins University Bloomberg School of Public Health and is sponsored by the National Institute on Aging (U01AG032947). NHATS is a longitudinal, nationally representative study started in 2011 that contains data on more than 8,000 Medicare beneficiaries aged 65 years or older in the U.S., with an oversampling of Black and older respondents and additional individuals added in 2015 to the cohort to maintain a representative population (Freedman & Kasper, 2019). In Round 5 (2015), 8,334 respondents living in community and residential care settings other than nursing homes completed in-person interviews, yielding a response rate of 73.6% (Kasper & Freedman, 2019). The participants were interviewed in person annually (Montaquila et al., 2012).
Measurements
The outcome of interest was the level of depressive symptoms. The independent variables were financial difficulties and health behavior variables, including walking, vigorous activity, eating, alcohol consumption, smoking, watching TV, and sleeping. Depressive symptoms, financial difficulties, and health behavior variables were from the supplementary COVID-19 data. Covariates included age, marital status, gender, race, and education.
Depressive Symptoms
Participants were asked the following questions: “During two weeks in the past 12 months, during the COVID-19 outbreak, in a typical week, how often have you felt lonely? How sad or depressed have you felt about the outbreak? How worried or anxious have you felt about the outbreak? Recurring thoughts about the outbreak and its effects?” The variables were re-coded so that a higher value meant a higher level of depressive symptoms.
Financial Difficulties
Participants were asked, “Has your household had any financial difficulties because of the COVID-19 outbreak?”
Health Behavior Variables
Participants were asked, “During the COVID-19 outbreak, in a typical week, have you spent more or less time than you did before the outbreak: walking for exercise, doing vigorous activities, eating including snacking, drinking alcohol, smoking or vaping, watching TV or online programs or movies, and sleeping.” The variables were re-coded so that a higher value meant a higher intensity.
Covariates
Covariates were selected because of their established relationships with the independent and dependent variables found in previous research (Gausman & Langer, 2020; Maier et al., 2021). These demographic variables include age (in years), gender (male or female), education, marital status (married and living with a partner coded as one category, and separated, divorced, widowed, and never married as the other category), and race/ethnicity (classified into four categories: (a) non-Hispanic White, (b) non-Hispanic Black, (c) Hispanics, and (d) Others, including American Indian, Asian, and native Hawaiian). Non-Hispanic White was the reference group. Age, marital status, Gender, and race were from Round 10. Education information was not collected in Round 10, so education data from Round 1 was used for participants who joined the study in Round 1. Education information from Round 5 was used for participants recruited in Round 5.
Analytic Strategy
Our analyses took into account the complex survey design and weighted sampling probabilities of the data source during all the analysis. We obtained univariate and bivariate analyses using descriptive statistics by calculating frequencies and proportions. Chi-squared and Fisher’s exact tests were conducted to compare behavioral and financial variables across genders and races/ethnicities. We conducted Fisher’s exact test when the expected frequency in a cell was less than 5. Values were considered statistically significant if the p-values were <.05.
Structural equation modeling was built on the complete data in R using the “lavaan” package predicting depressive symptoms and behavioral changes. We built confirmatory factor analysis models on both endogenous (or explanatory) and exogenous (or response) variables. First, we conducted exploratory factor analyses for ordinal data on the endogenous variable side to obtain latent factors that explain the common features in behavioral change variables. We used exploratory factor analysis to obtain the three latent factors in the seven behavioral change variables. The three latent factors represented active behavior (walking, vigorous activity), sedentary behavior (eating, watching TV, sleeping), and unhealthy behavior (smoking, drinking alcohol), respectively. Next, we built a three-factor confirmatory factor analysis model to obtain the best-fit measurement model for behavior change. For the exogenous variables, we had four survey questions that were driven by a common latent factor related to depression and mental health. Thus, we constructed a one-factor confirmatory factor analysis measurement model for ordinal data to measure the severity of participants’ depressive symptoms. For these models, we used both standardized variables (mean = 0, SD = 1) and the actual values of the variables. We considered factor loadings greater than 0.3 in the standardized indicator models clinically meaningful. All indicators had positive loadings on latent factors, meaning that a higher value of a latent factor led to higher intensities of relevant behaviors or symptoms.
Next, we built a structural model to establish the relationship between financial difficulties, behavioral changes, and depressive symptoms. The measurements of behavioral changes and depressive symptoms were obtained from the confirmatory factor analysis models described above. We measured behavioral changes by three latent factors: active behavior, sedentary behavior, and unhealthy behavior. Depressive symptoms were measured by one latent factor. We included demographic variables, including gender, age, race, ethnicity, education, and marital status in the structural model as covariates. We also examined the impact of financial difficulties on behavioral changes. We obtained the parameter estimation using the weighted least square mean and variance adjusted estimator by the default setting in the “lavaan” package for ordinal data. Chi-square test, Root Mean Square Error of Approximation (RMSEA), Comparative Fit Index (CFI), Tucker Lewis Index (TLI), and Standardized Root Mean Square Residual (SRMR) were used to assess model fit with the following values: RMSEA < 0.08, CFI > 0.95, TLI > 0.95, and SRMR < 0.08 (Hooper et al., 2008).
Results
Description of Study Sample
We summarized the weighted and unweighted descriptive statistics of the study variables, including frequencies and percentages (see Supplemental Table A). Of the 3,118 participants included in the study sample that represents over 30 million older adults national-wise, 58.37% were female, and 76.62% were Non-Hispanic White. About 60% of the participants had completed high school or more education, and nearly half were married or living with a partner. Table 1 presents the unweighted frequency and percentage of each depressive symptom, financial, and behavioral variable. In this sample, 32.1% of the participants experienced loneliness for at least some days, while 27.7% experienced worries or anxiety at a moderate or severe level during COVID-19. Additionally, about 22.0% of the participants reported feeling sad or depressed at a moderate or severe level during COVID-19. For health behaviors, 27.3% of the participants walked less, 24.4% had less vigorous physical activity, 37.0% spent more time watching TV, 24.5% changed their eating pattern (eating more or less), and 21.4% changed their sleeping pattern (sleep more or less) compared to before the pandemic. (See Supplemental Table B for the corresponding weighted statistics).
Bivariate Associations Across Gender and Ethnicity Groups. a

Calculated using unweighted sample. fIndicates Fisher’s Exact Test.
Bivariate Associations and Confirmatory Factor Analysis
As shown in Table 1, the bivariate associations were examined across gender and race and ethnicity. Walking, eating, drinking alcohol, and sleeping were significantly associated with gender. Compared to male participants, more female participants reported walking less, eating (including snacking) more or less, and sleeping less during the pandemic than before. On the other hand, male participants reported drinking more alcohol during the pandemic than female participants. Financial difficulties and all behavior change variables except drinking alcohol and smoking were significantly associated with race and ethnicity. Non-Hispanic Black, Hispanic, and Other races reported more financial difficulties, less walking, less vigorous activity, and eating more or less during the pandemic than before the pandemic compared to their Non-Hispanic White counterparts.
The confirmatory factor analysis results are shown in Table 2. All indicators in the confirmatory factor analysis had positive loadings on latent factors, meaning that a higher value of a latent factor led to higher intensities of relevant behaviors or symptoms. Participants who experienced a higher level of depressive symptoms reported a higher frequency of feeling lonely, sad, or depressed about the outbreak, worried or anxious about the outbreak, or having recurring thoughts about the outbreak and its effects.
Results of the Confirmatory Factor Analysis. a

Calculated using sampling weights. Comparative Fit Index (CFI) = 0.87; Tucker-Lewis Index (TLI) = 0.85; root mean square error of approximation (RMSEA) = 0.03; Standardized Root Mean Squared Residual (SRMR) = 0.04.
Results From the Structural Equation Model
The structural equation model revealed adequate model fit predicting depressive symptoms (Chi-square = 286.23, degree of freedom = 119, p < .01; CFI = 0.87; TLI = 0.84; RMSEA = 0.03; SRMR = 0.04). Unstandardized and standardized coefficient estimates and p-values for depressive symptoms are presented in Table 3. The final model indicated that financial difficulties and health behaviors were strongly associated with depressive symptoms. Participants who experienced financial difficulties, on average, had more severe depressive symptoms compared to those who experienced no financial difficulties (b = 0.67 p < .05). Active behavior had a strong negative association with depressive symptoms (b = −0.15, p < .001), whereas sedentary behavior had a strong positive association with depressive symptoms (b = 0.45, p < .001). Older female adults experienced more depressive symptoms during the pandemic than their male counterparts (b = 0.55, p < .001). Compared to Non-Hispanic White participants, Hispanic participants experienced more severe depressive symptoms (b = 0.54, p = .01), while participants in the other races category experienced less severe depressive symptoms (b = −0.35, p < .05) during the pandemic than before. Figure 1 presents the measurement model pathways from each latent factor (depressive symptoms, active behavior, sedentary behavior, and unhealthy behavior) to the variables and the structure model pathways that predict depressive symptoms from sedentary, active, and unhealthy behaviors. The unstandardized coefficient values are on the arrows, the same values as those in Tables 2 and 3. Note that Figure 1 shows that participants who experienced financial difficulties tended to engage more in sedentary behavior (b = 0.54, p < .05).
Standardized and Unstandardized Coefficients for Final Structural Equation Model. a
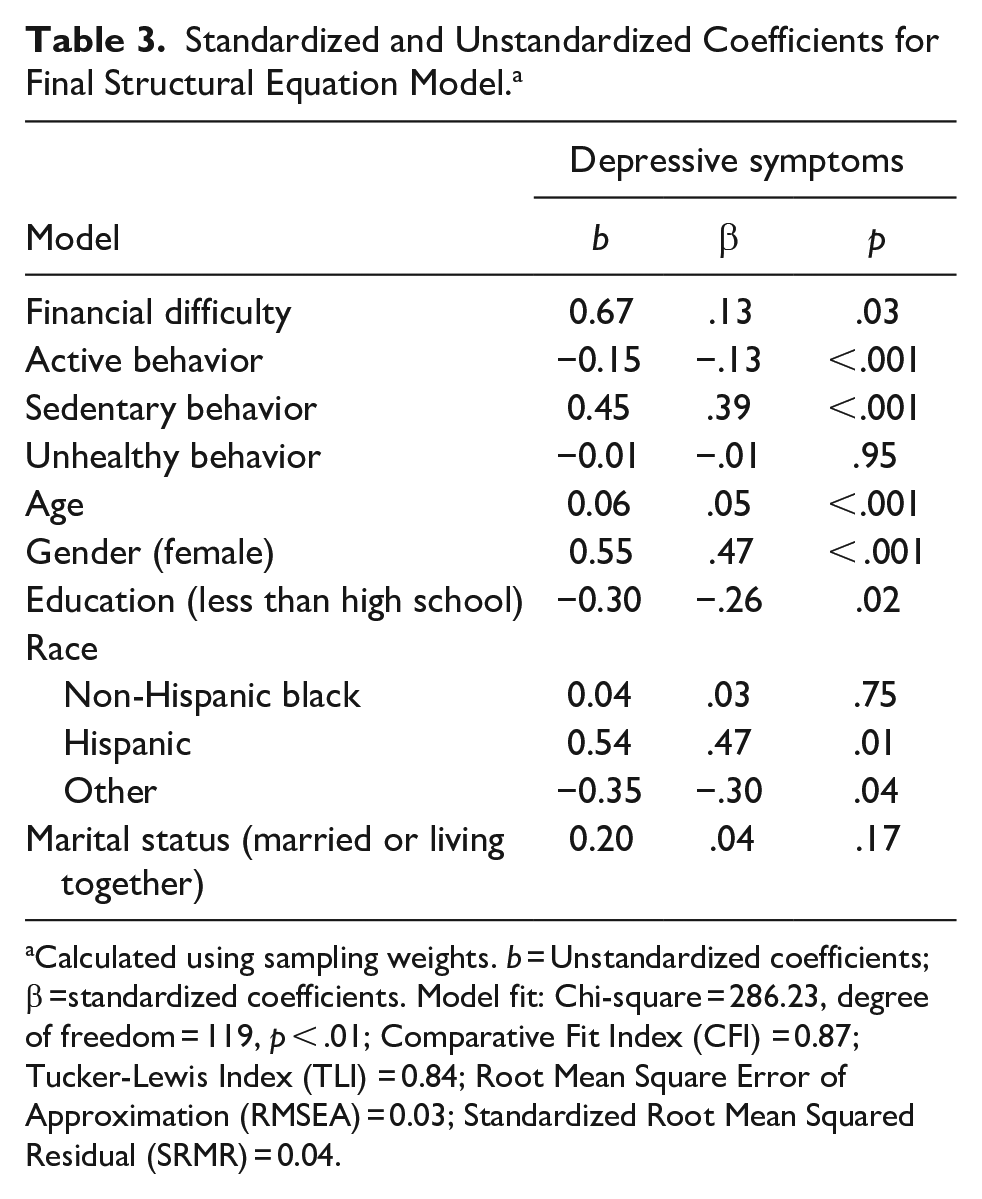
Calculated using sampling weights. b = Unstandardized coefficients; β =standardized coefficients. Model fit: Chi-square = 286.23, degree of freedom = 119, p < .01; Comparative Fit Index (CFI) = 0.87; Tucker-Lewis Index (TLI) = 0.84; Root Mean Square Error of Approximation (RMSEA) = 0.03; Standardized Root Mean Squared Residual (SRMR) = 0.04.

Results of the final structural equation model calculated using sampling weights.
Discussion
Our study used structural equation modeling to provide nationally representative findings about associations between health behavior changes, financial difficulties, and depressive symptoms among older adults during the COVID-19 pandemic across gender and race. Greater health behavior changes and financial difficulties were correlated with more depressive symptoms. In addition, we found significant disparities in health behavior changes, financial difficulties, and depressive symptoms related to gender and race. Our findings about older adults in the U.S. align with studies of older adults in other countries that have examined single relationships such as physical activity and depressive symptoms (Hayashi et al., 2022) and health behaviors and mental health (García-Esquinas et al., 2021). The results herein are unique in that we examined multiple relationships between the three areas of health behavior changes, financial difficulties, and depressive symptoms and studied these relationships across gender and race categories.
In establishing the rates of health behaviors during the COVID-19 pandemic among older adults, we found that, for several health behaviors, about one-quarter of older adults changed their habits during the pandemic. Spending time watching TV was particularly notable, with 37.0% of older adults watching more TV during the pandemic than before. In addition, we found significant disparities in health behavior changes during the pandemic related to gender and race. These results are consistent with Knell and colleagues’ (2020) study examining the entire U.S. adult population; that is, there were health behavior changes during the pandemic and disparities based on demographic factors exist. Our results are unique in that they show health behavior changes and disparities in health behavior changes among older adults, a demographic group that was more vulnerable to death and severe symptoms from COVID-19 than the general population (Schöley et al., 2022; Tejada-Vera & Kramarow, 2022).
Other findings are worth noting. First, female older adults reported walking less, eating more or less, and sleeping less than their male counterparts during the pandemic compared to before the pandemic. This may be because females are more likely to be caregivers (Gausman & Langer, 2020), and the added duties and stress related to the COVID-19 pandemic contributed to worse health behaviors. Second, male participants reported drinking more alcohol during the pandemic. This is consistent with research showing that adult men drink more than women (White, 2020). However, it is not consistent with a review by Peltier et al. (2019) showing that adult women are more likely to drink as a reaction to stress than men (Peltier et al., 2019). Our finding may indicate that this gender difference was the opposite for older adults when faced with the stress of the COVID-19 pandemic. Third, Non-Hispanic White respondents reported more walking, more vigorous activity, and fewer changes in eating during the pandemic compared to before the pandemic than their counterparts from other racial groups. This is consistent with research conducted before the pandemic showing that better health behaviors existed among White older adults than older adults in other race and ethnic groups in the U.S. (Hughes et al., 2020).
Our study considered how negative mental health outcomes may be exacerbated by the coexistence of multiple disadvantaged and marginalized identities among older adults. In light of the attention that gender and race have received in the aging development and psychology fields, the limited research on the gender and race differences on health behavior and depressive symptoms among older adults is needed in future studies. In addition, future research should consider taking a mixed-method approach to combine quantitative results with insights from qualitative studies to include contextual measures and take a person-in-environment perspective to investigate broader social inequalities such as sexism or racism and reveal the underlying cultural or historical values embedded in older adults’ multiple identities that may affect their mental health.
Limitations
This study has some limitations. A limitation is that the analysis results do not represent the whole U.S. older adult population. NHATS only surveyed Medicare beneficiaries aged 65 or older, which limited the understanding of populations not covered by Medicare. Complex survey sampling designs should be considered in future studies. In addition, we were limited in this investigation by a lack of racial diversity in the sample; the majority of participants were non-Hispanic Whites, which may have masked finer group differences. Furthermore, the cross-sectional design limited the study to only examining health behavior change, financial difficulties, and depressive symptoms among older adults at a particular point in time, while behavioral, financial, and mental health conditions are likely to change over time. NHATS follows older adults and tracks financial, lifestyle, and health changes and factors that may also affect these changes over multiple years. For example, aging and cognitive function decline affect older adults’ behavioral, financial, and mental health (Fauth et al., 2020). However, these factors could not be included in the analysis using the cross-sectional COVID-19 data. Future studies should consider longitudinal data with multiple survey cycles to develop a more comprehensive understanding of this topic.
An additional limitation is that we could only use the variables that were exclusively available within the COVID-19 dataset. For example, “financial difficulties” was the only variable representing older adults’ financial situation in the COVID-19 data. NHATS’ regular cycle surveys contain rich financial situation information, like household income in 2015 (round 5) data. The integration of financial data from the 2015 cycle with the COVID-19 dataset resulted in a substantial number of missing values. As our research is centered on examining the effects of the COVID-19 pandemic on the mental health of older adults, the use of financial variables from round 5 was precluded from the analysis. Another variable that posed limitations to our study was the classification of gender, as the NHATS survey exclusively provided options for male and female genders. Notably, other gender identities, such as non-binary, were not considered in the survey. Future studies would benefit from the inclusion of additional financial situational data and a wider range of gender identity choices.
Implications for Policy and Practice
With the rapidly growing aging population worldwide (WHO, 2022), a better understanding of depression in old age is highly valuable from clinical and public health perspectives. Due to the stigma surrounding mental health, many older adults are reluctant to seek necessary care for mental health conditions (Fu et al., 2023; Iob et al., 2022). As a result, depression is often under-identified and under-reported by healthcare professionals and older adults themselves (Krishnamoorthy et al., 2020). Our study’s findings about the associations between health behaviors, financial difficulties, and depressive symptoms and disparities across gender and race may improve health professionals’ knowledge about groups more likely to experience depressive symptoms. This could lead to improved identification of older adults’ needs for mental health interventions. Furthermore, a greater awareness of the significant burden of depressive symptoms in the U.S. associated with the COVID-19 pandemic among older adults is crucial as older adults have also faced a disproportionally greater share of morbidity and mortality associated with the COVID-19 pandemic (Schöley et al., 2022; Tejada-Vera & Kramarow, 2022). In the future, health professionals can offer interventions to help decrease depressive symptoms among older adults, such as home exercise programs (Hayashi et al., 2022).
Formal financial management training programs, such as the Savvy Saving Seniors® financial education toolkit developed by National Council on Aging (NCOA) to help professionals educate older adults about financial management skills (Greenberg et al., 2016; National Council on Aging [NCOA,], 2019) and the AARP’s Money Management Program assisting low-income older adults in managing their finances (Johnson et al., 2016), should be promoted to older adults, especially among disadvantaged groups. Additionally, policies aimed at helping vulnerable populations make sound financial decisions can help older adults address financial difficulties, especially after the COVID-19 pandemic. For example, the Senior Financial Empowerment Act (2021) requires the Federal Trade Commission to provide educational materials to seniors and families about safe and smart financial practices (Congress.gov, 2021). Such policies assisting older adults, along with a concerted effort by health professionals to address physical and mental health issues, are needed to reduce the negative impact of COVID-19 on older adults in the U.S.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231192820 – Supplemental material for Health Behaviors, Financial Difficulties, and Depressive Symptoms Among Older Adults Across Gender and Race During the COVID-19 Pandemic
Supplemental material, sj-docx-1-ggm-10.1177_23337214231192820 for Health Behaviors, Financial Difficulties, and Depressive Symptoms Among Older Adults Across Gender and Race During the COVID-19 Pandemic by Yujun Liu, Heng Wang and M. Courtney Hughes in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-2-ggm-10.1177_23337214231192820 – Supplemental material for Health Behaviors, Financial Difficulties, and Depressive Symptoms Among Older Adults Across Gender and Race During the COVID-19 Pandemic
Supplemental material, sj-docx-2-ggm-10.1177_23337214231192820 for Health Behaviors, Financial Difficulties, and Depressive Symptoms Among Older Adults Across Gender and Race During the COVID-19 Pandemic by Yujun Liu, Heng Wang and M. Courtney Hughes in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data from National Health and Aging Trends Study (NHATS), sponsored by the National Institute on Aging (U01AG032947), is available to other researchers for replication purposes (2) The data can be accessed on the NHATS website: ![]() (3) The study reported in the manuscript was not pre-registered.
(3) The study reported in the manuscript was not pre-registered.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.