
Abstract
The unpredictable spread of the COVID-19 pandemic, national lockdowns, and public health measures implemented in the Czech Republic had a negative effect on older adults’ mental health and loneliness. The 2,631 older adults in 2020 and 2,083 older adults in 2021 used in this study formed a nationally representative sample of the Survey of Health, Ageing and Retirement in Europe (SHARE). Almost every third older adult experienced feelings of loneliness in both stages of the COVID-19 outbreak. Loneliness increased in 2021 in those individuals who reported their physical health as poor, who felt nervous, sad or depressed, and who had ever left their home since the outbreak. According to age-related drivers of loneliness, feelings of loneliness were prevalent (40% vs. 45%) among younger retirees in both waves. In both data sets, declared feelings of sadness or depression were the strongest sustainable predictor of loneliness (2020 and 2021 models, OR = 3.69; 95% CI [2.90, 4.69] and OR = 2.55; [1.97, 3.30]). Being a woman and feeling nervous equated with a higher likelihood of feeling lonely compared to counterparts. Policy makers should therefore aim to carefully improve psychosocial and health-related consequences faced by this vulnerable population during the pandemic and beyond.
• Anticipated increase in loneliness during COVID-19 and the associated safety measures resulted in its experience by a third of the older adult population.
• Declared feelings of sadness or depression, nervousness, and gender were identified as the main risk factors affecting mental health in case of loneliness during the early and late stage of the COVID-19 pandemic in high-risk 50+ population.
• Most lonely older adults were typified by women who felt nervous, and experienced sadness or depression in the previous month.
• As a response to early and late COVID-19 outbreak, social institutions, health-care providers, gerontologists, and social workers should focus on facilitating meaningful social connections and ensuring support for social needs in order to reduce the short- and long-term negative health consequences of the pandemic in the high-risk 50+ population.
• Negative trend of increased level of loneliness in the high-risk 50+ population should be considered in future handling of the ongoing pandemic.
• Special focus should be addressed to women who felt nervous and experienced sadness or depression during the COVID-19 pandemic.
Introduction
Coronavirus disease (COVID-19) was first identified in December 2019 in Wuhan, Hubei Province, China (Phelan et al., 2020). However, following the rapid spread of the disease globally, COVID-19 was declared a pandemic on March 11, 2020 by the World Health Organization (WHO, 2020a).
Despite the evidence indicating that COVID-19 occurs across the life span, older adults (aged over 50 years) were recognized as a risk group in the pandemic (United Nations, 2020a). In response, many governments adopted lockdowns and social distancing safety measures to combat human-to-human transmission of the disease (Gupta et al., 2020; WHO, 2020b). In the Czech Republic, the State of Emergency, followed by a lockdown and social distancing measures, was first announced on March 12, 2020. With fast-growing numbers of people testing positive in vulnerable older adult populations, the restrictive measures were repeatedly updated and extended between March 12, 2020 and December 25, 2021 (Ministry of the Interior of the Czech Republic, 2020, see the timeline in Supplemental Appendix Figure A1). To date (February 20, 2023), out of 4,562,045 confirmed COVID-19 cases, 1,919,073 people were aged over 50, with 41,998 deaths reported in this population (Ministry of Health of the Czech Republic, 2023).
While public health safety measures showed positive effects regarding infection numbers (Atzendorf & Gruber, 2021; Vokó & Pitter, 2020), psychologists and mental health professionals suggest that COVID-19 safety measures followed by the sudden loss of personal freedoms, along with changes in social contacts and activities, may have brought additional challenges for the usual activities, routines, and livelihoods of older adults (United Nations, 2020b; WHO, 2020c). Following pre-pandemic evidence showing that social isolation increases the risk for mental health problems, particularly for older adults (Santini & Koyanagi, 2021), developing or worsening loneliness among this high-risk population has emerged as a COVID-19 research priority during the early stage of the pandemic across continents. In China, Shi et al. (2020) found that centralized or home quarantine during the early stage of pandemic may have heightened the presence of symptoms of depression, anxiety, and insomnia among older adults. Additionally, Wong et al. (2020) suggest that strict lockdown measures may have resulted in worsening mental health, including loneliness, anxiety, and insomnia, in Chinese older adults after the onset of the COVID-19 outbreak. Consistently, Gan et al. (2021) has shown that quarantine measures are a risk factor contributing toward higher levels of loneliness, sadness, and depression among Vietnamese people aged 50 and over.
In Europe, Stolz et al. (2021) found a worsening of mental health outcomes among Austrian older adults during the early stage of the pandemic, showing increased levels of loneliness among 9% of respondents. Dziedzic et al. (2021) found higher levels of depressive symptoms and a high sense of loneliness among Polish people aged 50 and over experiencing social distancing and isolation after the COVID-19 outbreak. In the Czech Republic, Novotný et al. (2020) revealed that the prevalence of high stress and symptoms of depression increased during the COVID-19 lockdown among older adult respondents.
Prior results on mental health changes during the pandemic correspond with the recent North-American experience, as Fuller and Huseth-Zosel (2021) showed increasing rates of loneliness among U.S. older adults due to social isolation and feelings of loss during COVID-19 lockdown measures. Consistently, 43.1% of Canadian older adults reported that 2020 physical distancing and stay-at-home measures intensified their feelings of loneliness (Savage et al., 2021).
Overall, the relationship between preventive strategies, loneliness, and mental health changes during the early stage of the COVID-19 outbreak has been reported globally by recent research. However, some COVID-19 research gaps still remain to be addressed. Recent mental health studies on COVID-19 were mostly one-time cross-sectional, focusing on mental health consequences in the vulnerable older adult population after the 2020 pandemic outbreak. Uncertainty remains about the trajectory of loneliness and mental health changes throughout the lockdowns and social safety measures (e.g., Bartrés-Faz et al., 2021; Macdonald & Hülür, 2021). Additionally, international comparative studies could shed light on the question of whether the prevalence of loneliness and mental health changes during the pandemic differs between countries and explore which micro-level factors may contribute toward those possible differences (e.g., Atzendorf & Gruber, 2022). However, evidence of loneliness across advanced age groups from a longer time perspective remains sparse.
The Czech Republic is one of the countries that prolonged the duration of COVID-19 social distancing measures during the early (2020) and late (2021) stages of the pandemic (see Ministry of Health of the Czech Republic, 2023; WHO, 2021), and reported higher rates of stress, anxiety, or loneliness during the 2020 COVID-19 restrictions (Vaculíková & Hanková, 2021; Winkler et al., 2020). Therefore, it seems relevant to take into consideration these specifics on the pandemic (early and late stages of COVID-19 outbreak) and age (older adults aged over 50) and examine the potential impact of social distancing restrictions on mental health outcomes in a high risk population.
To address this gap, the current study analyzes data from two waves of the Survey of Health, Ageing and Retirement in Europe (SHARE) Corona survey, targeted to the COVID-19 living situation. We aim to explore trends in the presence of loneliness in the high-risk population aged 50 and over between the early (2020) and late (2021) stages of the COVID-19 outbreak. In addition, given the fast-growing evidence showing that loneliness may be a risk factor for higher rates of depression, anxiety, or nervousness (Killgore et al., 2020; Losada-Baltar et al., 2021; Park et al., 2021), we sought to identify the main determinants of loneliness in the Czech Republic, a nation which is one of the European countries with the highest proportion of lonely people (Yang & Victor, 2011).
Method
Study Design and Participants
Participants were drawn from SHARE, a cross-national representative panel study focused on the health and living situation of the population since 2004, covering all continental EU countries, plus Switzerland and Israel (Börsch-Supan, 2020). The target population of SHARE consists of all persons 50 years and over who have their regular domicile in the respective SHARE country. Additionally, respondents are followed when entering a nursing or residential home (Bergmann & Börsch-Supan, 2021). Individuals are excluded from the sample if they are incarcerated, hospitalized, out of the country during the entire survey period, unable to speak the country’s language, or have moved to an unknown address (SHARE, 2022). Spouses or partners of people 50 years and over are included in the target population, regardless of their own age. Therefore, the target population of SHARE could also be defined in terms of households, that is, all households with at least one member belonging to the target population of individuals (Bergmann & Börsch-Supan, 2021).
Age-eligible respondents who were interviewed in any previous wave are part of the longitudinal database and can be re-interviewed in any following wave. In the ideal case, all countries would have a probability-based sample from an official persons register used as sampling frames (Bergmann & Börsch-Supan, 2021). Therefore, sampling frames can be different between waves or countries. However, a key feature any sampling frame has to fulfil is the availability of reliable information on age. For details on SHARE’s target population and eligibility criteria, see Kneip (2013), Bergmann et al. (2017), and Bergmann and Börsch-Supan (2021), or visit the official SHARE webpage (https://share-eric.eu/).
Fieldwork for the SHARE Wave 8.0 data collection started in October 2019 and was impacted by the early stage of the COVID-19 outbreak in March 2020 (Börsch-Supan, 2022a). At this point in time, about 70% of all expected longitudinal and 50% of all expected refresher interviews across countries had been completed (Scherpenzeel et al., 2020). As a reaction, a specific “SHARE Corona survey” was targeted to living situations during the pandemic to better understand the unintended consequences of epidemic control decisions to contain the pandemic. Therefore, SHARE provided an ideal infrastructure to put the consequences of the current situation in its proper context and determine the impact of the pandemic on respondents’ living conditions, which had been routinely recorded from previous waves. Using the SHARE Corona survey, ongoing interviews among all its panel respondents were instituted using computer assisted telephone interviews (CATI) from June 8 to August 6, 2020. This covered 2,631 participants with the average age of 72.9 years (SD = 7.7), mostly women (62%).
Meanwhile, the Czech government implemented a public COVID-19 lockdown between March 16 and May 17, 2020 (see Supplemental Appendix Figure A1). It included a national COVID-19 crisis quarantine with closures of borders, schools, and services excepting daily necessities, take-away, and deliveries, as well as compulsory usage of individual protection equipment and the implementation of safety measures prohibiting large gatherings. Data-gathering interviews during the late stage of the COVID-19 outbreak, SHARE Wave 9.0, were conducted between June 3 and August 4, 2021 (Börsch-Supan, 2022b). The data included 2,083 participants with the average age of 73.8 years (SD = 7.4), mostly women (63%).
The data collection and data analysis in this study have followed ethical principles of research, respecting the ICC/ESOMAR International Code (ESOMAR, 2016). The principle of anonymity was applied to maintain the anonymity of the participants, and SHARE emphasized informed verbal consent throughout the study. Participants were informed about the aims of the research and that the given information would be treated confidentially.
Measurements
Loneliness was measured with the question “How much of the time do you feel lonely?” Responses were classified as 1 (“often”), 2 (“some of the time”), and 3 (“hardly ever or never”). This score was further recoded to a binary variable with the values “Lonely” (formerly Level 1–2) and “Not lonely” (Formerly Level 3). We created a Physical social isolation variable by adding points if the respondent had less than weekly face-to-face contact with (a) their own children, (b) their own parents, (c) other relatives, or (d) other non-relatives like neighbors, friends, or colleagues; points were added if the respondent was not personally involved in social activities such as (e) volunteering or did not provide (f) personal care outside the respondent’s household. Scores ranged from 0 to 6, with higher scores indicating higher physical social isolation. Digital social isolation was measured as the sum of the points obtained if the respondent had less than weekly digital contact by phone, email, or any other electronic means with (a) their own children, (b) their parents, (c) their relatives, or (d) other non-relatives like neighbors, friends, or colleagues. Scores ranged from 0 to 4.
Mental health variables were measured with questions with single “yes/no” answer about whether participants felt nervous, anxious, or on edge (labelled as Nervous) or if they experienced trouble sleeping or any recent changes in sleeping patterns (labelled as Trouble sleeping). The same coding was used for the question “Have you been sad or depressed, meaning miserable, in low spirits, or blue, in the previous month?,” labelled as Sad/Depressed.
Physical health was self-rated on a five-point Likert scale from 1 (“excellent”), 2 (“very good”), 3 (“good”), 4 (“fair”), to 5 (“poor”). Scores were further recoded into a three-category variable with the levels “Very good” (formerly Levels 1–2), “Good” (formerly Level 3), and “Poor” (formerly Level 4–5). The coding 0 (“Good” or “Poor”) and 1 (“Very good”) was used for binary analysis. Respondents were also asked if they had ever left their home since the COVID-19 outbreak (where 0 = “no,” 1 = “yes”). Demographic variables included gender (0 = “men,” 1 = “women”), age category, and age in years, including Working (50–70 years), Young retirees (71–79 years), and oldest old (80+ years).
Analysis
To compare the primary results of the SHARE Wave 8.0 (fielded in 2020) and SHARE Wave 9.0 (fielded in 2021) data sets, descriptive statistics were applied. Changes in loneliness, in relation with physical and digital social isolation in response to the early and late stages of the COVID-19 outbreak, were assessed by t tests. To analyze the impact of individual sociodemographic, physical, and mental health characteristics on the probability of the presence of loneliness, separate binary logistic regressions were carried out. The aim of model selection was to define the main micro-level demographic, health-related, and social variables that would explain the maximum range of the dependent variable. Therefore, the impact of theory-based variables on the likelihood of the presence of loneliness was partly exploratory in nature, but at the same time built up the models that balance goodness of fit with simplicity.
Subsequently, a decision tree analysis was included, featuring a CHAID growing method, which orders independent variables according to their influence on the dependent variable. More specifically, the decision-tree analysis clusters results in a progressively branching chart. CHAID combines the categories of individual variables unless they are significantly different. Therefore, the demand is placed on internally homogeneous categories that are, on the contrary, heterogeneous between each other. Validation included a cross-validation method (10 sample folds), with the growth limit of the minimal number of cases set to 100 for Parent node and 50 for Child node. Based on careful consideration of the key factors included (Deaton, 2019; Leamer, 1978), such as sample size and expected losses from Type I and II errors, the level of significance was set at 0.001. Statistical computations were performed using IBM SPSS version 27.
Results
The descriptive results (see Supplemental Appendix Table A1) show that 27% of participants felt lonely in 2020. In 2021, the presence of loneliness rose negligibly to 28%. Looking more closely, we can see several trends in the presence of loneliness between the early and late stages of the COVID-19 outbreak. A substantial increase in reported loneliness was found in those participants who reported their physical health as poor (32% in 2020 and 46% in 2021), who felt nervous (by 8%), sad or depressed (by 4%), and who had left their home since the COVID-19 outbreak (by 8%). While in 2020, the reported loneliness of mostly working adults (50–70 years) was high at 36%, the data from 2021 show a slowly decreasing trend at 27%. On the contrary, retirees (71–79 years) and the elderly (80+ years) felt more lonely in 2021 compared to the previous year. However, in both data collections, reported loneliness was the highest in 71 to 79 year old adults. As for gender and trouble sleeping, the percentage of reported loneliness remained almost unchanged. Moreover, the results show that participants experienced more physical social isolation in 2020 (M = 3.86, SD = 1.07) than in 2021 (M = 2.82, SD = 1.12). Digital social isolation increased slightly in 2021 (M = 1.32, SD = 1.04) compared to 2020 (M = 1.20, SD = .99).
The Influence of Individual Characteristics on the Presence of Loneliness
We focused on the simplicity of the models and uploaded micro-level independent variables that would explain the maximum range of the presence of loneliness. Adding other variables to the models did not lead to a significant improvement of the correct classification of the cases. Preliminary analyses were conducted to ensure that there was no influence of outliers or violations of the assumptions of multicollinearity. This can be excluded as all values of tolerance (1/VIF) are above 0.2 (see the last column of the Tables 1 and 2).
Model 1: Logistic Regression of the Presence of Loneliness in 2020 (n = 2,631).

Note. SE = standard error; Df = degrees of freedom; CI = confidence interval; VIF = variance inflation factor.
Model 2: Logistic Regression of the Presence of Loneliness in 2021 (n = 2,083).
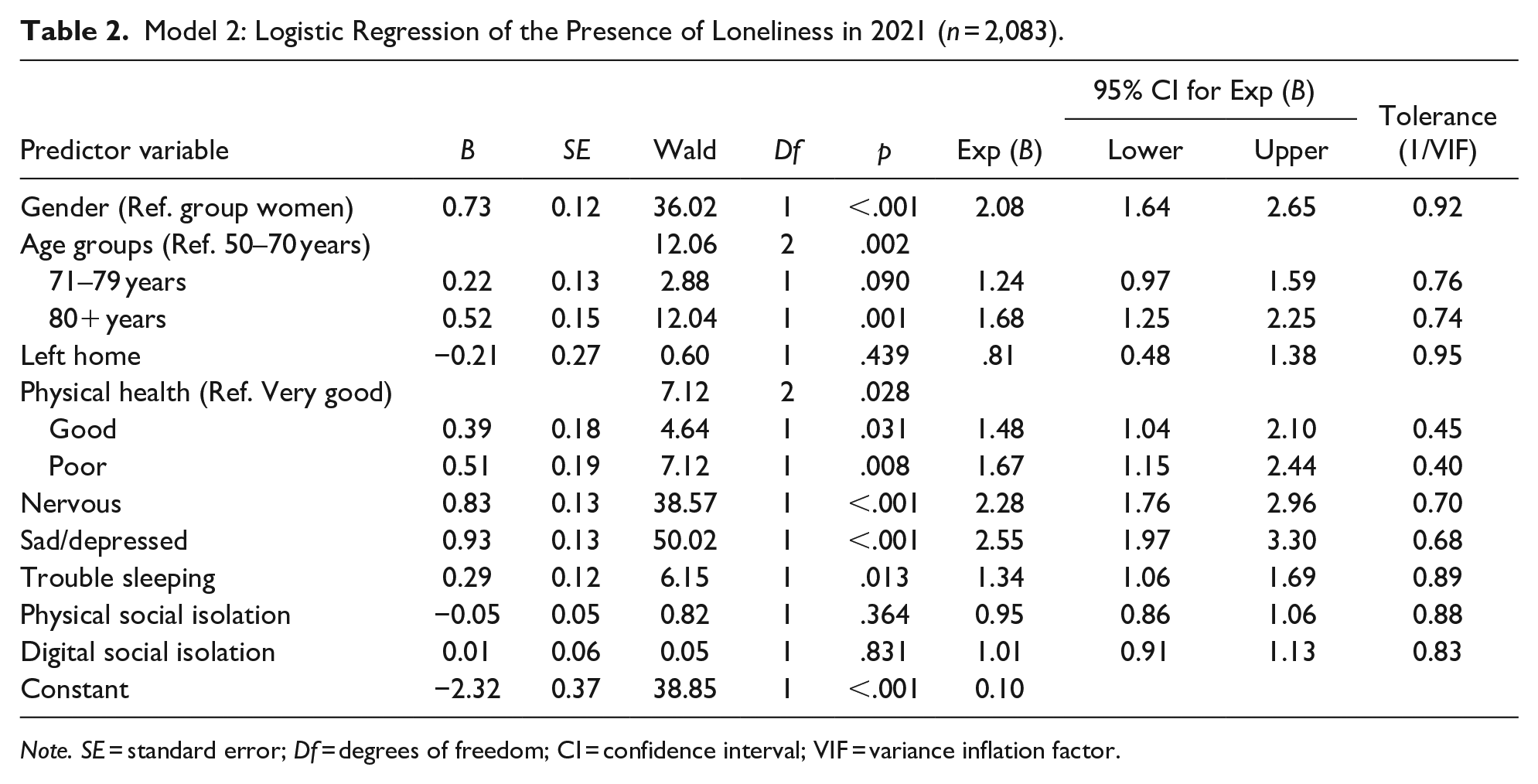
Note. SE = standard error; Df = degrees of freedom; CI = confidence interval; VIF = variance inflation factor.
Model 1 reached statistical significance x2(11, N = 2,63) = 411.51, p < 0.001; Cox and Snell R2 = 0.15 and Nagelkerke R2 = 0.21, explaining between 15% and 21% of the variability with the set of variables. The model correctly classified 76% of cases with an improvement from 72% to 76%. Out of the tested variables in the equation, the experience of sadness or depression, gender, self-rated physical health condition, nervousness, and trouble sleeping made a unique statistically significant contribution to the model (p ≤ 0.001). As can be seen in Table 1, participant age, leaving home since the COVID-19 outbreak, and physical and digital social isolation did not reach significance.
The crucial predictor of loneliness in the early stages of the COVID-19 outbreak within Model 1 was the experience of sadness or depression, recording the highest odds ratio for reported loneliness in sad or depressed individuals (OR = 3.69; 95% CI [2.90, 4.69]). This result shows that participants who felt sad or depressed were almost four times more likely to report the presence of loneliness than a person who did not feel sad or depressed, while controlling for all other predictors in the model. Another essential variable that rapidly increased the chances of reported loneliness was gender (OR = 1.98; [1.60, 2.45]), indicating that women were predicted to report the presence of loneliness more often relative to men. Further, those participants who felt good (OR = 1.81; [1.39, 2.36]) or poor (OR = 1.87; [1.38, 2.53]) before the outbreak were more likely to report loneliness compared those who felt that their general health condition was very good. Lastly, feelings of nervousness (OR = 1.63; [1.28, 2.07]) and trouble sleeping (OR = 1.43; [1.17, 1.76]) significantly increased the likelihood of reported loneliness in the early stages of the COVID-19 outbreak.
Model 2 reached statistical significance x2(11, N = 2,08) = 342.49, p < 0.001; Cox and Snell R2 = 0.15 and Nagelkerke R2 = 0.22, explaining between 15% and 22% of the variability. The improvement of the correctly classified cases within the model was from 71% to 76%. Out of the nine independent variables in the equation, four made a unique statistically significant contribution to the model (p < 0.001). Based on the regression analysis, sadness or depression was again the strongest significant predictor of loneliness (see Table 2). However, we found lower odds of loneliness (OR = 2.55; 95% CI [1.97, 3.30]) compared to 2020. In comparison with the previous year, feeling nervous (OR = 2.23; [1.76, 2.96]) and being a woman (OR = 2.08; [1.64, 2.65]) were associated with higher odds of loneliness. Further, we found no significant results indicating that being unhealthy predicts loneliness. Similarly, trouble sleeping lost its significance in 2021. On the other hand, oldest old (80+ years) participants were almost two times more likely to report the presence of loneliness than mostly working adults (50–70 years). In the case of physical and digital social isolation, similarly to 2020, we found no significant results indicating that being socially isolated predicts loneliness.
Application of a Decision Tree Algorithm
Further application of the decision-tree algorithm focused on previously identified key variables significant in both models, that is, being sad or depressed, nervous, and gender, and how their combinations change the percentage of reported loneliness. This analysis allows us to see our results from a different view, and we consider it their validation.
As shown in Supplemental Appendix Figure A2, the algorithm correctly classified 76% of cases. The graph is gradually split from top to bottom according to predictors of loneliness. The self-rated presence of sadness or depression had the most significant effect on loneliness, followed by nervousness and gender. Most participants (66%) were women and felt nervous, sad, or depressed in the previous month. On the other hand, the lowest level of reported loneliness (13%) was found among men who did not feel sad or depressed.
Supplemental Appendix Figure A3 shows the results for the late stages of the COVID-19 outbreak. The analysis correctly classifies 76% of cases and the results were similar to 2020. The results from the 2021 model showed that if respondents were women who felt nervous, sad or, depressed, we predicted that they would be lonely 68% of the time. This rule applied to 259 respondents and was accurate about 176 times. On the other hand, if respondents were men who did not feel nervous, sad, or depressed, we were able to accurately predict that they would be lonely around 11% of the time. This prediction applied to 571 men and the model was accurate 64 times.
Discussion
Prior results show that older adults are at high risk for demonstrating consequences of the pandemic (Krendl & Perry, 2021; Remuzzi & Remuzzi, 2020), especially increasing feelings of loneliness (Berg-Weger & Morley, 2020). Based on our findings from a nationally representative sample of adults aged 50 and over, including cross-sectional early and late data collection, almost every third older adult (27% in 2020 vs. 28% in 2021) experienced feelings of loneliness. This result represents a greater percentage of loneliness compared to previous years before the pandemic (Lee, 2020) and significantly exceeds the European average, ranging from around 7–9% to 14.5% in Great Britain (Thomas 2015; Victor and Bowling, 2012), and from 10% to 25% overseas (Kuwert et al., 2014).
Contrary to our expectations, we found no change in reported loneliness in the early and late stages of the pandemic. Consistently, Peng and Roth (2022) reported no change in reported loneliness during the pandemic among a nationally representative panel study of U.S. adults aged 50 years and older. Similarly, Luchetti et al. (2020) found no significant mean-level changes in loneliness using a nationwide sample of American adults. In contrast, Bu et al. (2020) showed that the prevalence of reported loneliness among the British adult population increased from 37% during the pre-pandemic period to 51% during the COVID-19 pandemic. However, compared to previous studies, we examined the trajectory of reported loneliness on nationally representative data in response to the early (fielded in 2020) and late stages (fielded in 2021) of the COVID-19 pandemic outbreak. Therefore, the presented results constitute original evidence of reported loneliness affected by the presence of the pandemic within a highly affected central European country.
Moreover, several trends can be tracked between the early and late stages of the COVID-19 outbreak. Loneliness increased in 2021 in those participants who reported their physical health as poor, who felt nervous, sad, or depressed, and who had never left their home since the COVID-19 outbreak. According to age-related drivers of loneliness, loneliness was the highest in 71–79 year old adults in both waves. Similarly, individuals aged 75–84 years were more likely to feel lonely most of the time compared with their younger (65–74) and older (85+) counterparts (Vozikaki et al., 2018). All adults felt lonelier in 2021 compared to the previous year, except mostly the working age-group (50–70). However, research focusing on loneliness and how it might vary with age has revealed developmental and partly socio-cultural mechanisms of loneliness (de Jong Gierveld, 2006; Qualter et al., 2015). As Jopling and Sserwanja (2016) stated, different age groups are likely to experience specific challenges with social connections or individualism turning to salient implications for loneliness related to old age.
Interestingly, participants felt more physical social isolation during the early stage of the COVID-19 pandemic compared to later years. Digital social isolation increased slightly in 2021 compared to the previous year. As reported in the literature (i.e., Barreto et al., 2021; Dahlberg et al., 2015; Singh & Misra, 2009), sadness or depression was the strongest significant predictor of loneliness in regression models from 2020 and 2021. In both models, women had higher odds of considering themselves lonely and individuals feeling nervous were more likely to feel lonely compared to their counterparts. Similarly to the reported results of von Känel et al. (2021) or Wickens et al. (2021), our findings show that out of socio-demographic characteristics, being a women and sensitive to adverse health conditions can serve as a risk factor predicting loneliness. In concordance with previous evidence of an association between health-related physical and mental outcomes and loneliness (Savikko et al., 2005, Victor et al., 2005), the current study found that poor health and trouble sleeping was significantly associated with loneliness but lost its significance in the 2021 regression model. Moreover, as confirmed by the decision-tree algorithm, women who felt nervous and experienced sadness or depression constitute a vulnerable population of older adults who are at high risk of feeling lonely.
There are several limitations on the current study. First, although we are building our research on a nationally representative sample, we are missing a comparison with young adults. However, based on a review of reported loneliness within a comprehensive theoretical framework (Hawkley & Cacioppo, 2010), loneliness is about three times more prevalent in older adults compared to young adults, and is therefore recognized as a vulnerable population. Second, loneliness is often measured on internally consistent scales instead of as the results of single-item measure as used in this study. However, this self-reported measure has been commonly used for its simplicity, easy understanding, and convergence with other multi-item scales (Pinquart & Sorensen, 2001; Vozikaki et al., 2018). Third, our results might not correspond with those of previous studies conducted worldwide since each country experienced specific lockdown measures with different kinds of restrictions reflecting the expansion of the pandemic. Similarly, the presented results can vary according to participants’ household composition, which was not measured in this study. However, people can live in a relatively solitary way without feeling lonely, and conversely, they can have a rich social life and nevertheless feel lonely. Therefore, further research should take these issues into account, as well as social and behavioral effects on loneliness.
As for future research, a comprehensive assessment of reported loneliness, utilizing sophisticated measures particularly relevant in the context of later life and experiences of the pandemic, might be beneficial. We encourage researchers to look for possible predictors of loneliness in a wider range of intervening life events and psychological predictors that may induce the presence of loneliness. As a related point, we need to bear in mind that older adults included in this study were most likely less affected by the pandemic than, for example, residents of nursing homes and other long-term care facilities. Moreover, attention should be placed on systematic and continuing research into negative effects of the recurring COVID-19 pandemic, as it is unclear how strong and long lasting the effects are on older adults’ loneliness. As age, gender, and culture interact to predict loneliness (Barreto et al., 2021), exploring loneliness in already lonely adults would be beneficial not only at the national but also the international level.
Despite these limitations, this study is, to our knowledge, the first attempt to explore the presence of loneliness by utilizing demographic, health-related, and social variables that are relevant for aging among older adults during the early and late peaks of the COVID-19 pandemic. Health and social policy initiatives should direct particular attention to the implications of safety measures; older adults’ social and health-related resources should be untouched during the pandemic and present opportunities to remain socially engaged.
Supplemental Material
sj-docx-1-ggm-10.1177_23337214231174129 – Supplemental material for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over
Supplemental material, sj-docx-1-ggm-10.1177_23337214231174129 for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over by Jitka Vaculíková and Magdalena Hanková in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-2-ggm-10.1177_23337214231174129 – Supplemental material for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over
Supplemental material, sj-docx-2-ggm-10.1177_23337214231174129 for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over by Jitka Vaculíková and Magdalena Hanková in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-3-ggm-10.1177_23337214231174129 – Supplemental material for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over
Supplemental material, sj-docx-3-ggm-10.1177_23337214231174129 for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over by Jitka Vaculíková and Magdalena Hanková in Gerontology and Geriatric Medicine
Supplemental Material
sj-docx-4-ggm-10.1177_23337214231174129 – Supplemental material for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over
Supplemental material, sj-docx-4-ggm-10.1177_23337214231174129 for Loneliness and Mental Health in Response to Early and Late COVID-19 Outbreak: A Cross-Sectional Study of Czech Adults Aged 50 and Over by Jitka Vaculíková and Magdalena Hanková in Gerontology and Geriatric Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04-064, HHSN271201300071C, RAG052527A), and from various national funding sources is gratefully acknowledged (see ![]() ).
).
IRB Protocol/Human Subjects Approval Numbers Acknowledgements
The CTL institution in cooperation with SHARE-ERIC took responsibility for the implementation of the SHARE survey. Participation in the SHARE interview was voluntary, and all information was kept confidential. The conversation was not recorded and all participants received a data-protection statement. Individual researchers were not provided with contact details of the respondents.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.