
Abstract
Introduction
Removable partial dentures are a simple, cost-effective treatment for tooth replacement in partially edentulous patients (Campbell et al., 2017). Removable partial dentures commonly have clasps that impart retention force to the dentures. Basically, wearing a denture means putting a new prosthesis in the oral cavity. This may be accompanied by various complications and trauma, including life-threatening bleeding (Boon Tat et al., 2018; Helft et al., 1986). Among these complications, the most confusing denture-associated injury is aspiration of the denture with a particularly sharp clasp, often resulting in esophageal mucosal impaction and ultimately perforation, risking major consequences such as deep neck infections, mediastinitis, and peritonitis (Gachabayov et al., 2015; Toshima et al., 2011). Because of the specific findings, cases of denture aspiration have often been reported.
Among denture-related injuries seen in the emergency room, penetration of the clasp into the oral mucosa can result from the clasp not releasing from the abutment tooth easily enough (Figure 1). Clasp-penetrating injury of the oral mucosa is usually superficial and is generally considered relatively insignificant mucosal trauma, so the precise etiology and details have not been studied in detail. However, this injury can be accompanied by complications such as the stress and emotional frustration from not being able to remove the clasp and continuous bleeding.

An example of clasp injury of the oral mucosa. The lingual arm (arrowhead) of the double-toothed clasp has pierced the floor of the mouth.
Older adults sometimes experience difficulty with inserting and removing dentures (Kawasaki et al., 2012). As the denture-using population is increasing in aging societies, increases in denture-associated injuries such as clasp-penetrating injury of the oral mucosa can be expected.
The purpose of this study was to provide an overview and to identify factors associated with clasp-penetrating injury of the oral mucosa. We hypothesized that the design of the denture itself, which causes the clasp injury, may be associated with specific injury characteristics. The primary aim of the present study was to identify variables associated with clasp injury to the oral mucosa.
Materials and Methods
This study was designed according to the Declaration of Helsinki and Good Clinical Practice guidelines; further, it was approved by the Ethics Committee of Saitama Medical Center, Saitama Medical University (2021-101). To address the research purpose, we designed and implemented this study using a retrospective design. The study population entirely comprised patients with clasp-penetrating injury to the oral mucosa involving partial removal dentures treated by oral surgeons in the Emergency Room from April 2011 to May 2021 (the Center is a regional institutional hospital with 24-hr urgent care services). Patients in this study excluded those with hand disorders that could affect the insertion and removal of dentures. Patients with hand disorders include, for example, those who have suffered a stroke and have impaired hand movements. Patient data were obtained from clinical records. The primary outcome variable was clasp injury to the oral mucosa. Potential predictive variables included patient demographics, time of injury, past and current medical histories and medications, local characteristics, and denture incompatibility. Ages were sub-grouped into 10-year strata and injury times were categorized by 6-hr intervals. Past and current medical histories and medication were limited to those considered potentially associated with the cause, condition, or treatment of clasp injury, including factors such as bleeding tendency and dementia. Bleeding tendency is an exacerbating factor for trauma, and dementia is known to be associated with denture handling (Kubo et al., 2007). Bleeding tendency included use of anticoagulants. Local characteristics included site of the denture, site of the involved clasp, and site of the injured soft tissue. Denture incompatibility included complications of not only the dentures themselves, but also residual teeth related to dentures. In cases of injuries with precise information on denture design, including the abutment tooth associated with the involved clasp, the type of denture and abutment tooth were examined. The type of denture was divided into four categories according to the Kennedy classification: Class I, edentulous areas present bilaterally, posterior to remaining natural teeth; Class II, edentulous area present unilaterally, posterior to remaining natural teeth; Class III, edentulous area present unilaterally, with natural teeth both anteriorly and posteriorly; and Class IV, single edentulous area present bilaterally, anterior to remaining natural teeth (Figure 2) (Miller, 1970). Treatment methods were divided into two categories: manual removal alone; and requiring more than manual removal, including cases in which hemostasis was achieved by suturing, use of topical hemostatic agents, and extraction of abutment tooth, at least under local anesthesia.

Kennedy classifications of removable partial dentures.
All statistical analyses were performed using js-STAR version 9 software (http://www.kisnet.or.jp/nappa/software/star/index.htm; accessed August 5, 2022). The collected data were analyzed using the χ2-test or Fisher’s exact test. Multivariate analysis using the Cox proportional hazards model or logistic regression analysis was not performed due to the small size of the study cohort. For all tests, the significance level was set at 5% (p < .05).
Results
A total of 82 patients were initially identified for potential inclusion in this study. Nine patients were excluded from the study due to insufficient or missing records, leaving a total of 73 patients. The 73 patients comprised 36 men (49.3%) and 37 women (50.7%), giving a male-to-female ratio of 1:1.03. Mean (±standard deviation) age was 72.8 ± 12.7 years. In terms of age distribution, clasp-penetrating injuries were less common among patients <50 years old and increased among those ≥50 years old. Percentages of patients in the age strata of 50 to 59, 60 to 69, 70 to 79, and ≥80 years were 12.3%, 16.4%, 34.2%, and 32.9%, respectively. The age strata most commonly involved were thus 70 to 79 years and ≥80 years, but no significant differences in group size were evident among the three age strata ≥60 years (p = .119) (Table 1). Injuries mostly occurred between 18:00 and midnight (67.1%; p < .001) (Table 1). As a clinical variable, bleeding tendency (11, 15.1%) was significantly less common than no bleeding tendency (62, 84.9%) (p < .001) (Table 2). However, bleeding at the time of visit was significantly more common in patients with bleeding tendency (36.4%) than in patients with no bleeding tendency (6.5%; p < .05) (Table 3). Absence of dementia (67, 91.8%) was significantly more frequent than its presence (6, 8.2%) (p < .001) (Table 2). As a local characteristic, the involved denture was significantly more often a mandibular denture (67, 91.8%) than a maxillary denture (6, 8.2%; p < .001) (Table 4). No significant difference was seen in laterality of the involved clasp (right, 47.9%; left, 52.1%) (p = .408) (Table 3). The most frequent site of the affected oral soft tissue was the tongue (46, 63.0%), followed by gingiva (15, 20.5%), floor of the mouth (10, 13.7%), lower lip (1, 1.4%), and buccal mucosa (1, 1.4%). Further, lingual-side soft tissues including the tongue and floor of the mouth were significantly more frequently affected than other tissues (p < .001) (Table 4). No significant difference was seen in the presence (32, 43.8%) or absence (41, 56.2%) of denture incompatibility (p = .175) (Table 4). Precise information on the type of denture and abutment tooth associated with the involved clasp were available for 31 cases, comprising 4 maxillary dentures and 27 mandibular dentures. Kennedy classification was most frequently Class I (16, 51.6%), followed by Class II (10, 32.3%), Class III (3, 9.7%), and Class IV (2, 6.6%). Class I and II free-end saddle dentures were significantly more frequently involved than Class III and IV (p < .001) (Table 5). The abutment tooth associated with the involved clasp was most frequently a premolar (20, 64.5%), followed by a canine (10, 32.3%) or molar (1, 3.2%) (Table 4). Premolars and canines were significantly more common than incisors and molars (p < .001) (Table 5). In terms of treatment, cases of manual removal alone (50, 68.5%) were significantly more frequent than cases requiring more than manual removal (23, 31.5%; p = .001) (Table 6).
Demographic Characteristics and Time of Injury for Included Patients.

Note. SD = standard deviation.
Clinical Characteristics of Patients.

Note. Bleeding tendency includes anemia and use of anticoagulants.
Relationship Between Bleeding Tendency and Bleeding at Time of Visit.

Note. Bleeding tendency includes anemia and use of anticoagulants.
Local Characteristics of Clasp Injury.
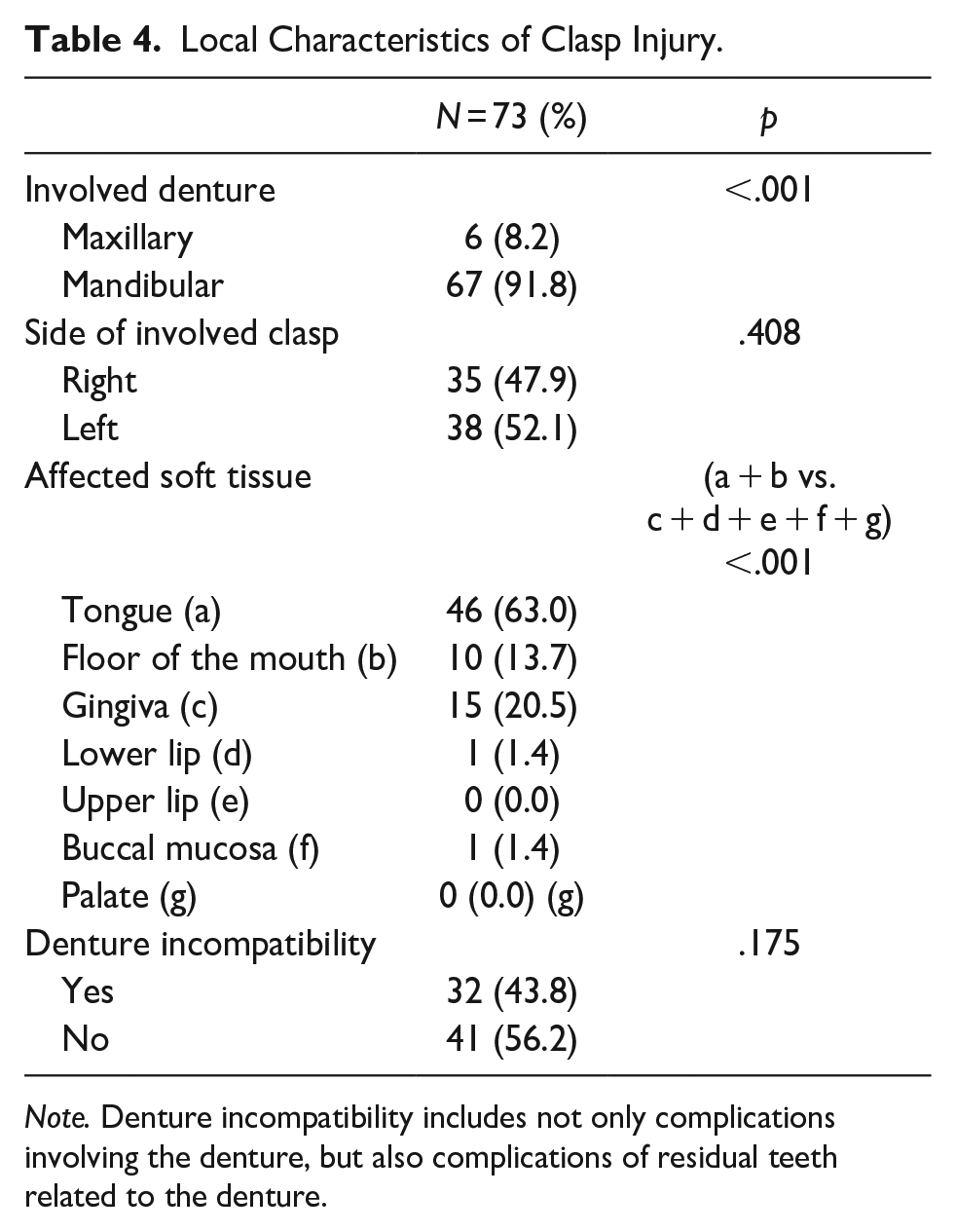
Note. Denture incompatibility includes not only complications involving the denture, but also complications of residual teeth related to the denture.
Characteristics of Involved Dentures.

Including four cases of maxillary denture.
Treatment Methods of Clasp Injury.

“Manual removal alone” included three cases requiring bending or cutting of clasp.
“Requiring more than manual removal” included cases in which hemostasis was performed by suturing, use of topical hemostatic agents, and extraction of abutment tooth, at least under local anesthesia.
Discussion
This study studied the characteristics of clasp-penetrating injury of the oral mucosa from removable partial dentures. Mandibular free-end saddle dentures with premolar or canine clasps showed the highest risk of causing injury.
No sex difference in clasp trauma was seen. In terms of age, this injury was rarely observed in individuals under 50 years old, as this population had few dentures. The proportion of cases increased from the 50s, peaking in the 70s and 80s. It has been described that the ability or inability to use dentures is not related to age and that dementia, rather than physical function, makes it more difficult to wear dentures (Minakuchi et al., 2006; Taji et al., 2005) The lack of significant differences in the frequency of injury among individuals over 60 years old wearing dentures may suggest that the physical functional decline seen with older age does not necessarily contribute to the risk of clasp injury. Injuries were significantly more likely to be sustained in the evening (p < .001), potentially due to a greater number of opportunities for removing dentures at night after eating and before going to bed. Patients with clasp injuries often visited the emergency room with the chief complaint of continued bleeding, and bleeding tendency is a factor that increases bleeding during trauma. Patients were then examined for bleeding tendencies to search for bleeding effects. The results showed significantly fewer patients with bleeding tendencies (p < .001). However, bleeding at the time of visit was significantly more frequent among patients with bleeding tendency (p < .05). For patient with bleeding tendencies, clasp injuries would logically be prone to result in more bleeding. However, in this study, one patient with no bleeding tendency showed persistent, difficult-to-hemostatic bleeding (Figure 3). In cases of clasp injury, wound hemostasis may be more strongly affected by a greater extent of soft tissue damage than by underlying bleeding tendency.

A 72-year-old woman with no bleeding tendency. (A) Oral view shows persistent, difficult-to-hemostatic bleeding from the right side of the tongue. (B) The removed denture (arrow indicates the involved clasp).
Dementia was present in only 8.2% of affected patients (p < .001). This may be because this study did not include patients with advanced dementia who cannot handle their dentures themselves, that is, those who do not wear dentures. Older adults with mild to moderate dementia are considered able to insert and remove dentures without assistance (Kubo et al., 2007). Older adults with severe dementia, on the other hand, reportedly take significantly longer to remove partial dentures due to disorientation (Kubo et al., 2007). This may also contribute to clasp injuries. In an unusual case included in the present study, a dementia patient suffered clasp-penetrating oral injury late on the same day that the denture was aspirated and endoscopically removed. How long dentures should continue to be used by patients with dementia should definitely be examined in future research.
Mandibular dentures were significantly more commonly involved than maxillary dentures (67, 91.8%, p < .001). The tongue is obviously a major obstacle to the insertion and removal of mandibular dentures. This was reflected in the fact that the injured site was frequently lingual-side soft tissues, such as the tongue (63.0%) and floor of the mouth (13.7%) (p < .001). Since the tongue and floor of the mouth are soft, the clasp can penetrate deeper depending on the movement of the denture.
Denture incompatibility was not a significant cause of clasp injury. This means that clasp injury can occur in any oral environment or with any denture fit. The only problem may be whether patients are good at removing their dentures.
Regarding the type of denture, various systems are used to classify edentulous spaces. The Kennedy classification system is simple and widely used (Miller, 1970), and so was adopted in this study. Class I (51.6%) and Class II (32.9%) were significantly more common than Class III (9.7%) or Class IV (6.6%) (p < .001), and both Class I and Class II dentures are free-end saddle dentures. From the site of the affected clasp, premolars (64.5%) and canines (32.3%) were significantly more common as abutment teeth for the penetrating clasp (p < .001). Premolars and canines are common abutment teeth used in Class I and Class II dentures, which involve missing molars. These results suggest that clasp-penetrating injury is more likely when lifting a free-end saddle denture with a premolar or canine clasp. Clasp arms for premolars and canines, such as Akers’ clasp, are short and involve strong angulation compared to clasps for molars, and so may be difficult to remove after becoming embedded in soft tissue (Owen & Naidoo, 2022). Of course, various types of clasps are in use. Whether differences in the risk of penetration are seen according to the type of clasp is an issue for future study.
As for treatment, clasp-penetrating injuries were typically minor, with manual removal alone the most common intervention (68.5%; p = .001). However, one-third of cases required more than simple manual removal, so clinicians should always be prepared with measures to stop bleeding.
As a preventive measure, dentures that are easier to insert and remove may prove beneficial (Davenport et al., 2000; Manzon et al., 2019). In particular, adjustment of free-end saddle dentures of the mandible is important, and clinicians should also carefully explain to patients how to remove the denture without pinching soft tissue. Regular oral examinations including denture adjustment would likely prove helpful. Patients should also be advised that if a clasp becomes caught, strong efforts to achieve removal should not be attempted. Forceful attempts at removing the clasp may exacerbate tissue injury and bleeding, so early consultation is recommended. In another case included in the present study, the patient dislocated a temporomandibular joint by inserting a finger deep into the mouth in an attempt to remove the embedded denture.
As limitations to this study, the sample size was relatively small and sufficient information on dentures was difficult to collect due to the retrospective design. If more detailed form and usage histories from more cases could be obtained, denture-related factors associated with complications may be better elucidated.
In conclusion, clasp-penetrating injury of the oral mucosa was significantly more common for the tongue, and mandibular free-end saddle dentures with premolar or canine clasps were the most prominent risk factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.