
Abstract
The risks of iatrogenic medication related adverse events are high among older patients. Assessing prescriptions is critical to prevent overusing, underusing, or misusing medications. The aim of this study is to evaluate the prescription reassessment in older patients hospitalized in long-term care unit. Among the 30 patients (Mage = 83 years, woman 66%), polymedication was present, patients taking 5 to 18 drugs (mean 11 drugs). The length of stay varied from 92 days to 4.5 years (mean 564 ± 430 days). The prescription reassessment of the patients hospitalized in our long-term care unit varied from 1 to 125 days with a mean of 16 days. Plan the prescription reassessment could reduce the iatrogenic medication in weakened patients.
Introduction
Long-term Care Units (LCU) provide medical and non-medical support to older patients with chronic diseases that are either active on the long term or prone to recurring episodes resulting to degradation or loss of autonomy (Direction de l’hospitalisation et de l’organisation des soins, 2006). LCU patients usually present with stroke, brain vascular affections, neurodegenerative illnesses like Alzheimer’s disease, psychiatric disorders, and other organic chronic diseases causing handicap. Therefore, the health condition of LCU patients theoretically require follow-up with regular medical care. This population is highly exposed to polymedication and therefore drug-induced iatrogenesis. Reducing iatrogeny, with its consequences on both personal and economical scales, represents a public health issue for French regional health agencies (Ponte, 2008). A part of this iatrogeny is the result of medication errors that are, by definition, foreseeable. These medication errors may be associated with defects in the organization of the medication management steps and inadequate or insufficiently reevaluated prescriptions. Studies based on the use of these lists have shown that the quality of prescriptions in geriatrics is usually poor. In the United States, 3% to 46% of older patients are exposed to potentially inappropriate medications; a similar proportion is encountered in Europe (6%–41%) and a higher one in Asia (12%–70%; Laroche et al., 2009). The existence of numerous diseases, and therefore polypharmacy, raises the risk of non-compliance, drug interactions, and adverse events including relapse, falls, and mortality (Saum et al., 2017; Wimmer et al., 2017).
Older patients with a greater degree of frailty may be particularly vulnerable to adverse drug reactions. Studies have detected potentially inappropriate medications (PIM) and potential prescribing omissions (PPO) in geriatric populations receiving long-term care (Candeias et al., 2021). In these studied patients, PIMs were detected in 85.1% and PPOs in 81.4% of patients. In a French prospective observational study, PIM were detected in 46% of older inpatients. Psychotropic (36%), cardiovascular (29%), and laxative drugs (16%) were the most-frequent classes prescribed. This underlines the need for accurate guidelines on PIM monitoring (Pandraud-Riguet et al., 2017).
The aim of this study is to assess the frequency of the re-evaluation of medical prescriptions in older patients hospitalized at long-term care unit.
Methods
An observational and retrospective study was performed in 30 patients aged 65 years and over from long-term care unit in the geriatric Paul Doumer hospital, between January and June 2022. This was limited by the representativeness and typology of the patients who stay in the unit until the end of life. According to patient needs and goals established, the length of stay extended from admission to death of patient. All patients were monitored by various professionals such as physicians, nurses, physiotherapists, psychologists, nutritionists, and pharmacists. The retrospective approach of the study had no impact on patient care, and informed consent was not required. Patients’ data were anonymized through the assignment of an alphanumeric code and access restricted to the first author. The further assessment was carried out purely on the coded data.
Data were mainly collected from the patients’ electronic records. All relevant patient information are documented in these electronic records, i.e. discharge summaries, periodic assessments by different professionals, diagnoses, prescribed medication, medical examinations, nutritional status, level of dependence in the daily life activities, and results of assessment scales (e.g., risk of falling and pain assessment).
For each patient, a pharmacist analyzed the demographic and clinic data, level of dependency in daily life activities using the Autonomy Gerontology Iso-Resources Groups (AGGIR) scale, medications, and the length of stay. The AGGIR scale is an autonomy assessment tool used in France for measuring the independency level of elderly people (Aguilova et al., 2014). This scale covers so-called instrumental dimensions that correspond to relatively complex activities with the dominating cognitive component (cooking, medication use, finances, etc.) as well as dimensions with the dominating physical component (fundamental dimensions that are related to such activities as walking, dressing, toileting, etc.). The scale classified the older adults into homogeneous groups from AGGIR1 meaning dependency in all daily activities to AGGIR 6 meaning total functional autonomy.
Results
Table 1 shows inpatients characteristics. The mean age of patients was relatively high at 83 ± 9 years old with a sex ratio of 2:1 (Female/Male). Majority of patients were classified AGGIR2 including patients confined to bed or chair with cognitive impairment and requiring care for most daily life activities. Eight patients (27%) were classified AGGIR1 including patients confined to bed or chair with impaired cognitive functions and requiring ongoing presence of caregivers. All patients were polypathologic and polymedicated taking between 5 and 18 drugs (mean 11 ± 4). At the end of the study, the length of stay varied from 92 days to 4.5 years (mean 564 ± 430 days). The prescription reassessment of the inpatients hospitalized in our long-term care unit varied from 1 to 125 days with a mean of 16 days. The repartition of the prescription reassessment is defined by a very strong heterogeneity for the global cohort or the same patient.
Characteristics of Patients.
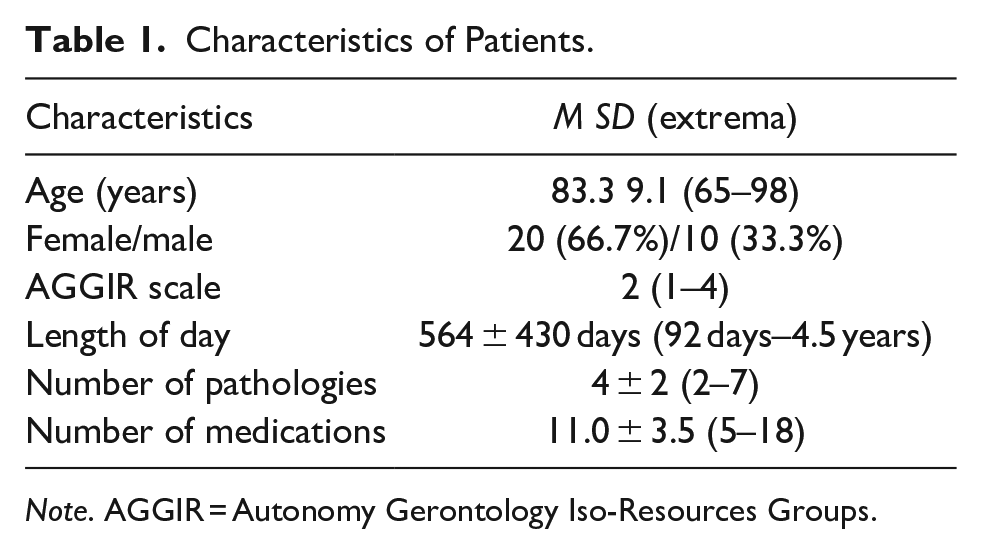
Note. AGGIR = Autonomy Gerontology Iso-Resources Groups.
Discussion
The risks of iatrogenic medication are especially high among older patients because of frequent polymedication or pharmacokinetic and pharmacodynamic modifications related to aging (Andro et al., 2012; Hämmerlein et al., 1998). Assessing prescriptions regularly is critical to prevent overusing, underusing, or misusing medications. In particular, some studies have demonstrated the benefit of monitoring potentially inappropriate prescriptions in the older patients (Bongue et al., 2011; Candeias et al., 2021; Pandraud-Riguet et al., 2017; Saqlain et al., 2020). Even though extensive literature on inappropriate prescribing is growing over the last decade, no data are available on the required frequency of reassessment to ensure optimal prescribing. Based on the frequency and severity of adverse drug reactions related to suboptimal monitoring, defining the frequency of reassessment would be beneficial for optimal prescribing with alerts generated to enable specific responses in these cases. This brief report highlights the wide heterogeneity of prescription reassessment in the older patients. Scheduling the reassessment of prescriptions based on criteria such as number of medications prescribed, occurrence of inappropriate medications, physiological, and psychological characteristics of the patient, would contribute to better medication management in the elderly.
Conclusion
This report indicated that the reassessment of medical prescriptions are widely heterogeneous. However, this is a practice study with limited number of patients. Thus, further investigation is required focusing on the relationship between clinically relevant adverse events and reassessment frequency of inappropriate prescriptions in older population. The future objective is to establish a checklist selecting the patient to be selected for an optimal reassessment prescription.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The patients gave their oral informed consent to use their anonymized data. Our institutional ethics review board gave its approval to use the information in database.
Data Sharing Statement
The data of patients were acquired from the electronic database of our hospital, including demographic information, laboratory results, and treatment details.