
Abstract
This study examined relationships among caregiver burden, depressive symptoms, and key processes related to psychological flexibility (experiential avoidance, cognitive fusion, values-driven actions, and mindfulness) in 157 family caregivers of individuals with dementia in the United States. Path analyses were used. Participants’ mean age was 59.5 years, ranging between 24 and 87 years. The model fit indices indicated excellent fit to the data. Caregiver burden had a direct effect on depressive symptoms (51.6 % of the total effect), while indirect effects accounted for 48.4%. The largest indirect effect was through values-driven action (14.6% of the total effect), followed by the paths through cognitive fusion → experiential avoidance (13.5%) and through mindfulness → cognitive fusion → experiential avoidance (8.7%). Targeting these key processes related to psychological flexibility with interventions such as acceptance and commitment therapy may help reduce the negative impact of caregiver burden on depressive symptoms in these caregivers.
• This study highlights the mediating role of values-driven actions, as well as cognitive fusion and experiential avoidance, in linking caregiver burden to depressive symptoms. • It reveals how mindfulness indirectly influences depressive symptoms through cognitive fusion and experiential avoidance, underscoring multi-step pathways.
• The results emphasize the importance of addressing processes related to psychological flexibility in family caregivers of people with dementia, which may alleviate the negative impact of caregiving burden on depressive symptoms. • Practitioners may develop targeted programs to prevent or reduce depressive symptoms by using psychological flexibility strategies.What this paper adds
Applications of study findings
Introduction
Family caregiving for individuals with Alzheimer’s disease and related dementias (ADRD) is an inherently complex and demanding role, often leading to significant caregiver burden and depressive symptoms (Harris et al., 2021). Caregiver burden refers to the extent to which caregivers perceive their caregiving responsibilities as negatively impacting various aspects of their lives (Zarit et al., 1986). Research indicates that between 36% and 89% of family caregivers of individuals with ADRD report caregiver burden, with a pooled prevalence of approximately 63% (Collins & Kishita, 2020). Given the demanding nature of the role, it is common for family caregivers to experience some level of burden throughout their caregiving journey (Cartaxo et al., 2023).
When caregiver burden becomes overwhelming and persistent, it poses a significant risk for depressive symptoms among family caregivers of individuals with ADRD (Del-Pino-Casado et al., 2019). An estimated 34% of family caregivers experience depressive symptoms, which can negatively affect their health and the quality of care they provide (Collins & Kishita, 2020; Guterman et al., 2019). Some studies have reported higher prevalence rates of depressive symptoms in these family caregivers, with estimates as high as 83% (Huang, 2022).
Numerous studies have explored predictors of caregiver burden and depressive symptoms, including care intensity, the presence and severity of behavioral and psychological symptoms of dementia (BPSD), and caregiver demographics such as gender (Cartaxo et al., 2023; Collins & Kishita, 2020). However, many of these factors are hard or impossible to prevent or modify and depend on disease progression, caregiving situations, and external support resources (Huang, 2022). Additionally, caregivers’ perceptions of caregiving demands can vary, even in similar caregiving situations (Liu et al., 2020; Pinyopornpanish et al., 2021).
Some studies suggest that objective caregiving stressors, such as the presence and intensity of BPSD, might be less important or less directly related to psychological distress, such as depressive symptoms, than individual caregivers’ perceptions of burden (Kishita et al., 2020; Pinyopornpanish et al., 2021). Fewer studies, however, have explored psychological processes underlying the relationship between caregiver burden and depressive symptoms in family caregivers of individuals with ADRD. Thus, understanding the relationship between caregiver burden and depressive symptoms while considering psychological dimensions that may mediate this relationship is crucial, as it could suggest interventions that may prevent those with caregiver burden from developing or worsening depressive symptoms.
One promising model for understanding these relationships is the psychological flexibility model (Hayes et al., 2012b). Psychological flexibility is defined as the ability to be open and present to thoughts and emotions, including those that are distressing, while engaging in values-driven actions (Cherry et al., 2021). Psychological inflexibility, its counterpart, involves avoidance or suppression of unwanted internal experiences, attachment to rigid thought patterns, and failure to act according to personal values (Cherry et al., 2021).
Key processes within the psychological flexibility model, such as experiential avoidance, cognitive fusion, values-driven action, and mindfulness, may mediate the relationship between caregiver burden and depressive symptoms (Barrera-Caballero et al., 2023; Kishita et al., 2023; Tolea et al., 2023; Trompetter et al., 2013). Experiential avoidance refers to efforts to control or suppress unwanted thoughts and emotions (Hayes et al., 1996). Cognitive fusion occurs when individuals become so entangled with their thoughts (Hayes et al., 2012b). Values-driven action refers to clarifying personal values and engaging in value-consistent actions, even in the presence of difficult thoughts and emotions (Hayes et al., 2012b; Trompetter et al., 2013). Mindfulness is the awareness that arises by paying purposeful attention to the present moment and observing thoughts and emotions without judgment (Kabat-Zinn, 2003). Mindfulness is embedded in the psychological flexibility model by fostering disengagement from cognitive fusion and experiential avoidance and promoting values-driven actions (Hayes et al., 2012a).
Studies across various populations support the associations among these key processes and depressive symptoms, including the link between high experiential avoidance and low values-driven actions with severe depressive symptoms (Cookson et al., 2020; Gupta & Sinha, 2023; McCluskey et al., 2022; Tunç et al., 2023). Cognitive fusion is often thought to precede and contribute to experiential avoidance, though the relationship can be bidirectional (Cookson et al., 2020). Some studies suggest that relationship between mindfulness and psychological distress, such as depressive symptoms and anxiety, is mediated by experiential avoidance (Gupta & Sinha, 2023; McCluskey et al., 2022).
These processes related to psychological flexibility are particularly relevant to family caregivers of individuals with ADRD, who frequently experience burden (Collins & Kishita, 2020). For example, experiential avoidance may occur when caregivers attempt to avoid or suppress unwanted thoughts and emotions that arise in day-to-day caregiving situations, such as feelings of frustration and anger (Chan et al., 2010). While such avoidance may provide temporary relief, it can exacerbate distress and contribute to depressive symptoms (Kishita et al., 2020, 2023). Cognitive fusion may amplify feelings of burden by leading caregivers to over-identify with distressing thoughts, such as guilt or inadequacy (Gallego-Alberto et al., 2022). This rigid attachment to negative beliefs—such as “I’m failing as a caregiver” or “This will never improve”—can trap caregivers in a cycle of hopelessness and self-criticism, intensifying their depressive symptoms (Barrera-Caballero et al., 2023). Caregivers with low mindfulness may find it difficult to stay present and open to their caregiving experiences without judgment, leading to overwhelm and heightened depression (Tolea et al., 2023). Moreover, caregivers experiencing burden may engage less in other valued aspects of life, such as self-care and social relationships, which may result in emotional exhaustion, a sense of purposelessness, and an increased risk of depression (Fauth et al., 2024; Tatangelo et al., 2018).
While some studies have explored these processes as mediators, they often examined only one or two, such as experiential avoidance either in isolation or alongside cognitive fusion, and did not investigate the complex interplay of multiple processes (Barrera-Caballero et al., 2023; Kishita et al., 2023). Moreover, much existing research used samples from countries with relatively homogenous populations such as Spain and Japan, with limited exploration of more racially diverse caregivers in countries like the United States (Barrera-Caballero et al., 2023; Kishita et al., 2023).
Few studies have examined the relationships among multiple psychological flexibility processes, caregiver burden, and depressive symptoms in family caregivers of individuals with ADRD. Thus, this study aimed to address these gaps by using path analyses to examine relationships among caregiver burden, depressive symptoms, and key processes related to psychological flexibility, including experiential avoidance, cognitive fusion, values-driven actions, and mindfulness in a sample of caregivers in the United States. The conceptual model (Figure 1) used for path analyses was informed by previous studies and the psychological flexibility model described above. Our conceptual model and hypotheses are detailed in the Methods section. Conceptual research model. Note. AAQ-II = Acceptance and Action Questionnaire-II; CFQ-7 = Cognitive Fusion Questionnaire-7; ELS-9 = Engaged Living Scale-9; FFMQ-SF = Five Facet Mindfulness Questionnaire-Short Form; PHQ-9 = Patient Health Questionnaire-9; ZBI-12 = Zarit Burden Interview-12.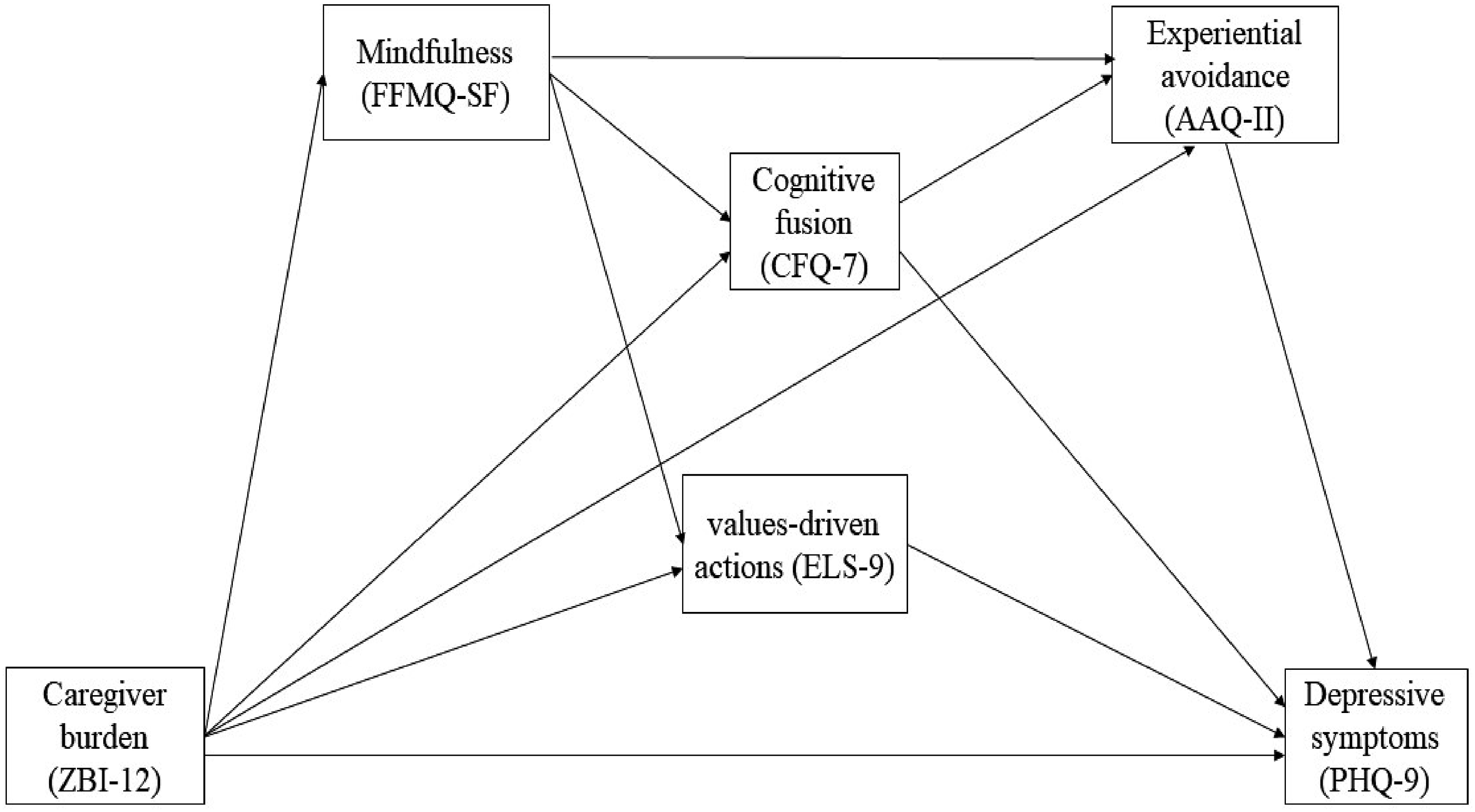
Methods
Design and Participants
This study employed a cross-sectional design to examine the relationships among caregiver burden, depressive symptoms, and key processes related to psychological flexibility in family caregivers of individuals with ADRD. Participants were 157 family caregivers (aged 18 years or older) of individuals with ADRD, who were recruited across the United States. A flyer containing the research team’s contact information and survey link was shared with Area Agencies on Aging, adult day services, and support groups for caregivers of individuals with ADRD, including those serving specific racial/ethnic communities in areas with diverse populations.
Procedures
Participants completed an online survey created in Qualtrics, which included demographic and caregiving-related questions along with the measures outlined under “Measures.” Participants received $35 via the ClinCard, a reloadable debit card used for research participant compensation, after completing the survey and providing a valid mailing address. Data collection for 157 participants was conducted over 2 months in early 2024. Ethical approval was obtained from the Institutional Review Board at the University of Alabama at Birmingham (IRB-300012390), and all participants provided informed consent before accessing the survey questions.
Measures
Caregiver Burden
Caregiver burden was assessed using the 12-item Zarit Burden Interview (ZBI-12; Bédard et al., 2001), a self-report questionnaire rated on a scale of 0 (never) to 4 (nearly always). Scores range from 0 to 48, with higher scores indicating greater caregiver burden (Bédard et al., 2001). Suggested cut-off points are: 0–9 (no or little burden), 10–19 (mild to moderate burden), and 20–48 (high burden; Bédard et al., 2001). The ZBI-12 has demonstrated good internal consistency, as well as convergent and discriminant validity, in caregivers of individuals with ADRD (Bédard et al., 2001).
Depressive Symptoms
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9; (Kroenke et al., 2001), a nine-item self-report questionnaire that assesses the severity of depressive symptoms over the past 2 weeks rated on a scale of 0 (not at all) to 3 (nearly every day). Scores range from 0 to 27, with higher scores indicating more severe depressive symptoms. Suggested cut-off points are: 0–4 (no depressive symptoms), 5–9 (mild depressive symptoms), 10–14 (moderate depressive symptoms), 15–19 (moderately severe depressive symptoms), and 20–27 (severe depressive symptoms). The PHQ-9 has shown acceptable diagnostic properties for detecting major depressive disorder with cut-off scores between 8 and 11 (Manea et al., 2012). It has demonstrated good internal consistency and test-retest reliability, as well as criterion validity and construct validity (Kroenke et al., 2001).
Processes Related to Psychological Flexibility
Experiential avoidance was measured using the Acceptance and Action Questionnaire-II (AAQ-II; Bond et al., 2011), a seven-item self-report questionnaire rated on a scale of 1 (never true) to 7 (always true). Scores range from 7 to 49, with higher scores indicating greater experiential avoidance. The AAQ-II has demonstrated good internal consistency and test-retest reliability, as well as concurrent, predictive, and discriminant validity (Bond et al., 2011).
Cognitive fusion was assessed using the seven-item Cognitive Fusion Questionnaire (CFQ-7; Gillanders et al., 2014), rated on a scale of 1 (never true) to 7 (always true). Scores range from 7 to 49, with higher scores indicating greater cognitive fusion. The CFQ-7 has shown good internal consistency and test-retest reliability, as well as concurrent validity and discriminant validity (Gillanders et al., 2014).
Mindfulness was measured using the Five Facet Mindfulness Questionnaire-Short Form (FFMQ-SF), a 24-item self-report questionnaire evaluating five facets of mindfulness: observing, describing, acting with awareness, non-judgment of inner experiences, and nonreactivity to inner experiences (Bohlmeijer et al., 2011). Responses are rated on a scale of 1 (never or very rarely true) to 5 (very often or always true), with total scores ranging from 24 to 120. Higher scores indicate greater mindfulness, and the FFMQ-SF has demonstrated good internal consistency and construct validity (Bohlmeijer et al., 2011).
Values-driven action was assessed using the Engaged Living Scale-9 (ELS-9; Trindade et al., 2015), a nine-item self-report questionnaire that measures clarity of and engagement with personal values on a scale of 1 (completely disagree) to 5 (completely agree). Total scores range from 9 to 45, with higher scores indicating greater clarity and engagement with personal values. The ELS-9 has demonstrated good internal consistency and construct validity (Trindade et al., 2015).
Conceptual Model
Figure 1 presents the conceptual model. We hypothesized that three psychological flexibility processes (AAQ-II, CFQ-7, and ELS-9) would partially mediate the relationship between caregiver burden (ZBI-12) and depressive symptoms (PHQ-9). In other words, we anticipated that higher caregiver burden would be both directly and indirectly associated with more severe depressive symptoms through its association with each of these processes (i.e., path: ZBI-12 → AAQ-II → PHQ-9; path: ZBI-12 → ELS-9 → PHQ-9; path: ZBI-12 → CFQ-7 → PHQ-9).
Additionally, we hypothesized that the relationship between caregiver burden and depressive symptoms might be mediated by a pathway in which high cognitive fusion (CFQ-7) is associated with greater experiential avoidance (AAQ-II), which in turn contributes to more severe depressive symptoms (i.e., path: ZBI-12 → CFQ-7 → AAQ-II → PHQ-9). In other words, when caregivers feel burdened and become overly fused with their thoughts about that burden (cognitive fusion), their tendency to avoid those difficult experiences (experiential avoidance) increases, ultimately leading to more severe depressive symptoms.
Furthermore, we hypothesized that mindfulness (FFMQ-SF) would mediate the relationship between caregiver burden and depressive symptoms via each of the three processes of psychological flexibility (AAQ-II, CFQ-7, and ELS-9) on the paths mentioned above (i.e., path: ZBI-12 → FFMQ-SF → AAQ-II → PHQ-9; path: ZBI-12 → FFMQ-SF → ELS-9 → PHQ-9; path: ZBI-12 → FFMQ-SF → CFQ-7 → PHQ-9; path: ZBI-12 → FFMQ-SF → CFQ-7 → AAQ-II → PHQ-9). For instance, if caregivers become more aware of their thoughts and feelings without being overwhelmed, it may reduce their tendency to avoid difficult experiences (i.e., less experiential avoidance). Similarly, mindfulness may help caregivers to engage in actions aligned with their personal values (i.e., increased values-driven action) despite caregiving responsibilities or to distance themselves from unhelpful caregiving-related thoughts (i.e., reduced cognitive fusion) that may lead to less experiential avoidance. These processes, in turn, may alleviate the negative impact of caregiver burden on depressive symptoms.
Data Analysis
Descriptive statistics were used to examine the characteristics of the participants. Skewness (< 2.0) and kurtosis (< 7.0) of the variables were checked to assess whether these variables violated the normality assumption (Curran et al., 1996) and to determine their suitability for path analyses. The six variables used in path analyses had skewness values below 2.0 and kurtosis values below 7.0, indicating that they did not violate the normality assumption for path analyses. The path analyses were then used to test the hypothesized relationships among caregiver burden, depressive symptoms, and key processes related to psychological flexibility.
Model fit of the path analyses was examined to assess whether the hypothetical model (Figure 1) adequately fit the data. The chi-square test (χ2), root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker-Lewis Index (TLI), and standardized root mean square residual (SRMR) were utilized. Criteria for acceptable model fit included χ2 p > .05, CFI and TLI > .95, RMSEA < .08, and SRMR < .08 (Browne & Cudeck, 1993; Hu & Bentler, 1999; Kline, 2023). Model parameters, including standardized coefficients and 95% confidence intervals (CI), were estimated using maximum likelihood estimation. Bootstrapping with 1,000 samples was used to accurately estimate the significance of the indirect effects of the path analysis variables between caregiver burden and depressive symptoms (Preacher & Hayes, 2008). SAS version 9.4 was used for data management and descriptive statistics, and Mplus version 8.8 was utilized to conduct the path analyses.
Results
Characteristics of the Participants
Characteristics of Participants (N = 157).
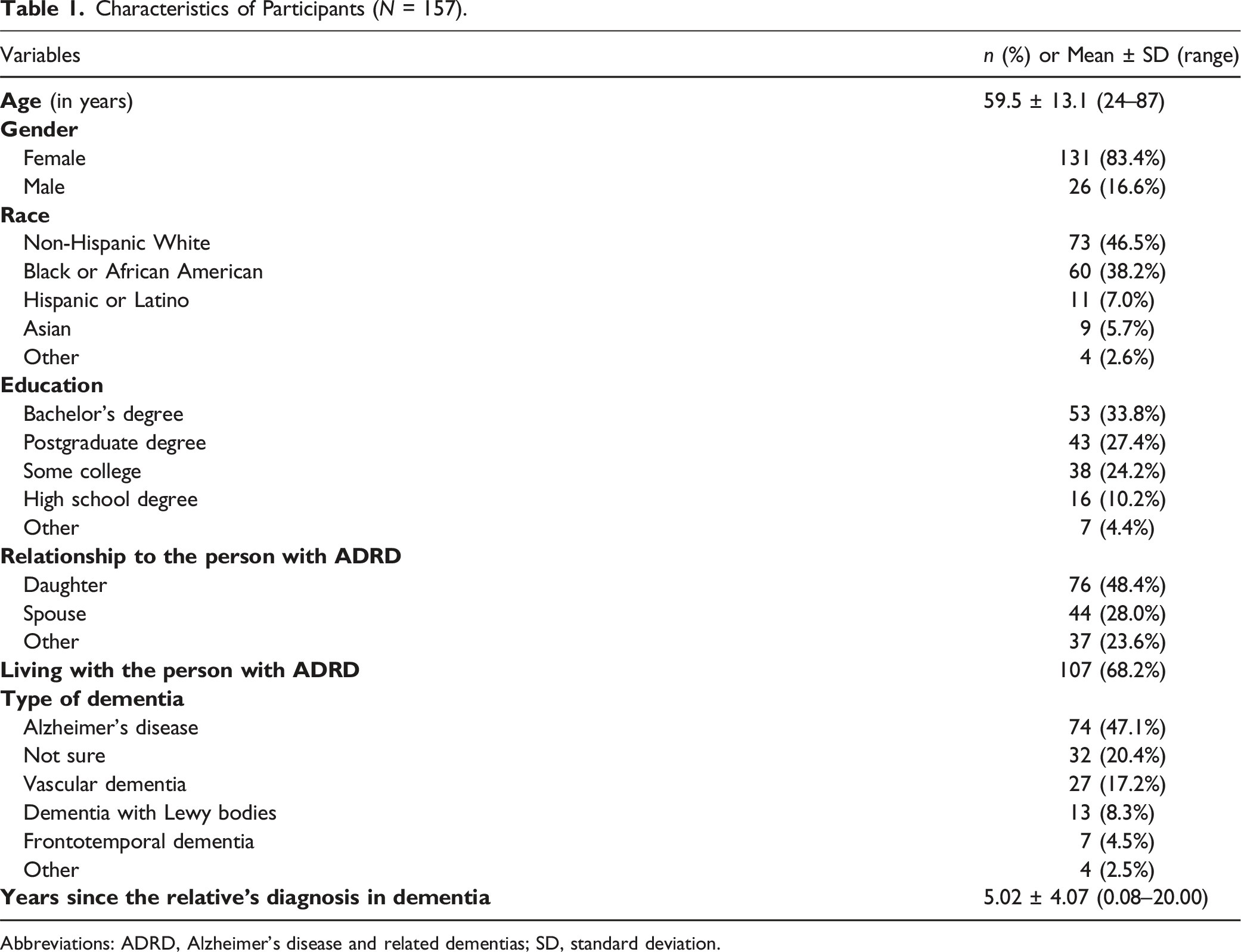
Abbreviations: ADRD, Alzheimer’s disease and related dementias; SD, standard deviation.
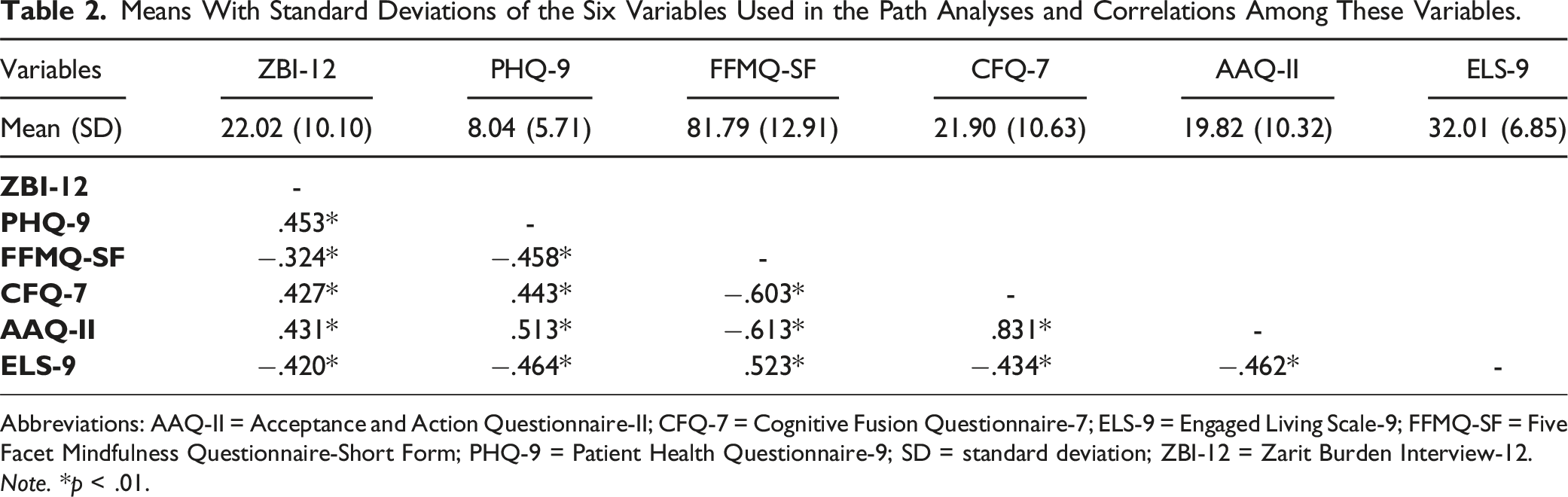
Means With Standard Deviations of the Six Variables Used in the Path Analyses and Correlations Among These Variables.
Abbreviations: AAQ-II = Acceptance and Action Questionnaire-II; CFQ-7 = Cognitive Fusion Questionnaire-7; ELS-9 = Engaged Living Scale-9; FFMQ-SF = Five Facet Mindfulness Questionnaire-Short Form; PHQ-9 = Patient Health Questionnaire-9; SD = standard deviation; ZBI-12 = Zarit Burden Interview-12.
Note. *p < .01.
Correlations Among the Variables Used in the Model
Table 2 shows the results of correlational analyses among caregiver burden, depressive symptoms, and the four processes related to psychological flexibility. All variables were significantly correlated with each other (p < .01).
Model Fit
The conceptual model (Figure 1) presents excellent model fit values, including χ2[3] = 5.374 (p = .146), RMSEA = .071, CFI = .994, TLI = .972 and SRMR = .025. However, the direct path from cognitive fusion (CFQ-7) to depressive symptoms (PHQ-9; β = −.033, p > .05, 95% CI = −.131, .081) and the direct path from caregiver burden (ZBI-12) to experiential avoidance (AAQ-II; β = .079, p > .05, 95% CI = −.024, .183) were not statistically significant, so relevant paths in the conceptual model (i.e., path: ZBI-12 → CFQ-7 → PHQ-9, path: ZBI-12 → FFMQ-SF → CFQ-7 → PHQ-9, and path: ZBI-12 → AAQ-II → PHQ-9) were omitted from the final model to improve model fit.
The final model fit indices also indicated an excellent fit to the data (Figure 2). The chi-square test of model fit was non-significant (χ2[5] = 8.230, p = .144), indicating that the model does not significantly deviate from the observed data. The RMSEA was .064, which was less than or equal to .08, suggesting a close fit. The CFI and TLI values were .992 and .977, respectively, both exceeding the commonly accepted threshold of .95, indicating excellent fit. The SRMR was .031, further supporting a good model fit. Final structural equation model with standardized coefficients. Standardized coefficients were estimated by the maximum likelihood estimation. Note. AAQ-II = Acceptance and Action Questionnaire-II; CFQ-7 = Cognitive Fusion Questionnaire-7; ELS-9 = Engaged Living Scale-9; FFMQ-SF = Five Facet Mindfulness Questionnaire-Short Form; PHQ-9 = Patient Health Questionnaire-9; ZBI-12 = Zarit Burden Interview-12. Note. *p < .05.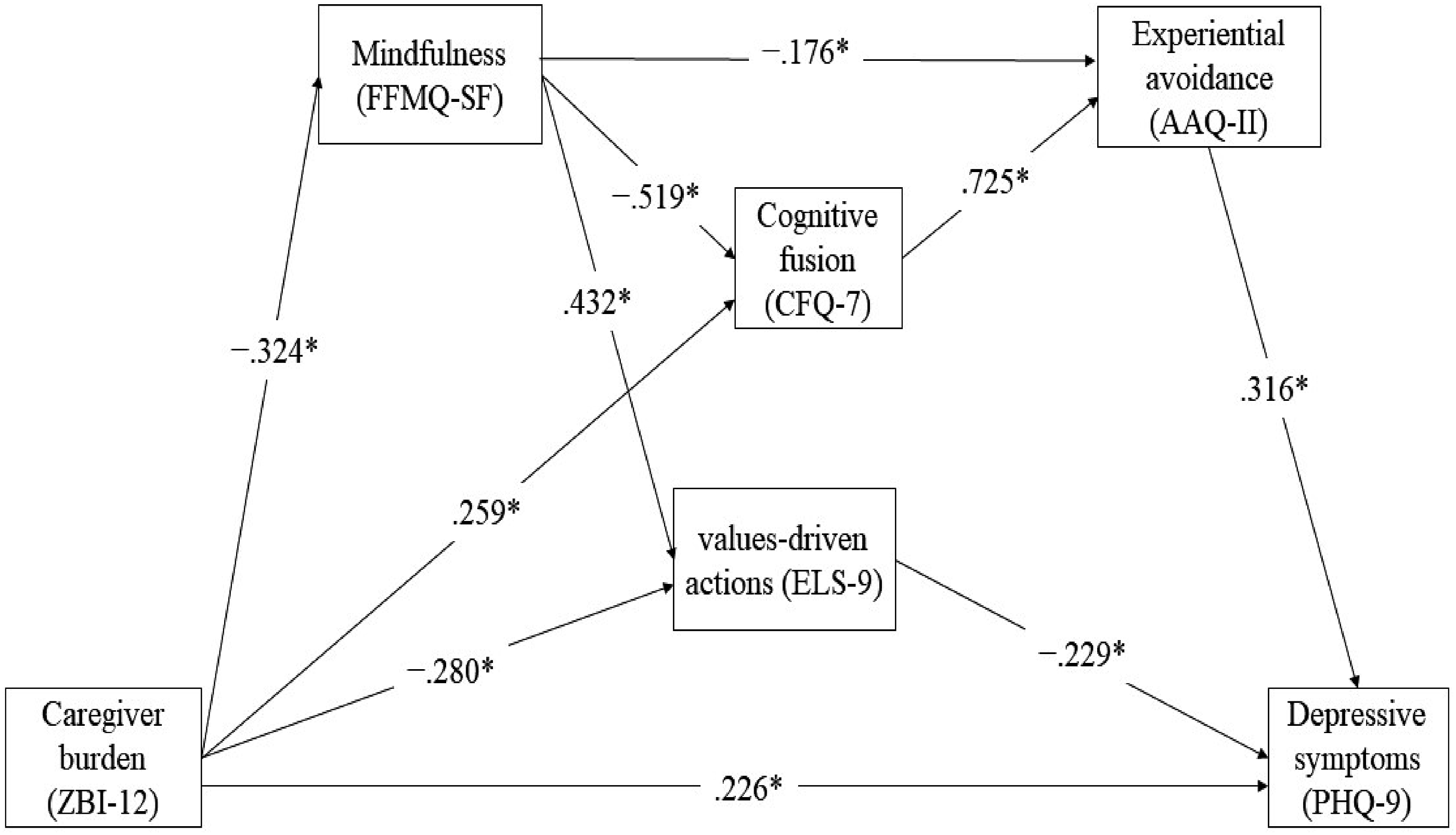
Findings of the Hypothesized Model
Standardized Path Coefficients With the 95% Confidence Interval for the Estimated Model.
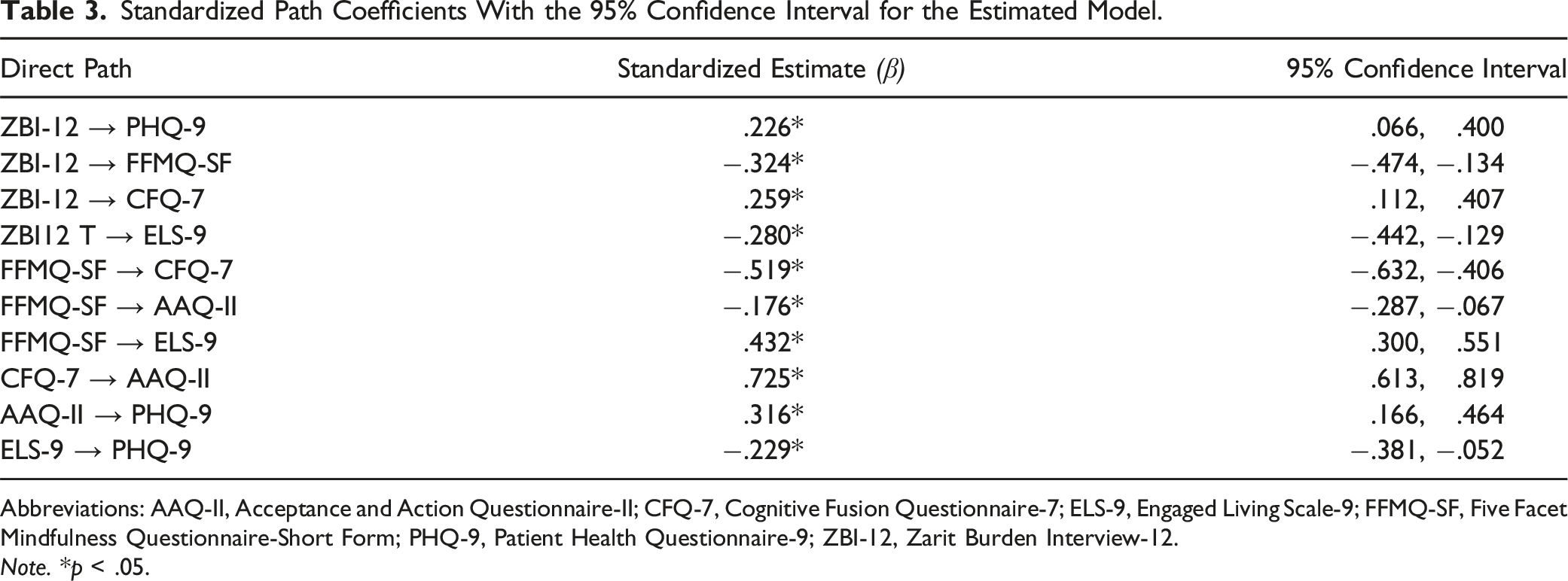
Abbreviations: AAQ-II, Acceptance and Action Questionnaire-II; CFQ-7, Cognitive Fusion Questionnaire-7; ELS-9, Engaged Living Scale-9; FFMQ-SF, Five Facet Mindfulness Questionnaire-Short Form; PHQ-9, Patient Health Questionnaire-9; ZBI-12, Zarit Burden Interview-12.
Note. *p < .05.
Indirect Effects Between Perceived Caregiver Burden (ZBI-12) and Depressive Symptoms (PHQ-9).
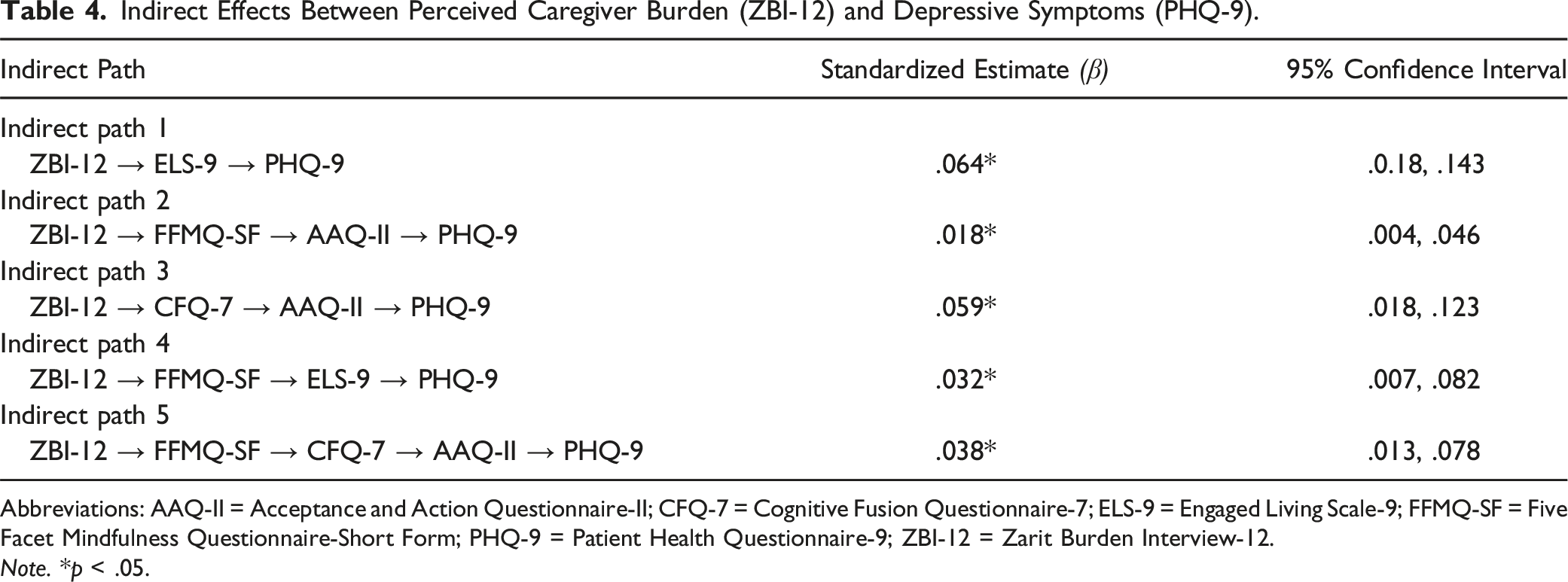
Abbreviations: AAQ-II = Acceptance and Action Questionnaire-II; CFQ-7 = Cognitive Fusion Questionnaire-7; ELS-9 = Engaged Living Scale-9; FFMQ-SF = Five Facet Mindfulness Questionnaire-Short Form; PHQ-9 = Patient Health Questionnaire-9; ZBI-12 = Zarit Burden Interview-12.
Note. *p < .05.
The standardized estimate (β) of the indirect path between caregiver burden (ZBI-12) and depressive symptoms (PHQ-9) through values-driven actions (ELS-9) was .064 (p < .05, 95% CI = .018, .143; indirect path 1 in Table 4). This estimate indicates that higher caregiver burden was associated with lower values-driven actions, which was associated with more severe depressive symptoms. Additionally, the standardized estimate (β) of the indirect path between caregiver burden (ZBI-12) and depressive symptoms (PHQ-9) through cognitive fusion (CFQ) → experiential avoidance (AAQ-II) was .059 (p < .05, 95% CI = .018, .123; indirect path 3 in Table 4). This suggests that higher caregiver burden was associated with higher cognitive fusion, which was related to increased experiential avoidance and, ultimately, more severe depressive symptoms.
The standardized estimate (β) of the indirect path between caregiver burden (ZBI-12) and depressive symptoms (PHQ-9) through mindfulness (FFMQ-SF) → experiential avoidance (AAQ-II) was .018 (p < .05, 95% CI = .004, .046; indirect path 2 in Table 4), through mindfulness (FFMQ-SF) → values-driven actions (ELS-9) was .032 (p < .05, 95% CI = .007, .082; indirect path 4 in Table 4), and through mindfulness (FFMQ-SF) → cognitive fusion (CFQ) → experiential avoidance (AAQ-II) was .038 (p < .05, 95% CI = .013, .078; indirect path 5 in Table 4). These findings indicate that higher caregiver burden was associated with lower mindfulness, which in turn was related to higher experiential avoidance and lower values-driven actions, both of which were associated with more severe depressive symptoms. Additionally, higher caregiver burden was associated with lower mindfulness, which was related to increased cognitive fusion; higher cognitive fusion, in turn, was associated with increased experiential avoidance, which was then related to more severe depressive symptoms.
Among the indirect effects (Table 4), the largest indirect effect was indirect path 1 (ZBI-12 → ELS-9 → PHQ-9), accounting for 14.6% of the total effect, followed by indirect path 3 (ZBI-12 → CFQ-7 → AAQ-II → PHQ-9) at 13.5%, indirect path 5 (ZBI-12 → FFMQ-SF → CFQ-7 → AAQ-II → PHQ-9) at 8.7%, indirect path 4 (ZBI-12 → FFMQ-SF → ELS-9 → PHQ-9) at 7.3%, and indirect path 2 (ZBI-12 → FFMQ-SF → AAQ-II → PHQ-9) at 4.1%.
Discussion
The present study examined the relationships among caregiver burden, depressive symptoms, and key processes related to psychological flexibility (i.e., experiential avoidance, cognitive fusion, values-driven action, and mindfulness) in 157 family caregivers of individuals with ADRD living in the United States. The study showed a direct effect of caregiver burden on depressive symptoms, which aligns with prior research that demonstrated this association (Del-Pino-Casado et al., 2019; Pinyopornpanish et al., 2021). More importantly, the study extends the literature by addressing multiple key processes related to psychological flexibility that may mediate this relationship.
As hypothesized, we found indirect effects of caregiver burden on depressive symptoms through its influence on values-driven actions, as well as through the pathway from cognitive fusion to experiential avoidance. The findings suggest that caregivers who remain engaged with their personal values despite the demands of caregiving are more likely to report less severe depressive symptoms. These findings are supported by previous research across various populations, including caregivers, that also identified relationships between low values-driven actions and more severe depressive symptoms (Fauth et al., 2024; Tunç et al., 2023). Furthermore, the results suggest that caregivers with higher caregiver burden are more likely to experience a higher degree of cognitive fusion and then more likely to avoid distressing caregiving-related thoughts that may exacerbate depressive symptoms. Cognitive fusion is often thought to precede and contribute to experiential avoidance, though recent studies suggest that the relationship may be bidirectional or even reversed (Cookson et al., 2020; Kishita et al., 2023). These differing findings could be due to variations in variables (such as using caregiver burden as the independent variable in the present study), measurement tools, countries, and populations across studies, warranting further investigation.
As hypothesized, the study also found that mindfulness, along with other key processes of psychological flexibility, played an important role in the relationship between caregiver burden and depressive symptoms. The findings showed indirect effects of caregiver burden on depressive symptoms through mindfulness, which influenced experiential avoidance, values-driven actions, and the pathway from cognitive fusion to experiential avoidance. These results are supported by the psychological flexibility model and previous studies, which have suggested that mindfulness may promote engagement in values-driven actions and disengagement from cognitive fusion and experiential avoidance (Gupta & Sinha, 2023; Hayes et al., 2012a; McCluskey et al., 2022). In other words, mindfulness may help caregivers create psychological distance from distressing thoughts, reduce their tendency to avoid difficult emotions, and engage in actions aligned with their personal values, thereby alleviating the negative impact of caregiver burden on depressive symptoms.
The present study found that the path from cognitive fusion to depressive symptoms and the path from caregiver burden to experiential avoidance were not statistically significant, so the relevant paths in the conceptual model were omitted from the final model. However, the path through cognitive fusion→ experiential avoidance was significant. These findings suggest that the relationship between caregiver burden and depressive symptoms may not be mediated by cognitive fusion or experiential avoidance individually, but by the combined pathway through cognitive fusion→ experiential avoidance. In other words, when caregivers feel burdened, they may initially become overly fused with their thoughts related to that burden, and then attempt to avoid or suppress these thoughts, which ultimately leads to depressive symptoms. Becoming overly fused with thoughts related to caregiver burden may not lead directly to depressive symptoms until caregivers make efforts to avoid or suppress these thoughts. Alternatively, caregivers may not attempt to avoid burden-related thoughts until they become so attached to these thought patterns (believing them as absolute truth), allowing them to rigidly dictate behaviors and emotions. As mentioned above, this warrants further investigation with a larger sample size in future studies.
Findings from the present study have important clinical and policy implications for supporting family caregivers of individuals with ADRD. The results highlight the importance of addressing psychological flexibility processes in caregiver support programs by helping caregivers develop skills to enhance psychological flexibility, which may alleviate the negative impact of caregiving burden on depressive symptoms. Acceptance and commitment therapy (ACT) specifically aims to promote psychological flexibility, and growing evidence suggests that ACT-based programs are feasible, acceptable, and beneficial for improving mental health outcomes among family caregivers of individuals with ADRD (e.g., Han et al., 2021; 2023). Findings from the present study provide a foundation for practitioners to develop targeted programs that teach caregivers strategies to step back from distressing thoughts and emotions related to caregiver burden, accept these experiences without avoidance or suppression, and engage in behaviors aligned with their core values. Integrating these ACT-based approaches into community and healthcare settings may help bridge the gap in accessible, evidence-based mental health services for caregivers.
Several limitations should be noted. The cross-sectional design limits the ability to make causal inferences, highlighting the need for longitudinal studies to clarify temporal relationships. Additionally, the sample size was relatively small, leading to insufficient statistical power. This study did not include objective caregiving stressors, such as BPSD, or caregivers’ sociodemographic characteristics, (e.g., economic stability and social and community support; Gaugler et al., 2023) as potential covariates to account for their potential confounding effects, primarily due to the limited sample size. Future research with a larger sample size and longitudinal data could address these factors for deeper insights. Furthermore, as this study was conducted in the U.S., the findings may not generalize to other cultural contexts (Knight & Sayegh, 2010). Future larger-scale studies may explore how psychological flexibility processes and the proposed model are influenced by cultural differences.
In conclusion, this study highlights the critical role of processes related to psychological flexibility in the relationship between caregiver burden and depressive symptoms in family caregivers of individuals with ADRD. Targeting these key processes related to psychological flexibility with interventions such as ACT may help reduce the negative impact of caregiver burden on depressive symptoms.
Footnotes
Acknowledgments
We sincerely thank all the study participants for generously contributing their time and effort. We are also grateful to the directors and staff of the Area Agencies on Aging and adult day programs serving individuals with dementia for helping distribute the study flyer to potential participants, with special recognition to Bill Zagorski for his assistance. Our heartfelt appreciation goes to the Alzheimer’s Association for their generous support of this research. We also acknowledge Donna Burnett from the Department of Occupational Therapy and Faye Suggs from the Office of Sponsored Programs at the University of Alabama at Birmingham for their outstanding administrative support in managing the research grant.
Author Contributions
Conceptualization: AH, IH, HKY; Methodology: AH, IH; Investigation: AH, JH; Formal analysis: IH; Resources: AH, IH, JMR; Data Curation: AH, IH, HKY, HKL; Visualization: AH, IH, HKL; Supervision: AH, IH; Project Administration: AH, IH, JH; Funding Acquisition: AH, HKY; Writing—original draft: AH, IH; Writing—review and editing: AH, IH, HKY, JH, HKL, JMR, YL, HYL, ESD.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Alzheimer’s Association Research Grant (AARG-21-846868).