
Abstract
Cultural and social factors significantly influence the care provided to persons with dementia. This scoping review aimed to map emerging evidence on the influence of cultural and social factors on care delivery among Africa American caregivers of persons with dementia, especially during the COVID-19 pandemic. Using a systematic scoping review approach, we identified 21 studies on cultural and social factors influencing care delivery. The search included EMBASE, CINAHL, the Cochrane Database of Systematic Reviews, JBI Evidence Synthesis, and Epistemonicos. A narrative synthesis of the data revealed that cultural and social factors greatly influence African American caregivers of persons with dementia and COVID-19 in care delivery, who perceive caregiving as a responsibility and not just a job. These caregivers are additionally guided by their racial identity and faith beliefs, integrating family values and culture into caregiving. African American caregivers showed compassion and resilient care selfperceptions. Supporting compassionate care delivery by African American caregivers requires an understanding of the social and cultural factors which drive their commitment to quality care for older adults with dementia in a pandemic environment.
Keywords
Introduction
The population of older adults worldwide, especially in the United States, is rapidly multiplying because people live longer now than 100 years ago (United Nations, 2022). The United Nations further projected that the global population of older persons 65 years and above would reach approximately 1.5 billion by 2050, up from the current 56 million older adults in 2022. As a result, caregiving has become integral to ensuring a better quality of life for the aging population, especially those with dementia and, most recently, the complications of COVID-19. The growing need for the care of this population is a worldwide phenomenon. In addition, it has proven to be a robust health and wellbeing risk factor due to dementia exacerbated by COVID-19 and its associated symptoms.
It is estimated that about 46.8 million people worldwide live with dementia (Prince et al., 2015, 2016). This number is expected to reach about 74.7 million by 2030 and approximately 131.5 million in 2050 (Prince et al., 2015, 2016), mainly due to natural processes of aging and increased longevity. Dementia affects caregivers’ health unfavorably compared to other disorders because of the needs and demands of providing care to persons with the condition (Alzheimer’s Association, 2016, 2019).
The World Health Organization [WHO] (2017) recognized the complexity of dementia as a disability that causes dependency. This requires prioritization through the “Global action plan on the public health response to dementia 2017 – 2025,” a targeted global health intervention policy with specific “Action Area 5,” which is geared to ensure that support is provided to caregivers of persons with dementia. One target tasks 75% of member-state governments to offer psychological, physical, and economic support and training for caregivers and families of persons with dementia by 2025 (WHO, 2017). This training can help improve coping mechanisms for the overall health condition of caregivers and provide a basis for quality healthcare delivery.
Studies show that over 30 million Americans spend more than $100 billion annually providing unpaid and informal caregiving services for over 3 million older Americans, 50 and over, with dementia (Family Caregiver Alliance, 2022; Sloane et al., 2002). Despite this financial investment, formal and informal dementia care systems experience complex care quality problems (Fortinsky et al., 2009). Caregivers of persons with dementia have consistently revealed high rates of depression, stress, and other psychological issues compared to caregivers of persons with different ailments (Covinsky & Yaffe, 2004; Schulz et al., 2008).
The effects of caregiving are more pronounced for persons providing care to persons with dementia due to the eccentric challenges of the cognitive and physical decline experienced (Schulz et al., 2008), and very often, the extended period of care in any context takes a toll on caregivers (Catalano et al., 2018). Studies have also shown substantial disparities in the prevalence of Alzheimer’s disease among minority populations, especially African Americans, who are twice as likely to develop late-onset Alzheimer’s disease than their Caucasian counterparts (Alzheimer’s Association, 2022). In addition, previous research has shown that myths and beliefs surrounding dementia within the African American community have advanced the wrong knowledge and understanding of the disease, thereby causing increased stress and difficulty among family caregivers (Cox, 1999; Green & King, 2009). For example, many black communities believe that dementia is an inevitable part of aging and that some interventions to arrest or alleviate it can yield positive results while aging in place or with family.
Conversely, some older persons are immediately relegated to a highly medicated life in a group home or assisted living, with many confined to bed, with no external stimulation or exercises, proven to alleviate the progression of dementia. Some psychosocial interventions by African American Alzheimer’s caregivers have decreased caregiver burden and stress (Dang et al., 2008). For example, a study by Oliver et al. (2022) stated that African American caregivers provided better care to persons with dementia and Covid-19 than other ethnic groups. They take better care of the family at home in an environment filled with other family members and more mental stimulation. However, informal African American caregivers of persons with dementia report less access to support services compared to other ethnic counterparts (Fabius et al., 2020). They also engage in more hours of care delivery and assign a large part of their income to ensure care provision compared to other ethnic groups (Cohen et al., 2019; Fabius et al., 2020). Nevertheless, the advent of COVID-19 resulted in unprecedented mortality among older adults (Ameis et al., 2020), especially African American older adults with dementia (Oliver et al., 2022).
African American older adults with dementia and their caregivers are highly vulnerable to stress from COVID-19 restrictions that have affected typical pre-pandemic activities according to the Centers for Disease Control and Prevention (Birhane et al., 2021). Despite all these challenges, African American caregivers still provide optimal care to persons with dementia and COVID-19. However, there is insufficient research on the effect, importance, and evaluation of social and cultural factors influencing care delivery interventions by African American caregiver populations. Therefore, we aimed to scope and synthesize emerging evidence of social and cultural factors influencing quality care delivery among the African American caregiver population for persons with dementia, especially during the COVID-19 pandemic when the need for caregivers is increasing with continued elevated risk factors.
Review of the Literature
Dementia Care and African American Caregivers
Dementia is a debilitating chronic condition with a significant negative impact on the brain, presenting with cognitive decline (Bartzokis, 2004). Often progressive, affecting older adults above 65 years, it is characterized by mental and behavioral interferences (Guarino et al., 2019), contributing to susceptibility to other co-morbidities and ailments such as COVID-19 (Li et al., 2020). Older adults as a population are greatly affected by dementia, although all races may be vulnerable. For example, there is a marked prevalence of dementia between 14% and 100% among African American older adults compared to the non-Hispanic Caucasian population (Alzheimer’s Association, n.d.; Barnes et al., 2014). This anomaly is mainly a result of the lack of monetary resources and inequalities in healthcare accessibility for preventive care encountered by this racially disadvantaged population during their lifespan.
Informal caregivers are typically unpaid, and estimates indicate that over 15 million caregivers provide care and support for older adults with dementia (Alzheimer’s Association, n.d.; Family Caregiver Alliance, 2022; Moore et al., 2020). Formal caregivers can receive remuneration, nurse aide assistance, or grants for one or two aging adults in a home or registered care facility (Family Caregiver Alliance, 2022; Moore et al., 2020). A typical example of caregiving for seniors would be for parents or parents-in-law. While research has often focused on Caucasian caregivers, almost 40% are reported to be black, indigenous, or otherwise classified as people of color, known by the acronym BIPOC, with 13% identified as African American (Mental Health America, 2022).
The article further expounds on the fact that African American caregivers, who account for 13% of the total caregiver population of about 43 million, often feel the cultural pressure to provide this care, and the burden of care mainly falls on women (Family Caregiver Alliance, 2022). According to the Alzheimer’s Association (n.d.), this disease is caused by genetic and environmental factors, with its prevalence exacerbated by vascular disease in African Americans. Common untreated conditions such as cholesterol, diabetes, and hypertension contribute to developing vascular disease, especially where preventive healthcare is erratic in the black community. Healthcare access remains a negative factor in the early diagnosis of chronic conditions. Similarly, the diagnosis of dementia in this population often occurs much later compared to other racial groups, resulting in the delayed start of various interventions that can make a positive difference in disease progression.
Older adults have limited access to information, resources, and details about the COVID-19 pandemic. It is estimated that more than 50 million persons worldwide live with dementia, with new cases diagnosed every 3 s (Alzheimer’s Association, 2019). In the aging population, dementia looms as a co-pandemic with COVID-19, which has become of great concern to persons with dementia, their caregivers, and society. These conditions are exponentially worsened by health disparities prevalent among different racial groups. Available studies have shown that African American caregivers of older adults with dementia are greatly affected by access to resources, information, and timely healthcare access, thereby hindering quality healthcare for persons with dementia (Dilworth-Anderson et al., 2020; Lynch, 2020; Wallace Williams et al., 2003). Despite these challenges, African American caregivers have continuously shown resilience in care delivery (Roth et al., 2001).
The care for persons with dementia is multidimensional, involving the person with dementia, the caregiver, their family, and associated social and cultural factors. Many persons with dementia live in their community and receive necessary care from either families or care providers. The caregiver’s wellbeing and the quality of care they can provide largely depend on their resilience in handling issues related to the person with dementia, how well they understand the disease, and the cultural and social factors influencing their decisions for care. Some of the social and cultural factors include:
Relatedness. Providing care to persons with dementia varies depending on their relationship with persons with dementia and their closeness (Chiao et al., 2015). Studies show that spouses and their children experience the highest burden of providing unpaid care for persons with dementia (Kaizik et al., 2017; Moore et al., 2020). In addition, studies indicate that spouses who serve as caregivers of persons with dementia suffer from physical health issues, which leads to stress. The offspring of persons with dementia also help provide necessary care and assistance to the individual with dementia, especially for African American caregivers (Pinquart & Sörensen, 2011). Feelings of obligation and duty are the primary motivational factors associated with this care provision and delivery (Heinz, 2010; Mental Health America, 2022). However, the quality of relationships that existed before dementia onset influences the extent of the resilience exhibited, which positively improves the care burden and enhances the feeling of satisfaction experienced within the care delivery relationship (Lopez et al., 2005).
Social support. Delivering quality care to persons with dementia is highly influenced by their social relationships, which consist of social and family support (Challis et al., 2002; Dang et al., 2008). Social support is mainly viewed as a form of subjective appraisal consisting of appropriateness and availability of support received (Gomez & White, 2006). Satisfaction with this support is consequently perceived to be the most critical part because it helps cushion the effect of stress factors, impediments to care delivery, quality, and caregivers’ overall physical and psychological health (Parrish, 2019).
Religious beliefs and spirituality. Studies by Karlin (2004) and Picot et al. (1997) showed that religion greatly influences African American caregivers’ ability to provide care and improves caregivers coping skills and abilities. Other reports also discussed the positive impact of religious beliefs and spirituality on caregivers’ satisfaction (Margallo-Lana et al., 2001), social functioning (Karlin, 2004), burden level, and overall satisfaction with life (Meller, 2001).
Ethnicity and culture. These have greatly influenced caregivers’ care delivery skills, ability, and resilience. For example, some studies show that Caucasian caregivers of persons with dementia show high levels of depression and burden levels and decreased levels of caregiver’s satisfaction compared to African American caregivers of persons with dementia (Hilgeman et al., 2014; Kosberg et al., 2007; Roth et al., 2001). Also, studies show that African American and Hispanic caregivers of persons with dementia rely heavily on informal long-term care due to the culture of family caregiving for persons with dementia (Dilworth-Anderson & Gibson, 2002; Dilworth-Anderson et al., 2020; Gaugler et al., 2007).
Gender. The caregivers’ gender greatly influences experiences and perceptions of consistent provision of care (Ashley & Kleinpeter, 2002). For example, studies show that men report less need for social support and burden than women (Ashley & Kleinpeter, 2002). However, providing care is generally regarded as a woman’s task, thereby creating gender bias (Lee & Tang, 2015). In addition, men embody masculinity norms of limited emotionality and less engagement in caregiving duties than women (Given et al., 1999). Therefore, gender is a predictor of caregiving skills, abilities, and resilience in care delivery (Baker & Robertson, 2008).
African American Caregivers and Care Delivery
Care delivery impacts the health and wellbeing of persons with dementia and their caregivers. Additionally, the nature and outcome of caregiving differ in various racial and ethnic groups. Therefore, a good understanding of the complexities and social and cultural factors associated with dementia care will form the basis for a proper understanding of the physical and psychological health outcomes of individuals with dementia and their caregivers.
Compared with their Caucasian counterparts, a study reported that African American caregivers of persons with dementia have reported stress, depression, and burden (Aranda & Knight, 1997). Also, pragmatic indexes of wellbeing have shown the existence of loathsome dissatisfaction in care delivery among Caucasian caregivers of persons with dementia compared to African American caregivers (Roth et al., 2001). In fact, for the Caucasian caregivers of persons with dementia, life dissatisfaction increases over time compared to African American caregivers, who have shown to be stable over time (Roth et al., 2001). Generally, care delivery, especially to persons with dementia, often leads to an increased risk of mortality, abnormalities in health behavior, malfunctioning of the immune system, and poor overall health (Haley et al., 2000). Providing care to persons with dementia can be very demanding as the caregiver must always think and analyze more issues on behalf of the person with dementia. A longitudinal study by Roth et al. (2001) noted that African American caregivers of persons with dementia reported below-par physical health compared to Caucasian caregivers, who subsequently showed decreasing physical health indicators over time.
In addition to these appraisals for caregiving, key indicators such as religious coping have been compared between African American caregivers of persons with dementia and their Caucasian counterparts. These studies showed that reduced distress accompanying behavioral issues, burden, and self-care were reported among African American caregivers of persons with dementia (Haley et al., 2004; Miller et al., 1997). More comparative studies have also reported greater levels of caregiving satisfaction (Vasileiou et al., 2017), perceived recompense (Doris et al., 2018), and increased self-worth (Haley et al., 2000) for African American caregivers compared to their Caucasian counterparts.
Various studies have also insinuated religion, prayer, faith, and belief as principal coping mechanisms to care delivery issues among African American caregivers of persons with dementia (Dilworth-Anderson & Gibson, 2002). They are reported to be involved in more spiritual gaging and greater levels of dedication than Caucasian caregivers of persons with dementia (Picot et al., 1997). Social factors and culture have also proven to affect care delivery, various community coping mechanisms, sound family settings, and good healthcare systems, potentially influencing caregivers. Understanding the inequalities in providing care for persons with dementia involves a thorough understanding of the individual care needs, life experiences, and various support sources for these individuals.
Some studies have shown that culturally diverse caregivers share the same stressors, such as behavioral, work, and family-related issues. Still, culturally adapted interventions can bring about positive effects within them (Gallagher-Thompson, Coon, et al., 2003; Gallagher-Thompson, Haley, et al., 2003). Caregiver interventions for persons with dementia should be tailored to address the various cultures, resources, and social networks (Martindale-Adams et al., 2017). Also, improved psychological wellbeing of African American caregivers of persons with dementia compared to their Caucasian counterparts’ points to the fact that they carry out their caregiving roles with more dexterity and focus despite the inability to afford health resources and lower financial resources. This scoping review focuses on the social and cultural factors influencing caregiving among African American caregivers of persons with dementia during the COVID-19 pandemic.
Therefore, our research question is, “What are the sociocultural factors that motivate African American caregivers of persons with dementia, and how do these factors influence sustainable quality care delivery?” The scoping review seeks to gather data and inform the design of dementia caregiving interventions while engaging sociocultural factors adapted from African American caregivers’ perspectives. Moreover, the findings would provide a basis for further empirical studies on the quality-of-care delivery factors for older adults with dementia in the context of the Covid-19 pandemic.
Methods
Research Design
A scoping review is suitable for summarizing the emerging evidence on a newer and under-studied phenomenon for mapping the trends to guide future related studies with the benefit of clarification of concepts and study procedures (Peters et al., 2015, 2020). Also, scoping reviews are mainly conducted to deliver an overview of the existing evidence regardless of methodological quality or risk of bias since the studies are exploratory and the data are preliminary (Alexandre et al., 2018). Therefore, a scoping review was appropriate for this study for aggregating and profiling the emerging research evidence on social and cultural factors influencing African American caregivers of older adults with dementia for quality care delivery.
Search Procedure
We searched the following electronic databases: (EMBASE), CINAHL, Cochrane Database of Systematic Reviews, JBI Evidence Synthesis, and Epistemonicos, for studies on social and cultural factors influencing care delivery by African American caregivers of persons with dementia and COVID-19 mitigation (Table 1).
A Overview of Search Procedures, Including Key Topics and Search Terms.

Eligibility Criteria
The review’s inclusion criteria consisted of peer-reviewed empirical research across the continuum of qualitative randomized controlled trials to quantitative studies. To be included in this review, we considered studies from the past 3 years (December 2019–September 2022) on social and cultural factors influencing African American caregivers of persons with dementia with COVID-19 mitigation for sustainable care delivery. In addition, we included studies reported in English and excluded gray literature from the review and other information sources that were not peer-reviewed empirical studies. Table 2 summarizes the eligibility criteria of potential studies for the present scoping review.
Inclusion and Exclusion Criteria Per Study Variable.

Data Extraction
The first author performed the literature search supported by the co-authors. We prioritized essential data qualities of study design (i.e., qualitative, randomized controlled trials, quantitative), participant characteristics (i.e., Reported on an older adult sample specifying the ages and African American caregivers), interventions (i.e., types of social and cultural activities), and outcomes (sustainable and quality care delivery through the application of social and cultural factors from African American caregivers). Finally, we each examined the articles for their relevance to the topic and probable link to the inclusion criteria, resolving emerging disagreements by consensus.
Risk Bias Assessment
The “Risk of Bias” across studies, an element drawn from the PRISMA approach (Page et al., 2021), is unsuitable for scoping reviews since the latter method does not appraise a clustered bulk of the evidence analytically. Hence, in scoping reviews, examining sources that encompass the proof is usually not critically appraised since the data are typically from a small number of exploratory studies (Pratt et al., 2019).
Study Selection
Figure 1 displays a flow chart of the studies’ selection process. The initial database search found 125 pertinent studies, with 56 duplicates. Further screening of the remaining 69 studies yielded 25 studies used in the present scoping review after 48 were excluded as they did not relate to care delivery nor African American caregivers. The low number of studies meeting the inclusion criteria is no surprise, as COVID-19 is a new community-spread virus and attracting sociocultural and behavioral health interest only in the past 3 years (or since its official global spread officially documented since December 2019).

2020 PRISMA flow diagram template for systematic reviews (Page et al., 2021).
Data Organization
We organized the data from the reviewed articles by author/s name/s, publication year, study design, target population, and health outcomes (see Table 3). Then, for each study, we considered whether it identifies a gap to be addressed based on the literature.
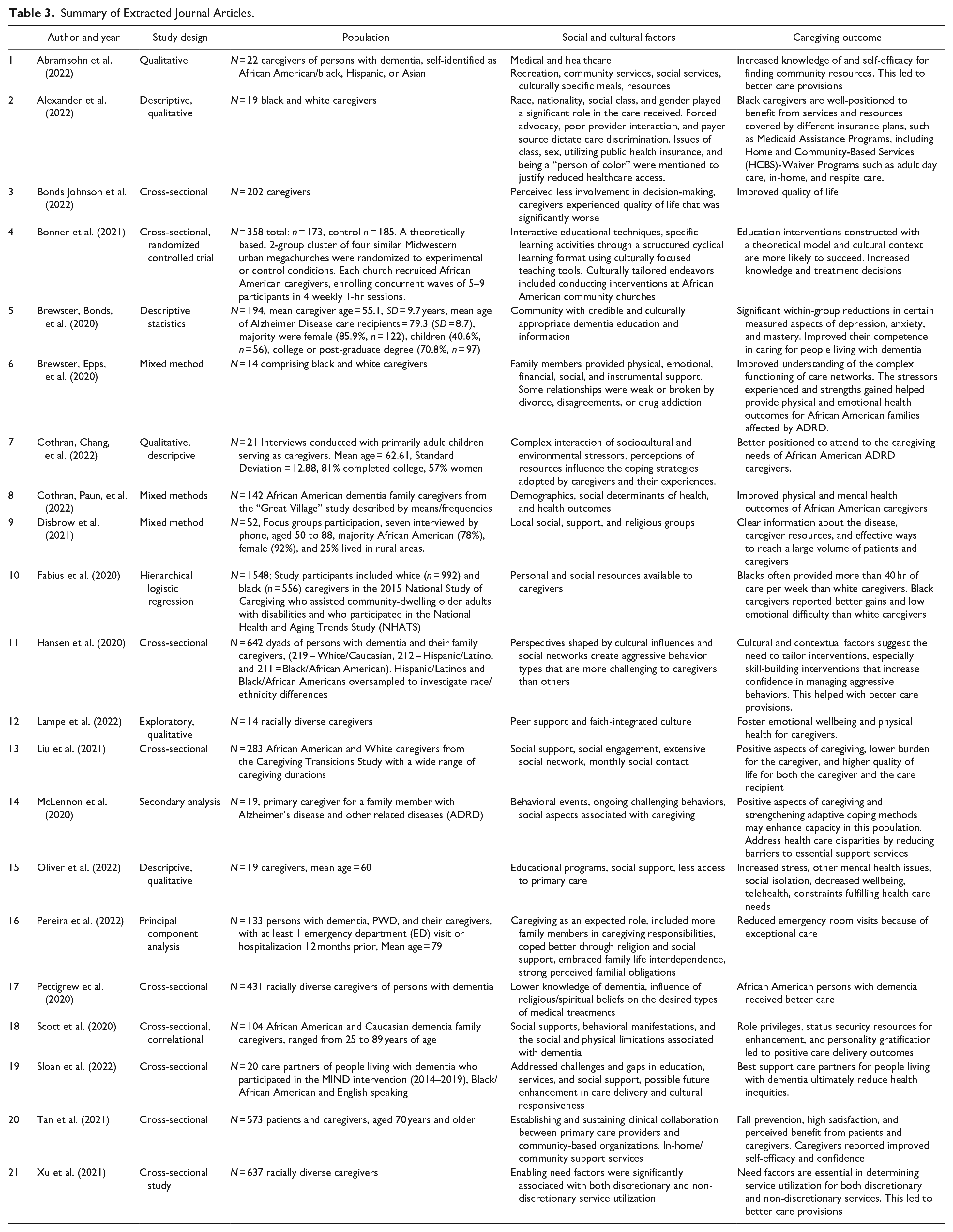
Summary of Extracted Journal Articles.
Results and Discussion
Table 3 presents our findings on the 21 empirical studies included in the present scoping review. By jurisdiction, all reviewed studies were from the United States. A majority of studies reported on the influence of social support and religious groups (peer groups, social groups, community, and environmental groups, social supports, behavioral manifestations, social resources, social supports, behavioral manifestations, social engagement, extensive social network, monthly social contact, social determinants of health, and health outcomes) for older adults during the COVID19 pandemic (Alexander et al., 2022; Disbrow et al., 2021; Fabius et al., 2020; Lampe et al., 2022; Liu et al., 2021; McLennon et al., 2020; Oliver et al., 2022; Pereira et al., 2022; Pettigrew et al., 2020; Scott et al., 2020; Sloan et al., 2022; Tan et al., 2021). Other studies (Abramsohn et al., 2022; Brewster, Bonds, et al., 2020; Brewster, Epps, et al., 2020; Cothran, Chang, et al., 2022; Cothran, Paun, et al., 2022; McLennon et al., 2020; Xu et al., 2021) reported on the influence of cultural factors in care delivery among African American caregivers of persons with dementia, while others discussed the combined effect of both cultural and social factors.
Cultural Factors
Journal articles indicated in Table 3 encompass involvement in decision-making, discretionary service utilization, culturally focused teaching tools, and education interventions. The themes included a theoretical model within a cultural context, with the perception of caregiving as an expected role. In addition, the analysis included the perceived substantial familial obligations, cultural responsiveness, enabling circumstances, and need factors for both discretionary and non-discretionary service utilization, such as culturally specific meals and resources and culturally appropriate Alzheimer’s disease education and information (Abramsohn et al., 2022; Bonds Johnson et al., 2022; Bonner et al., 2021; Brewster, Bonds, et al., 2020; Brewster, Epps, et al., 2020; Hansen et al., 2020; Pereira et al., 2022; Pettigrew et al., 2020; Sloan et al., 2022; Xu et al., 2021). Fewer studies discussed the combined influence of sociocultural factors (Cothran, Chang, et al., 2022; Cothran, Paun, et al., 2022; Lampe et al., 2022; Pereira et al., 2022; Sloan et al., 2022; Xu et al., 2021).
Religion, Spiritual Beliefs, and Faith Integrated Culture
In a study by Pettigrew et al. (2020) using 431 racially diverse caregivers of persons with dementia, African American caregivers had a lower level of knowledge about dementia. They reported a more significant influence of religious/spiritual beliefs on the desired types of medical treatments. In addition, these caregivers had a lower preference for comfort care (81% vs. 58%) and lower rates of completion of legal Advanced care planning (89% vs. 73%) compared to caregivers from other ethnic groups.
Interactive Educational Techniques
In the study by Bonner et al. (2021), with a 2-group, cluster randomized controlled trial, four similar Midwestern urban megachurches were randomized to experimental or control conditions. Each church recruited African American caregivers, enrolling concurrent waves of five to nine participants in four weekly 1-hr sessions (358 total: Action care Plan n = 173, control n = 185). A structured cyclical learning format and culturally focused teaching tools shaped interactive educational techniques and specific learning activities. Education interventions constructed with a theoretical model and within a cultural context were described as more likely to succeed when culturally tailored endeavors included conducting the intervention at African American community churches. This increased knowledge and treatment decisions among African American caregivers of persons with dementia.
A study by Sloan et al. (2022) used 20 care partners of people living with dementia who participated in the MIND intervention (2014–2019). All were Black/African American and English speaking. They addressed fundamental challenges and gaps in dementia education through in-home services and social support, with a possibility of future enhancement in delivery and cultural responsiveness. The outcome was that the support of care partners of people living with dementia could ultimately reduce health inequities.
Discretionary Service Utilization
In their study, Hansen et al. (2020) used a sample of 642 dyads of persons with dementia and their family caregivers (219 = White/Caucasian, 212 = Hispanic/Latino, and 211 = Black/African American), recruited from five U.S. cities (Birmingham, Alabama; Memphis, Tennessee; Miami, Florida; Palo Alto, California; and Philadelphia, Pennsylvania). Both Hispanic/Latinos and Black/African Americans were over-sampled to investigate significant differences by race/ethnicity. Analysis revealed that African American caregivers’ perspectives were shaped by cultural influences and social networks, leading to aggressive behavior types being more challenging to caregivers than others. The application of discretionary service utilization shaped by their culture managed such behaviors. The review suggests that cultural and contextual factors need tailored interventions and discretionary measures especially skill-building interventions that increase confidence in managing aggressive behaviors while decreasing anger incidents and ultimately leading to quality care delivery.
Culturally Specific Meals
A study by Abramsohn et al. (2022) used 22 caregivers of persons with dementia who self-identified as African American/black, Hispanic, or Asian. African American caregivers were more involved in Medical and healthcare recreation, community services, and social services than other ethnic groups. Their actions aided the adoption of culturally specific meals and resources to meet the needs of persons living with dementia. This involvement helped increase their knowledge and self-efficacy in finding community resources for better healthcare delivery.
Responsibility Perception
In a study by Pereira et al. (2022), African American caregivers of persons with dementia perceived caregiving as an expected role. The care involved more family members who embraced interdependence and familial obligations as a priority.
Strong Familial Obligation
Brewster, Bonds, et al. (2020) studied 14 caregivers of persons with dementia. Family members provided physical, emotional, financial, social, and instrumental support. Although some relationships were weak or broken by divorce, disagreements, or drug addiction, there was still a better understanding of the complex functioning of these networks. Despite the stressors and strengths experienced by these networks helped explain physical and emotional health outcomes for African American families affected by ADRD.
McLennon et al. (2020), using a total of N = 19 primary caregivers, stated that persons with dementia showed signs of associated acute behavioral issues and challenging behaviors. African American caregivers were seen to apply positive aspects of caregiving and strengthen adopting coping methods. They concluded that there were also signs of enhanced capacity in this population, addressing health care disparities and reducing barriers to essential support services.
Social Factors
Such factors include social support through religious-based groups, strong peer and community support, and the strong effect of social determinants of health resulting from racial disparities (Abramsohn et al., 2022; Brewster, Bonds, et al., 2020; Brewster, Epps, et al., 2020; Disbrow et al., 2021; Fabius et al., 2020; Lampe et al., 2022; Liu et al., 2021; McLennon et al., 2020; Oliver et al., 2022; Pereira et al., 2022; Pettigrew et al., 2020; Scott et al., 2020; Sloan et al., 2022; Tan et al., 2021).
Social Support and Religious-Based Groups
African American caregivers of persons with dementia utilized social and religious-based support groups for care delivery, thereby achieving quality care delivery to persons with dementia (Abramsohn et al., 2022; Brewster, Bonds, et al., 2020; Brewster, Epps, et al., 2020; Disbrow et al., 2021; Fabius et al., 2020; Lampe et al., 2022; Liu et al., 2021; McLennon et al., 2020; Oliver et al., 2022; Pereira et al., 2022; Pettigrew et al., 2020; Scott et al., 2020; Sloan et al., 2022; Tan et al., 2021). Since the caregivers were predominantly female, they had close social support with other female counterparts. The social support is consistent with other findings by Cohen et al. (2019), where female caregivers provided more personalized caregiving activities, such as bathing, dressing, feeding, shopping, preparing meals and, resource management, compared to men.
Social Services and Networking
Across age cohorts, social services and networking during the COVID-19 pandemic included the utilization of peer groups, maintaining social contact, and the utilization of social resources such as educational and available informational resources (Fabius et al., 2020; Liu et al., 2021; Pettigrew et al., 2020; Scott et al., 2020; Sloan et al., 2022). Fabius et al. (2020) examined the influence of social factors on African American caregivers of persons with dementia for quality care delivery, encompassing a sample of N = 1548. Study participants included white (n = 992) and black (n = 556) respondents to the 2015 National Study of Caregiving who assisted community-dwelling older adults with disabilities who participated in the National Health and Aging Trends Study. The study noted that blacks more often provided more than 40 hr of care per week (54.3% vs. 38.6%) and more often cared for older adults with dementia (27.1% vs. 20.7%) who were living below the federal poverty line (31.7% vs. 11.9%) or Medicaid-eligible (42.2% vs. 11.8%). Black caregivers often used supportive services (32.9% vs. 24.8%). In fully adjusted regression models, black caregivers were more likely to report client behavioral gains and fewer setbacks. Scott et al. (2020) examined the effect of social support and social limitations among caregivers of persons with dementia, totaling 104 African American and Caucasian dementia family caregivers. For this study, caregivers ranged from 25 to 89 years of age, with African American caregivers as the majority. Positive outcomes identified by these authors included role privileges, status security resources for enhancement, and personality gratification with the presence of social support systems.
Additionally, a study by Liu et al. (2021) cited social support, social engagement, an extensive social network, and monthly social contact as influential in care delivery. This study evaluated 283 African American and White caregivers from the Caregiving Transitions Study with a wide range of caregiving durations. It reported positive aspects of caregiving, a lower burden for the caregiver and higher quality of life for both the caregiver and the care recipient.
Strong Peer and Community Support
Lampe et al. (2022) explored the integration of peer support that influenced quality care delivery by African American caregivers of persons with dementia. A peer group with 14 African American caregivers fostered caregiver emotional wellbeing and physical health, leading to quality care delivery by these caregivers. Also, Tan et al. (2021) noted in their study of N = 573 patients aged 70 years and older that peer support helped establish and sustain clinical collaboration between primary care providers and community-based organizations in home-supportive services. In addition, this support helped prevent falls, leading to high satisfaction and perceived benefits from patients and caregivers.
A study of 19 caregivers by Alexander et al. (2022) noted that race, nationality, social class, and gender played a significant role in the care received by persons with dementia. Black dementia caregivers unanimously concurred that the health system they experience in America is “broken.” Gaps in the health system can lead to people [as one caregiver passionately expressed] “falling between the cracks” in terms of care, services, and resources needed. Caregivers agreed that class, sex, access to public health insurance, and being a “person of color” contribute to their difficulties navigating the health system. Despite this, they were still able to offer quality care.
Social Support
In a study by Disbrow et al. (2021), 52 adult caregivers participated in focus groups and seven via telephone interview. Their ages ranged from 50 to 88, with the majority being African American and female (78% and 92% respectively), with 25% living in rural areas. The influence of social, support, and religious groups brought about clear information about the disease, caregiver resources, and the importance of having clinical trials clearly explained and ensuring accessibility by a representative sample of the population. Providing dementia care resources for primary care providers may be an efficient and effective way to reach a large volume of patients and caregivers.
Brewster, Bonds, et al. (2020) conducted a similar study, using 194 caregivers where the mean age was 55.1 (SD = 9.7) years, and the mean age of the dementia care recipients was 79.3 (SD = 8.7). The majority were female (85.9%, n = 122), children (40.6%, n = 56), and 70.8% (n = 97) had a college or post-graduate degree. African American caregivers demonstrated significant within-group reductions in certain measured aspects of depression, anxiety, and mastery, thereby improving their competence to care for people living with dementia.
Social Determinants of Health
Cothran, Chang, et al. (2022) and Cothran, Paun, et al. (2022) evaluated 142 African American dementia family caregivers from the “Great Village” study and described the data using means and frequencies. They posited that demographics, social determinants of health, and health outcomes among African American caregivers influenced stress susceptibility. They asserted that the role of protective factors helps explain inconclusive findings in current caregiver intervention research. African American family caregivers of persons with dementia exhibited improved physical and mental health outcomes, enhancing quality care delivery.
Implications for Gerontological Sociocultural Care Delivery Practices
A good understanding and application of the sociocultural factors influencing quality care delivery among African American caregivers of persons with dementia are essential to implement better care delivery standards. From these findings, the evidence suggests social and cultural factors influenced care delivery by African American caregivers in different domains, notably,
social support
social services and networking
reliance on religious-based groups
networking and social factors among the ethnic groups
peer support and faith-integrated culture,
Social Determinants of Health variations among African American caregivers
Religious and spiritual beliefs
adaptive interactive educational techniques
responsibility perception, and
strong cultural and familial relationships
(Bonner et al., 2021; Brewster, Bonds, et al., 2020; Brewster, Epps, et al., 2020; Disbrow et al., 2021; Pereira et al., 2022; Sloan et al., 2022).
These factors enable caregivers to carry out their duties with great dexterity while delivering quality care to persons with dementia. Engaging in religious activities and building upon strong familial relationships (Pereira et al., 2022; Pettigrew et al., 2020) were regarded as cultural factors that enabled African American caregivers of persons with dementia to deliver quality care. Pettigrew et al. (2020) reported the more significant influence of religious/spiritual beliefs on the desired types of medical treatments. They further noted that African American persons with dementia had a lower preference for comfort care (81% vs. 58%) and lower rates of completion of legal action care planning (89% vs. 73%) compared to caregivers from other ethnic groups. Such observations helped guide their decisions in caregiving, strengthened their relationship with the care recipient, and fostered good responses to care, thereby allowing better outcomes.
Social and cultural factors centered around African American caregivers of persons with dementia likely improved care recipient wellbeing by enhancing adjustment rates and preferences due to the COVID-19 menace. Additionally, Cothran, Paun, et al. (2022) showed that care delivery by African American caregivers was likely to achieve satisfactory outcomes when factoring in demographics, social determinants of health, and health outcomes. Stress susceptibility and coping mechanisms help explain different care delivery mechanics by various ethnic groups. This discrepancy is despite the inconclusive findings recorded in current caregiver intervention research with African American family caregivers. That finding supports recent observations stating that most African American caregivers of persons with dementia are likely to deliver quality care compared to caregivers from other ethnic groups (Kaufman et al., 2010). Several studies reported that compared to other racial groups, African American caregivers recorded a superior quality care level due to their understanding of social and cultural values.
Similarly, Kosberg et al. (2007) indicated that Caucasian caregivers were more likely to be married and older, imbibed acceptance and humor as coping mechanisms, with low rates of financial problems. On the other hand, African American caregivers applied more hours of care, embraced religion and denial as coping styles, and were less stressed. Utilizing the relevant social and cultural factors in caregiving can lead to quality care delivery and optimization of the quality of life (Gallagher-Thompson et al., 2020).
While this scoping review only evaluated social and cultural factors of caregivers of persons with dementia in the United States, similar levels of patient care could very well be applicable in other countries that have similar social profiles of care needs and caregivers. This could be an opportunity for future, broader research.
Limitations of the Review
In summary, we take note of the limitations we have considered in the scoping review. Firstly, we limited the scope to peer-reviewed studies published during the COVID-19 pandemic (December 2019–August 2022). The second is that the 21 studies we surveyed were primarily exploratory, and it is uncertain if the findings would be replicable in follow-up studies. Additionally, we only considered published data based on the United States, so the inferences may not represent global indices. With a more extended timeframe and coverage from more countries, findings may be more comprehensive and globally representative.
Conclusion
Findings from the present scoping review suggest social and cultural factor benefits in quality care delivery by African American caregivers of persons with dementia during the COVID-19 pandemic. Social factors, peer groups, social contacts, and social determinants of health among African American caregivers influence and help them deliver quality care to elderly persons with dementia. In addition, familial relationships, a perceived sense of responsibility, and beliefs in religious affiliations, all representing cultural factors, also help African American caregivers deliver resilient and quality care to older adults. In this exploratory scoping review, we identified that African American caregivers consider their job as a responsibility. This key element could be incorporated in training initiatives for new caregivers to see patients as if they were their own family members.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.