
Abstract
Introduction
A caregiver (CG) is a person who provides physical and mental care to individuals with a range of problems, including supporting their health and ability to do daily living activities. The term “CG burden” (Wade et al., 1986; Zarit et al., 1980) refers to the impact of the patient care on the emotional, physical, social, and financial domains of the caregiver. Included among the features of CG burden are depression, the deterioration of physical ability, and other stresses that negatively impact the quality of life of CGs (Chuakhamfoo et al., 2020; Lethin et al., 2020). Previous studies have reported three factors related to people with dementia (PwD) that might contribute to the CG burden: (1) the characteristics of the PwD, the stage and type of dementia, functional ability, and the severity of the Behavioral and Psychological Symptoms of Dementia (BPSD); (2) the demographic data of the CGs, including their gender, age, socioeconomic status, relationship with the PwD, personality, duration of care, coping skills, and learned resourcefulness (Chen et al., 2015; Gaugler et al., 2005; M. Pinyopornpanish et al., 2021; Yaffe et al., 2002); and (3) the support systems (Muangpaisan et al., 2010), including CG training programs, healthcare accessibilities and networks, respite care, public services, and community support.
COVID-19 emerged in 2020 and rapidly spread worldwide, causing a global pandemic that affected societies and economies. COVID-19 symptoms range from asymptomatic to severe respiratory failure, possibly occurring with a higher mortality rate in older people (Guan et al., 2020). Therefore, there are several recommended COVID-19 prevention protocols, including social distancing, masking, travel restrictions, and quarantine, to reduce viral transmission (The Government Public Relations Department, Thailand, 2021). The COVID-19 pandemic had negative physical and mental effects on PwD and CGs, either in terms of access to medical care or quality of life. As a result, the rate of disability and death among PwD increased, while the quality of life for CGs declined (Caratozzolo et al., 2020; Czeisler et al., 2021). Moreover, there are also concerns that the social restrictions during the pandemic may have had an adverse effect on CGs’ psychological health, manifesting as stress, irritability, depression, confusion, and insomnia (Brooks et al., 2020).
In Thailand, previous studies before the pandemic showed the characteristic of CG of PwD in Thai rural area. Most of them (86%) were informal caregivers and 63.2% of CGs were the PwD’s child. Informal CGs had regular work outside the home and had either minimal supporting system or other CGs to help (Chuakhamfoo et al., 2020; Sittironnarit et al., 2020). Two recent studies demonstrated that for PwD, COVID-19 prevention policies worsened their cognitive function (53.4%–55.1%), neuropsychiatric symptoms (NPS) (48.3%–51.9%), increased the incidence of new-onset NPS (25.9%), and caused functional decline (34.5%) (Borelli et al., 2021; Rainero et al., 2021). Previous research found that the incidence of stress in CGs increased from 9% to 22% of CGs before and during the COVID-19 pandemic (Nikolaidou et al., 2022). However, few global and local studies have focused on the effects of COVID-19 on the mental health, well-being, and health-related concerns of CGs (Cohen et al., 2020; Losada et al., 2022; Park, 2020). Consequently, the present study aimed to explore the impact of the pandemic on CG burden and examine the association of potential factors such as patients’ factors (functional change, neuropsychiatric symptoms, stage and severity of dementia) and CG’s factors (depression, CG characteristics, and support).
Materials and Methods
Study Design
This was a cross-sectional study using an electronic-based questionnaire administered to the primary CGs of PwD (Bédard et al., 2001; Hemrunrojn, 2011; Kaufer et al., 2000; Lotrakul et al., 2008; Mahoney & Barthel, 1965; Pinyopornpanish et al., 2020; Silpakit et al., 2015; Yi et al., 2020). This study was conducted between September 2021 and January 2022. Ethical approval was provided by the Research Ethics Committee (protocol number 621/2564).
Participants
The study participants were enrolled at the Geriatric Clinic at Siriraj Hospital, which is a tertiary hospital in Bangkok, Thailand, and via an online survey process. The 166 participants were recruited and their eligibility for participation in the study was determined by using screening questions. The inclusion criteria were as follows: (1) primary CGs of PwD who were diagnosed in any stage of dementia by geriatricians or neurologists and who were currently under treatment follow-up; (2) primary CGs who provided care to PwDs for at least 4 hours per day without remuneration; (3) primary CGs who had no communication problems; and (4) in case of visual or hearing impairment or unable to access the electronic questionnaire, availability of a family member or researcher who could fill in the questionnaire on their behalf. The primary CGs of PwD who were institutionalized 3 months before enrollment were excluded. The final eligible participants consisted of 135 primary CGs, who were recruited in the study and their data were included in the analysis. All the participants gave informed online consent prior to participating in the study.
Data Collection and Measures
Data collection was performed through an electronic questionnaire using a QR code generated by the researchers. The survey was completed by the primary CG or one of the researchers in the case that the CG had a visual or hearing impairment or was unfamiliar with the technology and needed assistance filling in the questionnaire. The questionnaire was composed of items related to both the CG and the PwD, including the demographics, burden, depression, and concerns of CGs and the NPS and functional capacity of PwD. In addition, the researcher inquired about the situation before and during the pandemic, as well as the individual’s responses to the questionnaire.
CG Burden
The Thai version of the Zarit Burden Interview (ZBI-12) was used to assess CG burden. Each item was rated for the frequency of symptoms on a 4-point Likert scale, from 0 (never) to 4 (almost always). The total scores ranged from 0 to 48, with a high score indicating a higher burden. The burden score of 0 to 10 was defined as “no to mild burden,” 11 to 20 as “mild to moderate burden,” and 21 to 48 as “severe burden” (Bédard et al., 2001; Pinyopornpanish et al., 2020; Silpakit et al., 2015).
Depression
The Thai version of the Patient Health Questionnaire (PHQ-9), which consists of nine items, was used to examine the depressive symptoms of the CGs. The total number of possible scores ranged from 0 to 27. The scores of 0 to 6 was defined as “no depression,” 7 to 12 as “mild,” 13 to 18 as “moderate,” and 19 to 27 as “severe” (Lotrakul et al., 2008).
NPS
The Neuropsychiatric Inventory Questionnaire (NPI-Q), which consists of 12 NPS, was used to measure the BPSD. These 12 NPS are: delusions, hallucinations, agitation/aggression, depression/dysphoria, anxiety, euphoria/elation, apathy/indifference, disinhibition, irritability/lability, aberrant motor behavior, sleep/nighttime behavioral disturbances, and appetite/eating abnormalities. The questionnaire focused on the severity and distress of each symptom. The total NPI-Q distress scores ranged from 0 to 60 (Hemrunrojn, 2011; Kaufer et al., 2000), which was rated by the primary CG.
Functional Independence of the PwD
Barthel’s Index (BI) was used to measure the functional independence of the PwD. Each of the 10 items was scored based on their functional performance as: inability, need for help, and independence. The total scores ranged from 0 to 100, with a lower score indicating a decreased functional ability. Functional ability was divided into five levels, with scores of 80 to 100 as “independent,” 60 to 79 as “minimally dependent,” 40 to 59 as “partially dependent,” 20 to 39 as “very dependent,” and 0 to 19 as “totally dependent” (Mahoney & Barthel, 1965; Yi et al., 2020).
CGs’ Concerns
Based on previous studies, the authors developed the questionnaire to assess the CGs’ concerns about the COVID-19 pandemic (Borelli et al., 2021; Mahoney & Barthel, 1965; Yi et al., 2020). The questionnaire asked questions regarding the CGs’ daily lives, their access to healthcare services, their COVID vaccination status, and their self-care throughout the pandemic.
Socio-Demographic Characteristics of the CGs and PwD
Details on the socio-demographics of both the CGs and PwDs were gathered, including age, gender, marital status, education, comorbidities, relationship with PwD, occupations, self-perceived income, duration of caregiving, care experience, and care training. In this study, the stage of dementia was determined based on the functional independence of the PwD using BI, in which PwD who could perform all indices without help, or who needed help in some indices, or who needed help in all indices were classed as having mild, moderate, or severe dependence, respectively.
The primary outcomes were CG burden and the CGs’ self-perceived change in CG burden and depression, comparing between before and during the COVID-19 pandemic. The secondary outcomes were the factors associated with the CG burden, depression, CGs’ concerns about COVID-19, NPS, and functional independence of the PwD.
Statistical Analyses
SPSS version 18.0 (SPSS Inc., PASW Statistics for Windows, Chicago, IL, USA) was used for the statistical analysis. Descriptive analysis results were reported as the mean, median, and standard deviation (SD), and categorical data were reported as frequency and percentages. The independent t-test, Pearson correlation, non-parametric test, Mann–Whitney U-test, and Wilcoxon Signed Ranks test were used to analyze the continuous data depending on the distribution of the data. The Chi-square test was used for the categorical data. The researchers performed multivariate linear regression analysis to evaluate the associations between the CG burden and related variables. A p-value <.05 indicated statistical significance.
Results
The characteristics of the primary CGs and PwD are shown in Table 1. Regarding the CGs, 103 (76.3%) were women, and the mean (SD) age was 54.2 (10.7) years old. In 72 cases (53.3%), the CGs were unmarried; 79.3% were the patients’ children; and 80.7% had a bachelor’s degree or above in education. Also, 91 CGs (67.4%) perceived that they had enough income. In terms of health, 42% of CGs had no underlying diseases. However, the most common underlying diseases among CGs were hypertension (18.5%), hyperlipidemia (17.8%), and knee osteoarthritis (11.9%). Sixty CGs (44.4%) spent at least 12 hours per day caring for the PwD, and 72 CGS (53.3%) had looked after the PwD for at least 48 months. Regarding the previous experience with PwD care, most CGs (88.9%) had no experience, and 80.3% had never attended a CG training program. In terms of the PwD, 100 PwD (74%) were women with a mean (SD) age of 81.7 (7.9) years old. About 69 PwD (51.1%) were married, and 62 (45.9%) had graduated from primary school. In 73 cases (54.1%), the duration of the dementia diagnosis ranged from 1 to 5 years, and the majority of dementia stages were moderate in 67 cases (49.6%).
Demographic Characteristics of the CGs and PwD (n = 135).

Note. CG = caregiver; PwD = people with dementia; N = number; SD = standard deviation.
The mean (SD) ZBI-12 score was 14.9 (8.7) during the COVID-19 pandemic. About 52 CGs (38.5%) were defined as having a mild to moderate burden, and 36.3% CGs had none or a mild burden. The mean (SD) of the PHQ-9 score was 4.87 (4.8), while 95 CGs (70.4%) had no depression and 27 CGs (20%) had mild depression. When comparing the self-perceived changes between before and during the COVID-19 pandemic, the majority of CGs reported an increased CG burden and depression with 48 CGs (35.6%) experiencing “increased burden,” 25 (18.5%) “strongly increased burden,” 57 (42.2%) “increased depression,” and 56 (41.5%) “strongly increased depression.”
Prior to the pandemic, the mean (SD) of the NPI-Q total score to evaluate 12 symptoms for the PwD was 12.4 (12.6), with severity of the symptoms at 6.6 (5.5), and distress of the symptoms at 6.2 (7.3). There was an increase in the mean (SD) total score of NPI-Q during the pandemic at 15.6 (15.7), with severity of the symptoms of 7.5 (6.9), and distress of the symptoms of 8.2 (9.0).
Regarding the functional abilities of the PwD, the mean (SD) scores of the Barthel’s Index declined from before the COVID-19 pandemic compared to during the pandemic by 5 (11) (95% CI [−0.27, 0.91]). About 50.4% of CGs perceived that PwD had independent functional status before COVID-19, whereas 20.7% perceived they had minimal functional independence. As shown in Table 2, the scores for the PwD’s dependent status increased, and their functional ability decreased during COVID-19. Furthermore, as shown in Table 3, the change in the PwD’s NPS and functional ability before and during the COVID-19 pandemic demonstrated statistical significance.
Comparison of the Functional Ability of the PwD Reported by CGs Between Before and During the COVID-19 Pandemic.

Note. CG = caregiver; PwD = people with dementia.
Comparison of the PwD’s NPI-Q Score and Functional Ability Between Before and During the COVID-19 Pandemic (n = 135).

Note. CG = caregiver; PwD = people with dementia; SD = standard deviation; NPI-Q = neuropsychiatric inventory questionnaire.
In term of the COVID-19-related aspects of CGs, self-concern, healthcare accessibility, routine daily lives, and concern about COVID vaccination, are shown in Table 4. It can be seen that 86.7% of CGs reported they had enough self-care protection facilities, and 79.3% reported receiving adequate COVID-19 information updates, while the most common concerns among the CGs were the high infection rate and the treatment if the CGs or PwD were infected. In terms of healthcare accessibility factors, more than half of the CGs (51.9%) experienced difficulties receiving routine follow-up care with multiple causes, including PwD immobility (25.2%) and a long distance between their residence and hospital (14.8%). Furthermore, approximately two-thirds of PwD used telemedicine services during the pandemic. Only 26.7% of CGs reported loneliness during the COVID-19 outbreak, although more than 60% of CGs were living under the policy of social restriction. Also, 70 CGs (51.9%) had registered for the COVID vaccine using mobile applications, while 21.5% did so at healthcare units. A minority of the CGs had rejected the COVID vaccine due to concerns about the potential side effects of the vaccine.
COVID-19-Related Concerns Variables (n = 135).
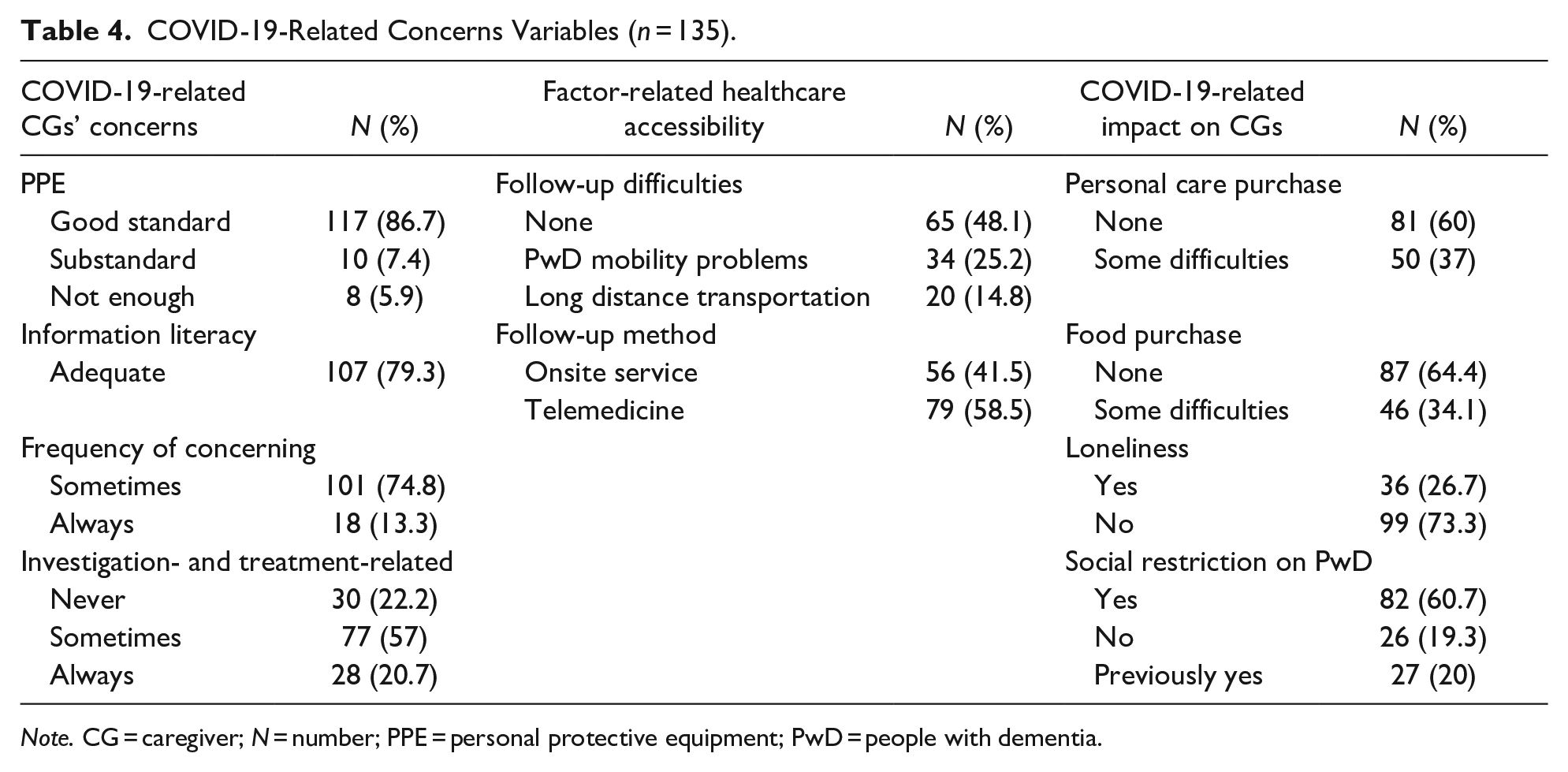
Note. CG = caregiver; N = number; PPE = personal protective equipment; PwD = people with dementia.
As shown in Table 5, the multiple logistic regression analysis showed that a high CG burden was significantly associated with having a higher level of education (p = .020), the incidence of family conflict (p = .004), depression (PHQ-9) (p < .001), and a high score in the NPS (NPI-Q) (p = .002) during the COVID-19 pandemic. There was no significant association between CG burden and COVID-19-related concerns.
Multiple Linear Regression Analysis of the CG-Burden-Related Factors in the CGs of PwD During the COVID-19 Pandemic (n = 135).

Note. CG = caregiver; PwD = people with dementia; SE = standard error; CI = confidence interval; PHQ-9 = 9-item Patient Health Questionnaire NPI-Q = Neuropsychiatric Inventory Questionnaire.
p < .05.
Discussion
This cross-sectional study evaluated the impact of the COVID-19 pandemic on PwD and their CGs in multiple dimensions, including CG burden and depression, PwD’s NPS and functional ability, and COVID-19-related concerns. The results of this study revealed a high CG burden, a high prevalence of depression in CGs, the development of NPS and functional dependency in PwD, and the CG-burden-related factors during the COVID-19 outbreak. The findings are in accordance with previous reports of a rising CG burden and worsening NPS during the pandemic (Borelli et al., 2021; Cohen et al., 2020; Tsapanou et al., 2021; Yuan et al., 2022). In this study, the authors showed the association between CG burden and related factors, including CG depression, a high level of CG education, conflict between the CGs and the PwD, and a high score for NPS. The level of education in this study corresponded with the average education year in Thai population in Bangkok, where the study was conducted (National Statistical Office, Thailand, 2021; Sittironnarit et al., 2020). The CGs’ background characteristics revealed a high level of education and the common presence of family conflict, which were reported in association with the CG’s burden. The high educational level of CGs was significantly associated with the CG burden, probably because CGs with higher education usually had more demanding jobs, which could be more burdensome when combined with caring for the PwD (Rosdinom et al., 2013). CGs’ perceptions of their burden and mental health were influenced by their relationship with the PwD through family conflict (Strawbridge & Wallhagen, 1991). A previous study reported a high incidence of depression in CGs during the COVID-19 outbreak, which might be a result of the intensity of caregiving, the feeling of loneliness, and the level of the burden they felt and experienced (Otobe et al., 2022). There was no association found between loneliness and depression in this study, which might differ from other studies (Sepúlveda-Loyola et al., 2020). This may be due to the fact that depression has a variety of etiologies, including increasing household responsibilities, financial problems (Ibáñez et al., 2021), personal health concerns, their perspective on depression, their capability to handle the situation (Messina et al., 2022), and social support (Losada-Baltar et al., 2022; Messina et al., 2022). The Ministry of Public Health takes mental health very seriously and their policy related to the mental health support system for primary healthcare in Thailand was for village health volunteers to survey and develop initial protocols to support people in their community in order to reduce the rate of depression during COVID-19 (Institute for Population and Social Research, Thailand, 2022).
The author surveyed the PwD-related factors, showing there was a high functional dependency and high prevalence of NPS. Previous studies found a correlation between PwD-related factors and CG burden (Borelli et al., 2021; Manini et al., 2021; Soysal et al., 2022). There are many causes related to NPS, such as a lack of social interactions, physical activities, and the closing of outpatient programs. Therefore, functional dependency and NPS affected CGs throughout the prolonged lockdown period; however, some studies revealed that CG burden may have had an impact on the CGs’ NPS reporting. The authors found that PwD tended to have a more dependent functional status, which could make them lose their ability to take care of themselves, resulting in higher physical resistance requirements and consequently an increased CG burden (Tsapanou et al., 2021).
The support systems, including family, community, social support, public utilities, government assistance, the healthcare system, and caregiver knowledge training might be associated with CG burden. A previous study revealed that social restriction policies decreased social interaction, limited non-pharmacological support, and restricted physical activities, which reduced the quality of care and increased stress in primary CGs (Borelli et al., 2021). Several research studies have found that a comprehensive family support programs and social support systems can reduce caregiver burden (Cravello et al., 2021; Institute for Population and Social Research, Thailand, 2022; Lai et al., 2020). National policies supported a campaign to establish a social support system and telemedicine to improve the resilience and well-being of both care recipients and CGs at home under the context of the need for social distancing caused by the pandemic. Consequently, this is why CG burden may not have been associated with support system factors in this study.
This study has several strengths to highlight. Beginning with this study, CG burden-related factors were established in a multidimensional survey, including physical, mental, and social aspects. The authors also assessed health literacy about the COVID-19 pandemic and factors influencing healthcare accessibility during the COVID-19 outbreak. Because all the PwD were identified by specialists, their characteristics were also highly reliable. Finally, there was no missing data due to the use of a well-organized online and face-to-face questionnaire.
There are also some limitations of the study to note, including the relatively small sample size. Also, the study was a cross-sectional study, which means that there was a risk of recall bias, which might have affected some questions that compared situations prior to and during the pandemic. However, the researchers emphasized that before beginning the questionnaire, the study participants should recall their situations in the pre-epidemic period as opposed to their current situation with the highest epidemic. Moreover, there was no causal relationship between the COVID-19 outbreak and CG burden-related factors. Also, some notable characteristics of CGs might not be generalizable, such as a high level of education and good financial status. Additionally, there was the possibility of selection bias because COVID-19 resulted in certain participants not being invited to participate in the study. Thus, the researchers extended the data collection time to gather more data from participants who were not able to visit the hospital at the time.
Conclusions
The study reveals the worsening mental health and increasing burden in CG, as well as the functional deterioration and higher NPS in PwD during the COVID-19 pandemic. This is important knowledge in order to initiate a further intervention aimed at reducing the incidence of CG burden during the COVID-19 outbreak or in the event of a future healthcare crisis. Modifiable factors should be identified in order to reduce the burden and improve the quality of care for PwD. Our results showed that caregivers are already grappling with rising stress levels caused by the pandemic. Additionally, the authors suggest providing social intervention and healthcare services, such as telemedicine and family interventions, and evaluating their effectiveness in preventing the adverse effects on PwD and CGs in particularly unusual situations.
Footnotes
Acknowledgements
The authors are extremely grateful to Mrs. Angkana Jongsawadipatana, Miss Rinrada Preedachitkul, Miss Nerisa Thonsri and all the staff members of the Geriatric Clinic, Siriraj Hospital, for their kind collaboration during this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Committee
The Siriraj Institutional Review Board (SIRB) of the Faculty of Medicine Siriraj Hospital, Mahidol University, Thailand. The protocol number is 621/2564(IRB3) COA No. Si 677/2021.