
Abstract
Objectives
This paper examines the longitudinal effects of changes in the association between loneliness and depressive symptoms during the pandemic among older adults (65+).
Keywords
Introduction
To reduce the spread of the highly contagious SARS-CoV-2 coronavirus (COVID-19), governments implemented physical distancing, closure of non-essential businesses and public spaces, implementation of lockdowns and stay at home orders, mask mandates, travel restrictions, and other public health restrictions. Although these measures resulted in some successes in reducing transmission of COVID-19, research demonstrating negative impacts of the prolonged periods of physical and social distancing on feelings of loneliness with specific attention on older adults has been accumulating (Heidinger & Richter, 2020; Morrow-Howell et al., 2020; Shahid et al., 2020). Indeed, Smith et al. (2020) use the term “Covid-19 Social Connectivity Paradox” to refer to the paradox that meaningful interactions and social participation are important for the health of older adults, yet pandemic restrictions require older adults to avoid friends, family, and sources of social support.
Loneliness refers to the subjective feeling of not having one’s social needs met, whereas social isolation pertains to the number and quality of social connections (Newall et al., 2015). According to the World Health Organization (2020), loneliness and social isolation are public health concerns that affect aging societies globally. An extensive body of literature prior to the pandemic has established associations between loneliness and social isolation and worsening mental health, lower health-related quality of life, and reduced access to health care services (Burholt et al., 2020; Cacioppo et al., 2010; Courtin & Knapp, 2017; Coyle & Dugan, 2012; Leigh-Hunt et al., 2017; National Seniors Council, 2016; Newall et al., 2015; Schwarzbach et al., 2014; Wister et al., 2019). Research has generally supported stronger associations between loneliness and mental health than for social isolation (Cornwell & Waite, 2009; Kadowaki & Wister, in press). For instance, Coyle and Dugan (2012) found that loneliness resulted in 17% higher odds of having a mental health issue. It is nevertheless estimated that 1 in 10 Canadians experienced a mental health problem in any given year, with depression being the most common (Canadian Coalition for Seniors’ Mental Health, 2021), accounting an economic burden in Canada of approximately US$32 billion (Smetanin et al., 2015).
Although a growing number of findings reinforce associations between loneliness or social isolation and mental health during the pandemic (Fingerman et al., 2020; Kim & Jung, 2021; Krendl & Perry, 2021), some studies show no change in the mental health of older adults during the pandemic or better mental health outcomes among older persons than those in younger age groups (De Bruin, 2021; Van Tilburg et al., 2020).
Social Isolation, Loneliness and Depression Pre- and Peri-pandemic
Social isolation and loneliness have been associated with worsening mental health among general populations in several pre-pandemic systematic reviews (e.g., Leigh-Hunt et al., 2017; Santini et al., 2015). Turning specifically to older adults, loneliness (and to a lesser degree social isolation), has been shown to worsen depressive symptoms in a number of studies (e.g., Coyle & Dugan, 2012; Noguchi et al., 2021; Taylor et al., 2018). For example, in a cross-comparison of longitudinal data drawn from two waves of the English Longitudinal Study of Ageing (ELSA) and the Japan Gerontological Evaluation Study (JAGES), associations were supported between greater social isolation (using marital status; interaction with children, relatives and friends, and social participation) and depression in both data sets (Noguchi et al., 2021). In addition, in a large US study, subjective social isolation (i.e., loneliness) from both family and friends was associated with further depressive symptoms but not objective social isolation (Taylor et al., 2018). Finally, loneliness was associated with higher odds of having a mental health problem among older adults (Coyle & Dugan, 2012).
Turning to the peri-pandemic period, a number of studies have reported that perceived loneliness during the pandemic is associated with depression (e.g., Kotwal et al., 2021; Krendl & Perry, 2021; Mistry et al., 2021; Robb et al., 2020). These studies were either cross-sectional or small sample size longitudinal designs, or provided only descriptive results. For instance, Kotwal et al. (2021) found that of the 151 participants in their study, the majority (54%) of the participants in their longitudinal study reported worsened loneliness due to COVID-19, which was associated with worsened pre-post depressive symptoms based on an ordinal self-reported question (62% vs. 9%; p < .001). In another longitudinal study, Krendl and Perry (2021) also found an association between greater loneliness and depression, but in a small (n = 120) local survey. Similarly, large cross-sectional results supporting an association between greater loneliness and depression have been reported in the UK (n = 7127, aged 50+) (Robb et al., 2020) and Bangladesh (n = 1032) during the pandemic (Mistry et al., 2021). Qualitative studies also support these findings. For instance, in a descriptive study by Whitehead and Torossian (2021), older adults reported loneliness or isolation as the third most frequently identified stressor during the pandemic. Additionally, older women, and older adults having low-income or single/widowed ranked loneliness or isolation highest as a stressor.
The evidence for an association between loneliness and depression during the pandemic remains equivocal and requires further research for several reasons. First, longitudinal studies tend to be small in size which limit generalization. Second, many studies used cross-sectional designs, which does not allow researchers to verify predictors of depressive symptoms. Third, different measures of social isolation and loneliness were used, ranging from validated scales to single-item proxies, making comparisons across studies difficult. Fourth, many studies did not incorporate covariates beyond basic demographic information. And fifth, these studies were carried out with diverse populations and variation in time, disease spread, and pandemic restrictions. Therefore, the aim of this paper is to address this gap in the literature by examining associations between changes in loneliness and depressive symptoms during COVID-19, including other covariates of depressive symptoms. Identifying whether such association exists is beneficial to health care providers, and health and community programs aimed at addressing depressive symptoms among older adults who are at risk of loneliness today and in the future.
Conceptual Model
The Transactional Stress Model (TSM) provides a conceptual foundation for understanding the links between stress, social support (providing assistance or comfort, including their absence due to loneliness and social isolation) and coping (Lazarus & Folkman, 1984, 1987; Obbarius et al., 2021; Pearlin et al., 2005). The TSM contends that the stress-coping process is affected by appraisals, responses and adaptations to adversity. One core component in this literature is the role of social support as a mediator (Pearlin et al., 2005). The TSM thus provides a rationale as to why we would hypothesize that pandemic-related stressors, such as heightened levels of loneliness and social isolation due to infection mitigation, would increase depressive symptoms among older adults (Minahan et al., 2021; Whitehead, 2021). Potential mechanisms underlying this process are negative appraisals of COVID-19 such as fear of infection, perceived seriousness, and overall pessimism; maladaptive behavioral responses such as restricting travel with others to obtain important necessities; and weakened coping skills. Further, models of resilience have also been incorporated into the stress-coping model to understand how individuals who have greater resources (e.g., structural and functional social support) are able to better offset the negative effects of pandemic adversity (Riehm et al., 2021; Wister & Speechley, 2020). The incorporation of a resilience strength-based lens can thus be added to the TSM and applied to the COVID-19 pandemic to understand mental health outcomes, including the identification of several important covariates that capture resources and deficits, consistent with key social determinants of health such as age, gender, socio-economic status, ethnicity, and functional status.
Methods
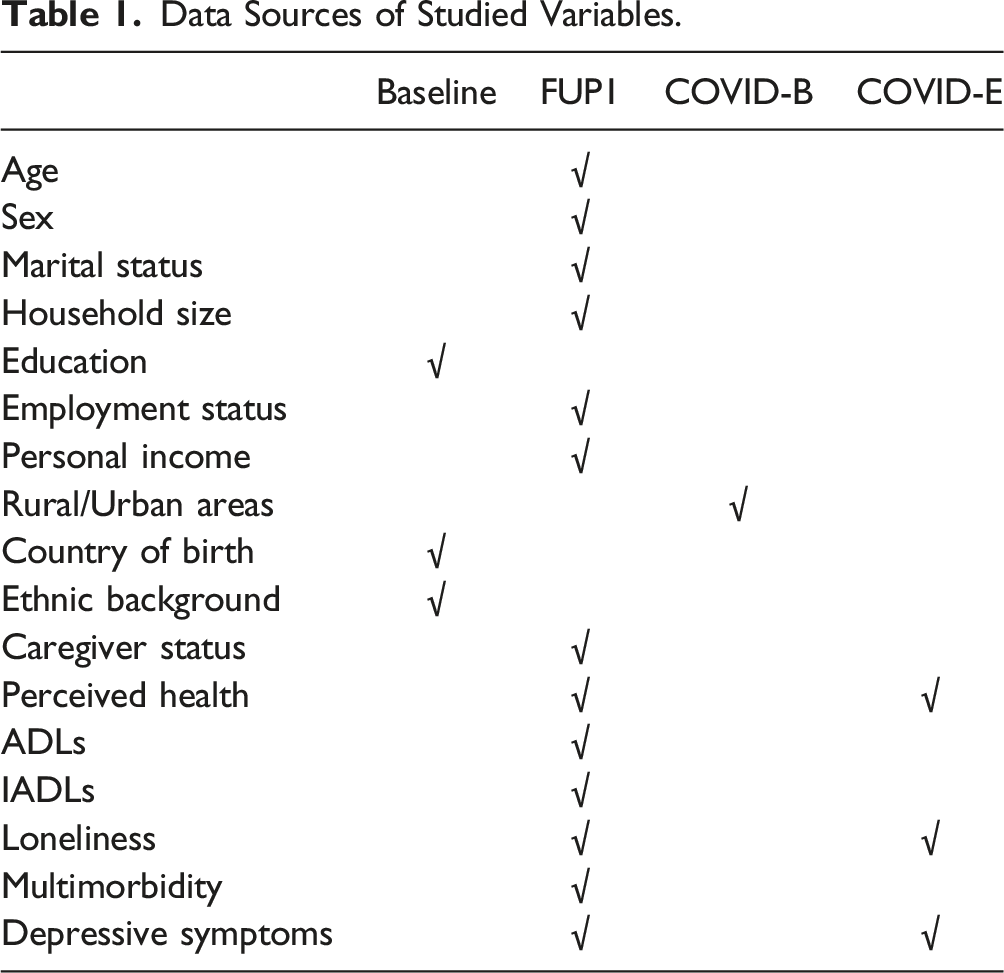
Data Sources of Studied Variables.
The CLSA participants are comprised of two cohorts, including the Comprehensive cohort and the Tracking cohort. The Comprehensive cohort participants were randomly selected from the population within 25–50 km (based on population density) from the 11 CLSA data collection sites across Canada, and the data were collected with a home-based interview and a follow-up visitation to the data collection sites for physiological and cognitive assessment. The Tracking cohort participants were randomly selected from the 10 provinces of Canada and interviewed through the telephone-interview system. This study analyzed the participants from both cohorts.
We focus on the group of older adults (65+) who finished both FUP1 and COVID-19 studies Exit survey. At FUP1, there are 23,466 participants aged 65 years and older. Among them, 12,469 (53.1%) participate in the COVID-19 studies Exit survey. The present study sample thus includes 12,469 older adults.
Measurement
Dependent Variable
The dependent variable, depressive symptoms, was measured by the Center for Epidemiologic Studies Short Depression Scale (CESD-10) (Andresen et al., 1994). The CESD-10 contains ten items assessing people’s depressive symptoms in the past week, with three items on depressed affect (e.g., I felt depressed), five items on somatic symptoms (e.g., My sleep was restless), and two items related to positive affect (e.g., I was happy). A Likert-scale was used to assess each item range from “rarely or none of the time” (score of 0) to “all of the time” (score of 3). In this study, the item “I felt lonely” was dropped, since we included the UCLA 3-item loneliness scale as an independent variable, which uses an identical scale item. Therefore, this study calculated the depressive symptoms with the remaining nine items, with a possible score ranging from 0 to 27 (Cronbach’s Alpha = .726 at FUP1, Cronbach’s Alpha = .815 at Exit survey). This measurement approach has been used in other research that examines associations between loneliness and depression (Cacioppo et al., 2010). A higher score means more depressive symptoms. As shown in Table 1, the data on depressive symptoms were collected at both FUP1 and COVID-19 studies Exit survey.
Independent Variable
The primary independent variable in this study is loneliness, measured using the 3-item UCLA loneliness scale (Russell, 1996). This scale is one of the most commonly used scales in assessing loneliness with very good reliability and validity (Hughes et al., 2004). Participants were asked to indicate the frequency they experience the following feelings based on a 3-point Likert scale (hardly ever, some of the time, and often), including (1) How often do you feel left out? (2) How often do you feel isolated from others? and (3) How often do you feel that you lack companionship? The summed-up scores range from 3 to 9 points, with a higher score indicating a greater level of loneliness (Cronbach’s Alpha = .739 at FUP1, Cronbach’s Alpha = .796 at Exit survey). The data on loneliness were collected at both FUP1 and COVID-19 studies Exit survey.
Covariates
Twelve demographic, health, and social determinants of health factors were included in the data analysis to control for potential confounding effects on the association between loneliness and depression based on a substantial body of literature (Kotwal et al., 2021; Krendl & Perry, 2021; Mistry et al., 2021; Raina et al., 2022; Robb et al., 2020; Wister et al., 2022a). We include: age, sex, marital status, household size, education, employment status, personal income, living areas, country of birth, ethnical background, several health measures, and caregiver status. Age was measured with actual number of years. Sex was measured by “female” and “male.” Marital status was dichotomized into “not married/partnered (single, widowed, divorced or separated)” and “married or in common-law relationship.” Household size was represented by the actual number of people living in the participant’s household. Education was grouped into two levels (due to small numbers in the original seven categories), including “without post-secondary education” and “with college diploma/university degrees.” Employment status was measured as “not working” or “working.” Personal income was originally measured at five levels and grouped into four levels: “less than US$20,000,” “US$20,000 to US$49,999,” “US$50,000 to US$99,999,” and “US$100,000 and more” (including US$100,000 to US$149,999 and US$150,000 and more). The living area was dichotomized as: “rural area” and “urban area.” Rural areas within the CLSA sampling frame are defined as communities with less than 10,000 population, and urban areas are defined from primary and secondary core areas down to the urban fringe and outlying areas with postal codes (St John et al., 2021). Country of birth was categorized into two groups, including “born in Canada” and “foreign born.” Ethnical background refers to participants’ cultural and racial backgrounds and was grouped into “Caucasian” and “visible minority.”
We also considered caregiver status (e.g., Wister et al., 2022a) and four health and function-related factors (e.g., Raina et al., 2022) drawn from prior research that has shown their effects on depression during the pandemic. Caregiver status was measured by “caregiver” and “non-caregiver” indicating whether participants provided assistance to another person due to a health condition or limitation in the past 12 months prior to the survey. Activities of Daily Living (ADL) and Instrumental Activities of Daily Living (IADL) were measured by the Older Americans’ Resources and Services Multidimensional Functional Assessment Questionnaire (Fillenbaum & Smyer, 1981). The ADLs and IADLs both contain seven items related to daily activities, such as dress and walk for ADLs, and use telephone and grocery shopping for IADLs. All the items were measured at three levels, from completely unable (0) to able (2). The ADLs and IADLs variables were summed based on each set of items, and higher scores indicate better functional capability. Self-perceived general health was measured with a 5-point Likert scale from “Poor” to “Excellent,” and further grouped into two levels, including “Poor to Fair” and “Good to Excellent.” Finally, multimorbidity status was measured at the FUP1 (2015–2018) pre-pandemic. At the FUP1, participants reported on the following 27 types of chronic conditions, including Alzheimer’s disease, back problems, bowel incontinence, cancer, cataracts, diabetes, epilepsy, glaucoma, heart attack, heart disease, high blood pressure, irritable bowel syndrome, kidney disease, Parkinson’s disease, peripheral vascular disease, lung diseases, macular degeneration, multiple sclerosis, osteoarthritis, osteoporosis, migraine headaches, rheumatoid arthritis, stroke, thyroid problem, transient ischemic attack, ulcer, and urinary incontinence. Based on the number of chronic diseases participants reported, participants were further grouped into two categories, including those with multimorbidity (with two or more chronic diseases), and those without (with one or fewer chronic disease).
Data Analytic Procedure
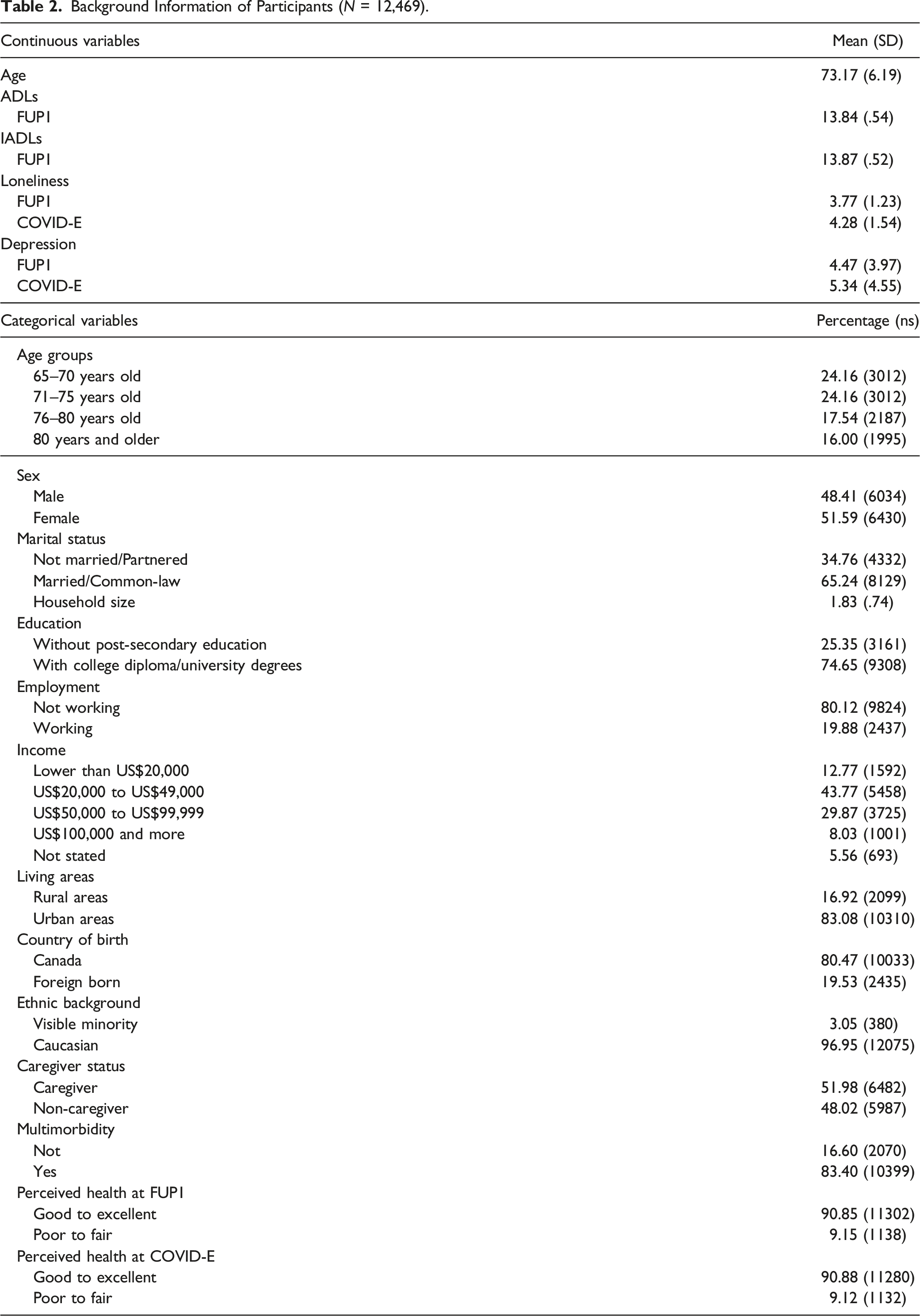
Background Information of Participants (N = 12,469).
Based on LMM, two models were created to examine the relationship between loneliness, multimorbidity status and the depressive symptoms among older adults. In model 1, loneliness and the survey factors (survey wave and participant cohorts) were included. In model 2, socio-demographic factors, caregiver status, health and function-related factors, and multimorbidity status variables were added. Interaction terms between all studied variables and survey wave were added in the analysis to examine the association between the independent variable/covariates and the change of depressive symptoms over the surveys. The socio-demographic, health and function related factors, loneliness, and multimorbidity status, as well as survey factors were included as fixed effects. A random intercept was included to model the variation in the dependent variable across participants. The estimates in the LMM can be interpreted the same way as those coefficients from a traditional ordinary least squares linear regression (Singer et al., 2017). Likelihood ratio tests based on the Akaike Information Criterion (AIC) was performed to compare the model fit. In addition, given the prominence of caregiving status, perceived health and multimorbidity on depression during the pandemic, we also test for interaction effects between each of these factors and loneliness on depression symptoms.
Results
Of 12,469 older adults that attended both FUP1 and the COVID-19 study Exit Survey, participants were an average of 73.2 years old (SD = 6.19) and living in a household with an average of 1.8 persons (SD = .74). Most participants were female (52%), married or living with a common-law partner (65%), educated with post-secondary diploma or degrees (75%), retired (80%), earning an annual income between US$20,000 and US$49,999 (44%), living in urban areas (83%), born in Canada (80%), Caucasian (97%), and caregivers (52%). About 83% of participants were categorized with multimorbidity (two or more chronic conditions). Most participants (9 in 10) rated their general health as Good to Excellent and reported high levels of ADLs and IADLs (13.8 and 13.9 out of 14, respectively). At the FUP1, the mean loneliness score was 3.77 (SD = 1.23), and it was 4.28 (SD = 1.54) at the COVID-19 Exit Survey. In addition, participants reported an average of 4.47 (SD = 3.97) for depressive symptoms based on the 9-item CES-D scale at the FUP1, and about 5.34 (SD = 4.55) at the COVID-19 Exit survey.
LMM for Depressive Symptoms (With Risk Groups in the Model).
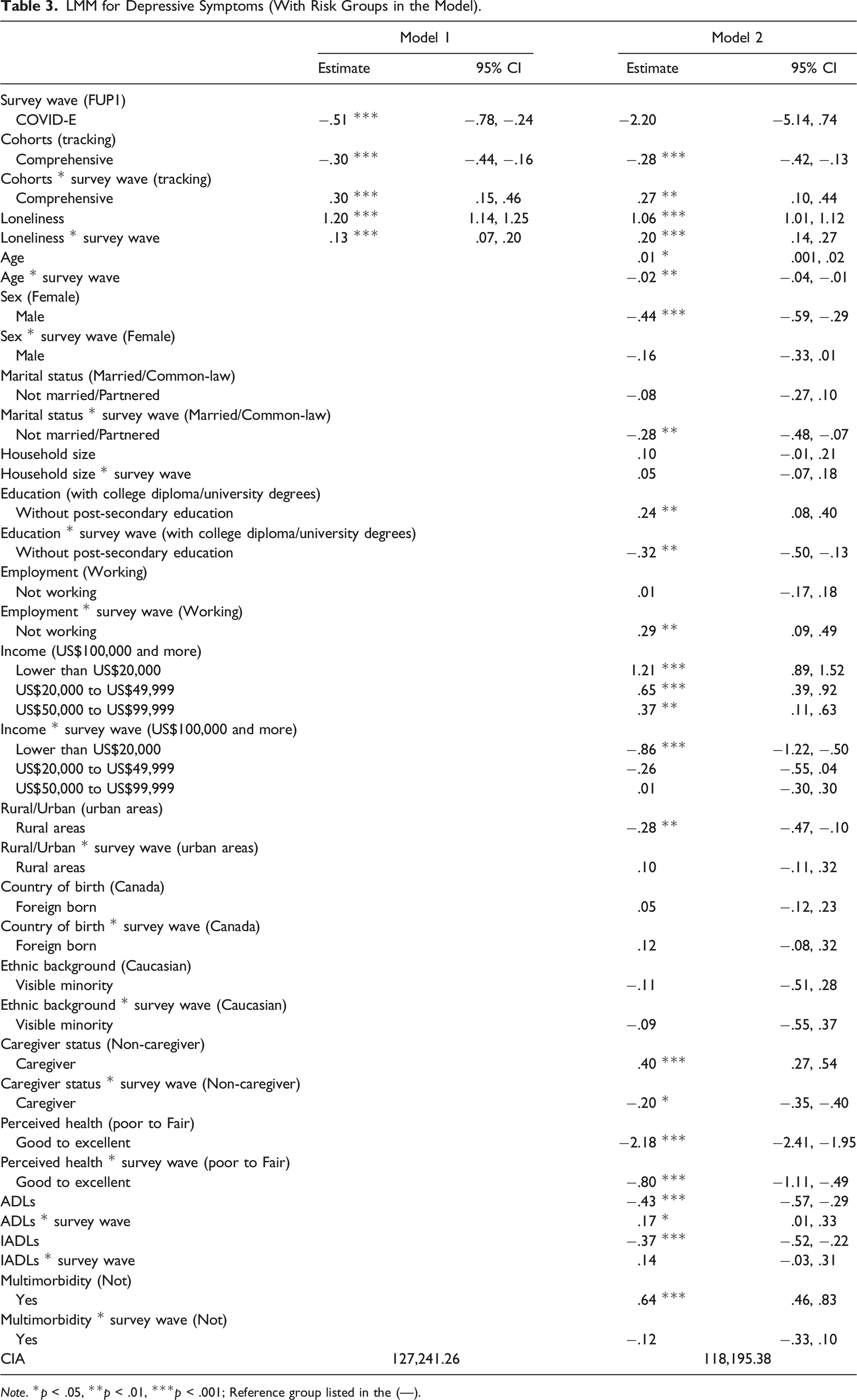
Note. *p < .05, **p < .01, ***p < .001; Reference group listed in the (—).
Considering the covariates, results yielded from model 2 with all studied variables incorporated are presented below. Being older was related to greater depressive symptoms at FUP1 (estimate = .01, 95% CI: [.001, .02]), and the association was reversed from FUP1 to the COVID-19 studies Exit survey (estimate = −.02, 95% CI: [−.04, −.01]). Older men reported fewer depressive symptoms at FUP1 than older women (estimate = −.44, 95% CI: [−.59, −.29]). Marital status was not related to depressive symptoms at FUP1, but participants who were not married/partnered reported smaller increasing of depressive symptoms from FUP1 to the COVID-19 Exit survey than those who were married or partnered (estimate = −.28, 95% CI: [−.48, −.07]).
For highest educational attainment, participants without post-secondary education reported higher levels of depressive symptoms than those with post-secondary education at FUP1 (estimate = .24, 95% CI: [.04, .40]). However, participants without post-secondary education reported a smaller increase in depressive symptoms from FUP1 to the COVID-19 Exit survey (estimate = −.32, 95% CI: [−.50, −.13]). Working status was longitudinally associated with depressive symptoms, and participants who were not working reported a greater increase in depressive symptoms than those who remained working from FUP1 to the COVID-19 Exit survey (estimate = .29, 95% CI: [.09, .49]). Compared to participants with an annual income of US$100,000 or more, all other participants with lower incomes reported greater depressive symptoms at FUP1, with an estimate of = 1.21, 95% CI: [.89, 1.52] for lower than US$20,000; estimate = .65, 95% CI: [.39, .92] for US$20,000 to US$49,999; and .37, 95% CI: [.11, .63] for US$50,000 to US$99,999. Between FUP1 and the COVID-19 Exit survey, the contrast of participants with an income lower than US$20,000 annually and US$100,000 or more was slightly attenuated (estimate = −.86, 95% CI: [−1.22, −.50]). The living location of participants was related to depressive symptoms at FUP1, and participants living in rural areas reported fewer depressive symptoms than those living in urban areas (estimate = −.28, 95% CI: [−.47, −.10]). Caregivers reported greater depressive symptoms than non-caregivers at FUP1 (estimate = .40, 95% CI: [.27, .54]), although this difference attenuated over time (estimate = −.20, 95% CI: −.35, −.40) (see Figure 1). Depression and loneliness from FUP1 to COVID-E based on caregiver status.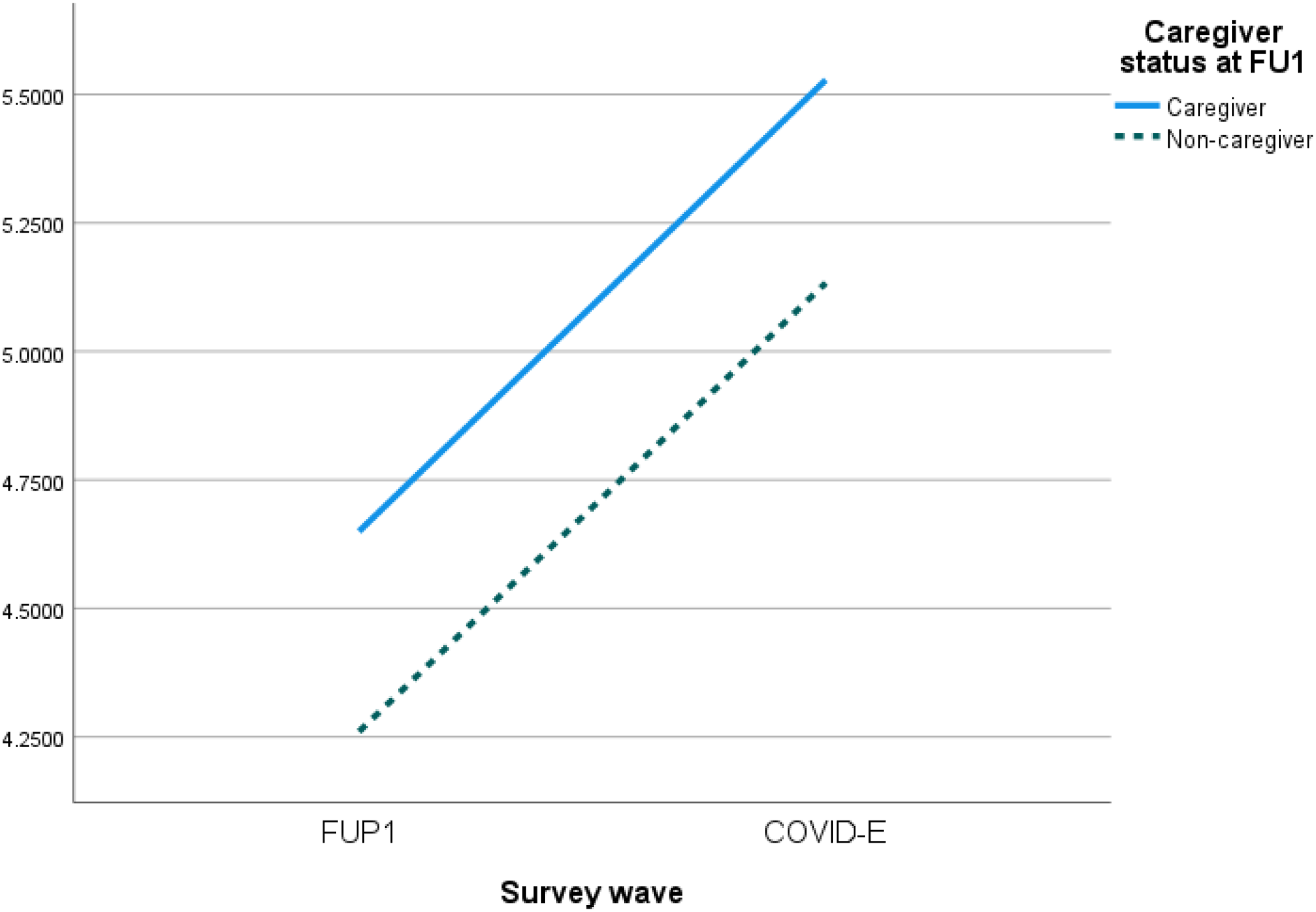
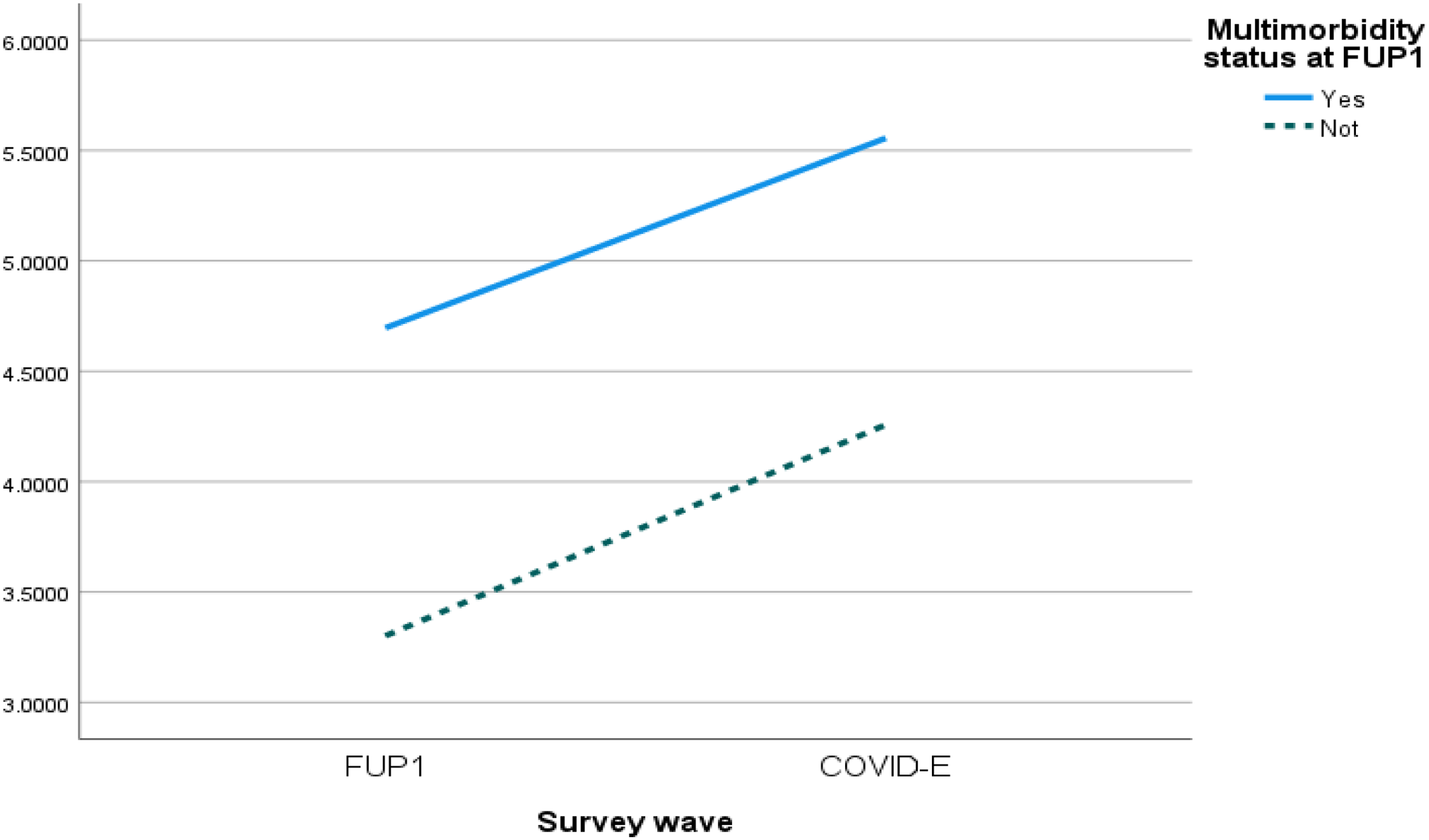
In addition, all four health factors were significantly related to depressive symptoms. Participants who rated their health as Good to Excellent reported fewer depressive symptoms than those with Poor to Fair health at FUP1 (estimate = −2.18, 95% CI: [−2.41, −1.95]), and the former group also reported a smaller increase in depressive symptoms than the latter group from FUP1 to the COVID-19 Exit survey (estimate = −.80, 95% CI: [−1.11, −.49]) (see Figure 2). The ADLs scale measuring functional status was negatively related to depressive symptoms at FUP1 (estimate = −.43, 95% CI: [−.57, −.29]), and the association was slightly attenuated over time (estimate = .17, 95% CI: [.01, .33]). The IADLs scale was also negatively associated with depressive symptoms at FUP1 (estimate = −.37, 95% CI: [−.52, −.22]), and no longitudinal effect was supported. When compared to participants without multimorbidity, older adults with two or more chronic diseases reported higher depressive symptoms at FUP1 (estimate = .64, 95% CI: [.46, .83]), but the interactive effect was not supported longitudinally (see Figure 3). Depression and loneliness from FUP1 to COVID-E based on perceived health. Depression and loneliness from FUP1 to COVID-E based on multimorbidity status.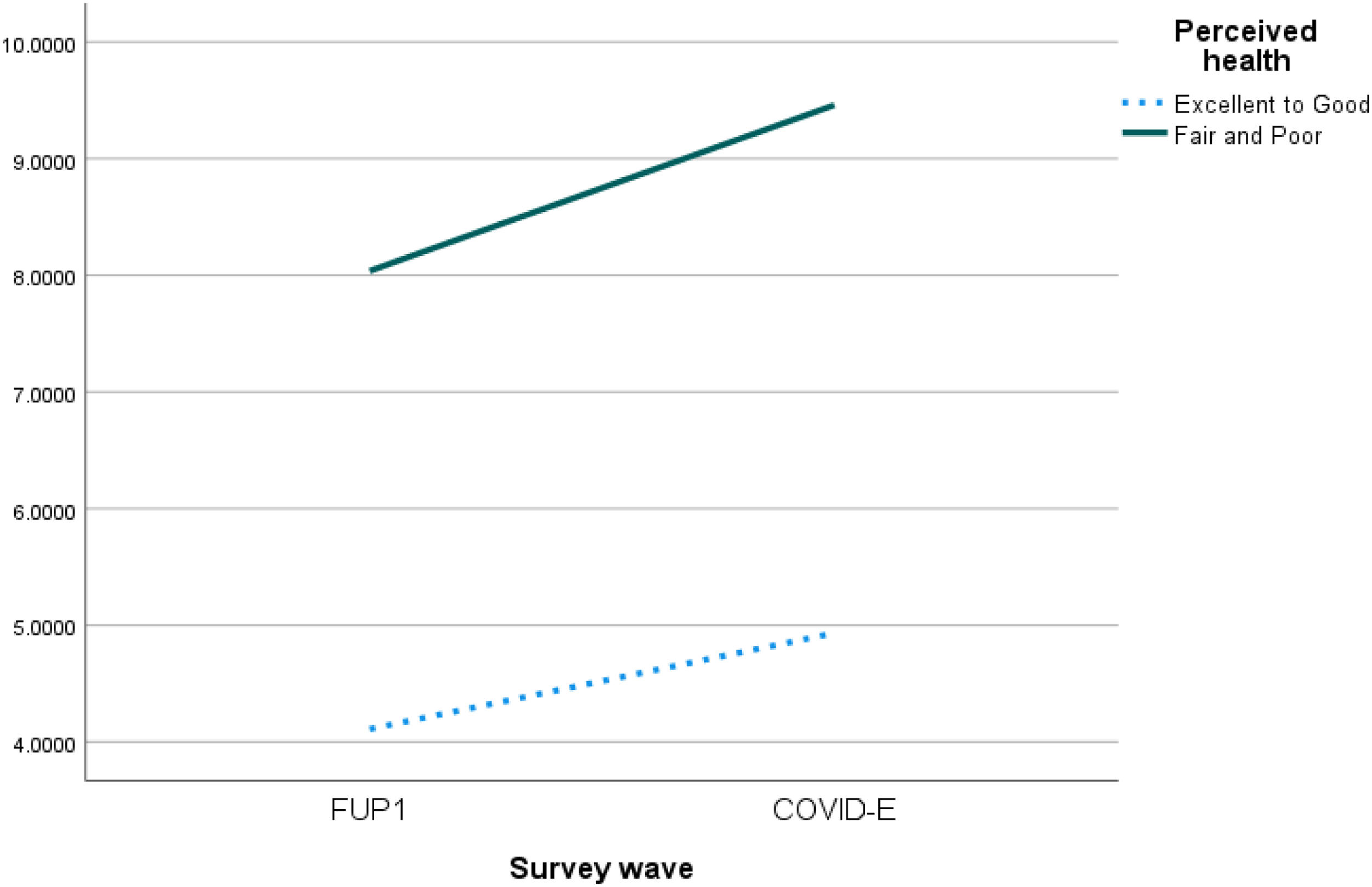
Neither of the interaction effects between caregiving status and loneliness, as well as for multimorbidity and loneliness, and perceived health and loneliness on depression symptoms were found (not shown in tables).
Discussion
Building on the understanding that the COVID-19 pandemic produces short- and long-term risk sequalae affecting quality of life, including psychological well-being, distress, anxiety, depression, and social isolation, this study focussed on the association between loneliness and depressive symptoms through an analysis of pre-pandemic and peri-pandemic (2020 waves) contexts. Research to date has been equivocal due to design limitations, such as small samples and cross-sectional studies incapable of disentangling likely bidirectional effects between loneliness and depression; measurement problems of key variables; and confounding effects of covariates. This paper is novel in its use of a large national longitudinal data set (CLSA) with multiple time points; sophisticated data analytic techniques (LMMs) that incorporate change over time; robust measures of loneliness and depression, and inclusion of a comprehensive set of covariates drawn from pandemic research on this topic.
This study provides strong evidence that loneliness worsens depressive symptoms pre-pandemic; and, moreover, the increase in level of loneliness during the early waves of the 2020 pandemic was also associated with worsening depressive symptoms. These results were again supported but slightly attenuated when associations were adjusted for twelve socio-demographic, caregiving, and health-related covariates identified in the burgeoning literature on factors affecting depression during the pandemic (Erbiçer et al., 2021; Raina et al., 2022; Robb et al., 2020; Van Tilburg et al., 2020; Wister et al., 2022d). The association between loneliness and caregiving status, as well as with perceived health and multimorbidity, did not vary as a function of depressive symptoms.
The results of the present research are consistent with a few small (>200) cross-sectional and longitudinal studies undertaken during the pandemic supporting associations between loneliness and depression or depressive symptoms (e.g., Kotwal et al., 2021; Krendl & Perry, 2021); as well as larger (<1000) ones (e.g., Mistry et al., 2021; Robb et al., 2020). Additionally, several descriptive and qualitative studies supported the results of the present study. For instance, Whitehead and Torossian (2021) found that loneliness or isolation was the third most frequently identified stressor that individuals in their study experienced during the pandemic, with older women, those with low-income, and unattached older adults ranking it first. The present findings diverge; however, from other research that has shown that loneliness or social isolation and mental health outcomes did not increase during the pandemic, and that older adults may have fared better than other age groups (Carney et al., 2021; De Bruin, 2021). These inconsistencies might be due to variation in populations, samples, measures (social isolation or loneliness), and pandemic waves.
By providing a rationale for links between pandemic stress, perceptions of loneliness and negative mental health outcomes in the form of worsening depressive symptoms coping (Lazarus & Folkman, 1984, 1987; Minahan et al., 2021; Whitehead, 2021), the TSM frames the present findings. The TSM also leads to an understanding of how appraisals of stress embedded in the profound experiences of living through a global pandemic can augment depressive symptoms when there are heightened perceptions of loneliness (Whitehead, 2021). Negative appraisals that may lead to loneliness may occur due to perceived susceptibility or seriousness of infection, pessimism, or maladaptive behavioral responses such as restricting travel to obtain important necessities, and other psycho-social processes. Furthermore, whether this is due to the lack of social connectedness, a combination of deleterious synergetic stressor effects, or erosion of fortitude under chronic periods of stress requires further study. Additionally, future studies may benefit by incorporating a resilience lens, which can explain why some individuals who have greater resources (e.g., structural and functional social support) are better able to adapt to the deleterious effects of pandemic adversity (Levasseur et al., 2017; Riehm et al., 2021; Wister & Speechley, 2020).
Several covariates also displayed important associations with depressive symptoms. The present study supports that younger older adults had slightly more depressive symptoms. This finding is consistent with other research suggesting that the very old fared better than the young-old or middle-aged (aged 50–65) (Carney et al., 2021; De Bruin, 2021), which might be due to having greater experience with disasters (e.g., wars), or fewer social interaction needs. Non-married/partnered individuals reported a smaller increasing of depressive symptoms than their counterparts, suggesting that partner status can protect against symptoms of depression and may provide more social participation opportunities. Although those without post-secondary education reported a smaller rise in depressive symptoms than higher educated perhaps due to attitudes and perceptions about the seriousness of COVID-19, individuals not working and those with lower incomes had greater increases in depressive symptoms during the early pandemic period. Unsurprisingly, a precarious financial situation exacerbated depressive symptoms during these lock-down and mitigation periods (Raina et al., 2022). Those living in rural environments appeared to fare better than urbanites, who experienced more infection spread of COVID-19 (McFarlane, 2021). Caregivers reported a higher level of depressive symptoms than non-caregivers over time, which coincides with another study based on the CLSA showing a link between caregiver contexts and mental health outcomes during the pandemic (Wister et al., 2022d). Perhaps the added stress and demanding nature of the caregiver role exacerbated underlying depressive symptoms.
Finally, health factors were significantly related to depressive symptoms between the pre- and peri-pandemic survey points. Participants who rated their health better, and those who had better functional status (ADLs, IADLs) had fewer depressive symptoms over time, which were expected findings consistent with prior research showing that health status can influence depressive symptoms in older adults (see Chang-Quan et al., 2010 for review). The findings showing that depression varies according to functional status indicates that there can be an independent physiological as well as a social-psychological mechanism to depressive symptoms.
Limitations
Our study provides confirmatory evidence by focusing exclusively on loneliness and depressive symptoms based on a large national study. However, this study has some limitations. First, while this paper focuses on the first year (2020) of the pandemic, associations between loneliness and depressive symptoms also need to be examined during other time periods and waves of the disease. Second, similarly to Cacioppo et al. (2010), we removed one of the 10 items from the CES_D that overlapped with one item in the UCLA Loneliness scale. The internal consistency of the 9-item scale was similar to the original form. Third, participants of the CLSA tend to be Caucasian ethnicity and highly educated, and interpretation of results should be made with caution when applying the findings to other population groups. This research also needs to be expanded to more diverse populations. Fourth, the modest change in depression due to the interaction of loneliness and the pandemic effect indicates that the impact of the public health restrictions were notable but not apocalyptically severe.
Conclusions
Earlier pandemic research examining the effects of loneliness on depression and its symptoms has been fraught with many methodological limitations, in particular, a lack of generalizability, cross-sectional designs that are constrained in terms of addressing potential bi-directional effects, confounding effects of covariates, and measurement issues. These have led to equivocal and sometimes weak results in the literature. This study responds to these issues and demonstrates clear support for the predictor effect of loneliness on depressive symptoms among older adults during the first year of the COVID-19 pandemic. The loneliness association is not modified by caregiver status or multimorbidity, two important factors associated with pandemic mental health conditions. However, it should be noted that the physical distancing policies that were employed during the pandemic saved lives, regardless of their effect of increasing the association between loneliness and depression. Several covariates are also predictive of increases in depressive symptoms; however, the effect of loneliness remains robust.
There are several important implications of this research for the current and future pandemics that may also have general applications. Addressing depressive symptoms and general mental health among older persons requires a multipronged approach that integrates the fostering of social connections among those at high risk of loneliness and social isolation in conjunction with management of depressive symptoms. From a health prevention perspective, interventions that focus greater attention on reduction of loneliness and depression pre-pandemic as well as early in a crisis are warranted, such as the phone-based Seniors Centres Without Walls Program (Newall & Menec, 2015) and related outreach programs to isolated older adults, as well as telehealth counselling and educational programs that enhance coping with isolation during periods of lockdown) (Van Tilburg et al., 2020). Clinicians responsible for high risk populations, especially those in health care settings, need to employ interventions early in a pandemic, such as early response teams (Kim et al., 2020). Interventions require identification of external support systems so that potential resources can be enhanced by fortifying the unique strengths and circumstances (resilience) of an individual, community or system to increase social connections and reduce depressive symptoms.
Footnotes
Acknowledgements
This research has been conducted using the CLSA Baseline Data Version 3.7 (tracking cohort) and 6.0 (comprehensive cohort), CLSA follow up 1 Data Version 2.2 (tracking cohort) and 3.0 (comprehensive cohort), and CLSA COVID-19 Data Version 1 (under Application Number 2104007 (![]() ). The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. Parminder Raina holds the Raymond and Margaret Labarge Chair in Optimal Aging and Knowledge Application for Optimal Aging, is the Director of the McMaster Institute for Research on Aging and the Labarge Centre for Mobility in Aging, and holds a Tier 1 Canada Research Chair in Geroscience.
). The CLSA is led by Drs. Parminder Raina, Christina Wolfson and Susan Kirkland. Parminder Raina holds the Raymond and Margaret Labarge Chair in Optimal Aging and Knowledge Application for Optimal Aging, is the Director of the McMaster Institute for Research on Aging and the Labarge Centre for Mobility in Aging, and holds a Tier 1 Canada Research Chair in Geroscience.
Author Contributions
A.W.—Main writer of manuscript; L.L.—Statistical analyses, methods and results drafting; All other authors made substantial contributions to the conception, design and editing of the manuscript, and interpretation of the data. All authors have read and approved the final version of the manuscript and have agreed to be accountable for all parts.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the support of the CLSA COVID-19 Questionnaire based study is provided by Juravinski Research Institute, Faculty of Health Sciences, McMaster University, Provost Fund from McMaster University, McMaster Institute for Research on Aging, Public Health Agency of Canada and Government of Nova Scotia. Funding for the Canadian Longitudinal Study on Aging (CLSA) is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference: LSA 94473 and the Canada Foundation for Innovation, as well as the following provinces, Newfoundland, Nova Scotia, Quebec, Ontario, Manitoba, Alberta, and British Columbia. Lauren Griffith is supported by the McLaughlin Foundation Professorship in Population and Public Health. Mélanie Levasseur is a Fonds de la recherche en santé du Québec Senior Researcher (#298996; 2021-2025).
Research Ethics and Patient Consent
This current project received ethics approval at two levels. Consent to participate was obtained for all participants under the CLSA harmonized multi-university ethics process approved by the Hamilton Integrated Research Ethics Board (HiREB), Hamilton Health Sciences/McMaster University. Written informed consent was obtained from all CLSA participants prior to enrollment. Individuals who were not deemed to be cognitively functional were excluded from the CLSA study. Simon Fraser University (SFU) was a participating institution in the CLSA data collection (SFU ORS #2010s0281), and the McMaster Research Services Ethics Committee reviewed all consent material prior to data collection.