
Abstract
People with dementia are often hospitalized from the emergency department (ED) for “borderline cases,” where outpatient or inpatient management may be clinically reasonable. We sought to investigate how ED physicians make and communicate about decisions in borderline cases. Through cognitive interviews, we asked attending ED physicians from an academic hospital to share their approach to scenarios representing borderline cases with people with dementia and verbalize communication about ED disposition with patients and care partners. We deductively coded responses related to patient/care partner engagement and key features of communication and then elucidated themes related to content and phrasing of communication. Of 21 physicians, two-thirds stated they would offer the option of admission or discharge, but few explicitly communicated admission versus discharge as a choice. Shared decision-making is applicable to these situations and could provide a consistent structure to communication about disposition.
• When emergency physicians involve persons with dementia (PWD) and care partners in disposition decisions, they may not offer clear choices of admission vs. discharge. • Shared decision-making is inconsistently applied in borderline cases, even when intended. • Indirect language (e.g., asking if patients feel “safe” going home) may not signal that a decision is being offered.
• Clinicians should explicitly communicate a need to make a decision about disposition and offer options. • Using structured shared decision-making can better align ED care with patient and caregiver priorities. • Training and tools are needed to support consistent, inclusive communication in emergency settings.What this paper adds
Applications of study findings
Introduction
Over half of people with dementia (PWD) visit the emergency department (ED) annually. PWD are hospitalized from the ED 1.4 times more often than older adults without dementia (LaMantia et al., 2016; Phelan et al., 2012). Up to 40% of PWD who are hospitalized present to the ED for conditions that could be treated in the outpatient setting (Anderson et al., 2020). This poses serious concerns for patient safety: hospitalization is associated with numerous harms in older adults including delirium, falls, and cognitive/functional decline (Liang et al., 2020; Parekh et al., 2020; Pavon et al., 2020; Tabbush et al., 2021). Additionally, each hospitalization costs tens of thousands of dollars; avoidable admissions strain health system resources (Anderson et al., 2020).
Emergency clinicians admit PWD with conditions that could be treated in the outpatient setting based on both clinical and social factors (A. N. Chary et al., 2022; Seidenfeld et al., 2023). Recent qualitative studies have also shown that PWD and care partners feel unheard and desire opportunities to provide input during clinical decision-making in ED and hospital-level care (Chary et al., 2024; Golden et al., 2023). They also show enthusiasm for alternatives to hospitalization, such as hospital at home programs and telemedicine (A. Chary et al., 2024). However, there has been limited research investigating whether and how emergency clinicians engage PWD and care partners in disposition decisions, that is, to discharge or admit from the ED, in clinical scenarios where either outpatient or inpatient management may be reasonable. Such scenarios include, but are not limited to, ambulatory care-sensitive conditions, a list of 28 conditions that can be prevented and/or managed through appropriate primary care (Billings et al., 1993). We refer to these scenarios in the ED as “borderline cases.” In borderline cases, patient and care partner values and goals may help determine the right care setting.
Methods
We performed cognitive interviews with attending emergency physicians to investigate how they approach communication about ED disposition with people with dementia and their care partners in borderline cases. We recruited physicians from an urban academic institution with four affiliated public and private EDs, including a high-volume public level one trauma center and a tertiary care referral hospital with over half of annual ED visits by older adults.
We developed several patient scenarios that were designed to be borderline cases and pilot tested them with three emergency physicians and then refined the cases into three distinct patient scenarios: (1) syncope, (2) congestive heart failure, and (3) pneumonia. Cognitive interviews focused on the physician’s approach to an ED patient with dementia who (1) had one of the three scenarios, that is, a condition that could be reasonably managed in the inpatient our outpatient setting (no vital sign abnormalities) and (2) was accompanied by an in-person care partner. We used a think aloud protocol (Wolcott & Lobczowski, 2021) to ask participants to verbalize their thought process while reviewing clinical data and to simulate communication with the patient and care partner (Supplement A, Interview Guide).
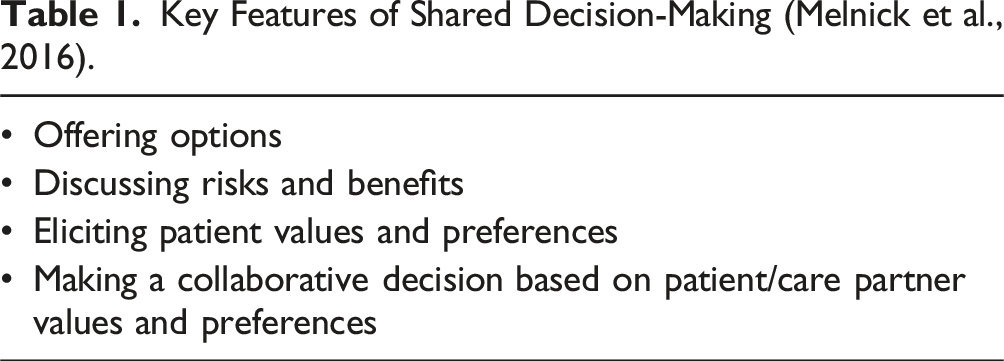
Key Features of Shared Decision-Making (Melnick et al., 2016).
Supplement C provides the Consolidated criteria for Reporting Qualitative research (COREQ) checklist (Tong et al., 2007). The Institutional Review Board of Baylor College of Medicine provided ethical approval (H-53024).
Results
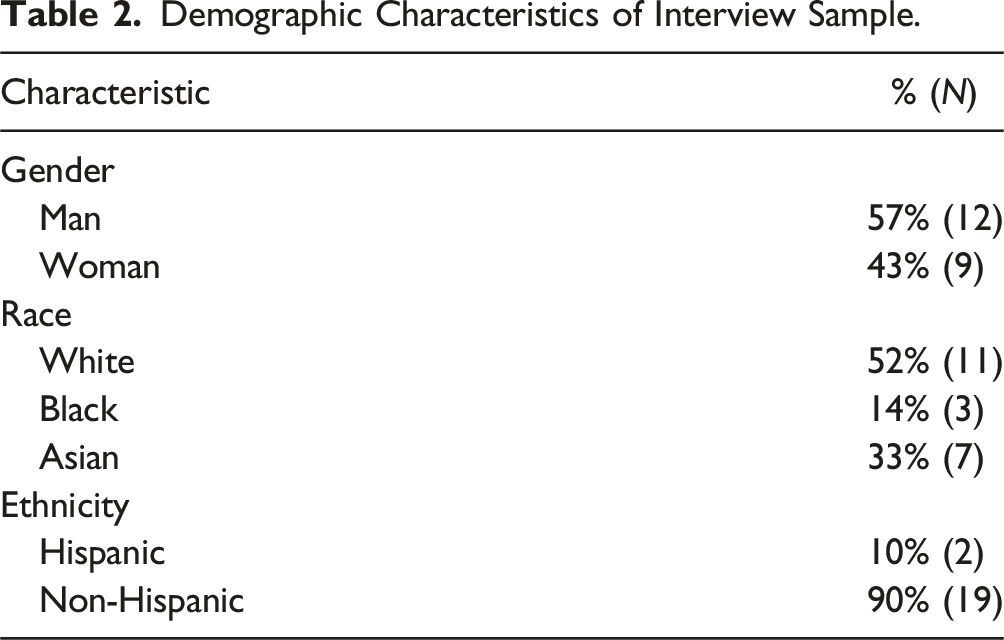
Demographic Characteristics of Interview Sample.
All participants expressed that patients’ conditions could be managed in the inpatient or outpatient setting. Figure 1 summarizes participants’ descriptions of how they would communicate with the patient and care partner about disposition. Most (67%, n = 14) stated they would offer options of admission or discharge. One-third (33%, n = 7) made a recommendation of admission (n = 2) or discharge (n = 5) without offering options or stating they would involve the patient or care partner in the decision. Emergency Physicians’ Approaches to Disposition Decisions for ED Patients with Dementia with Borderline Clinical Cases. SDM: Shared decision-making.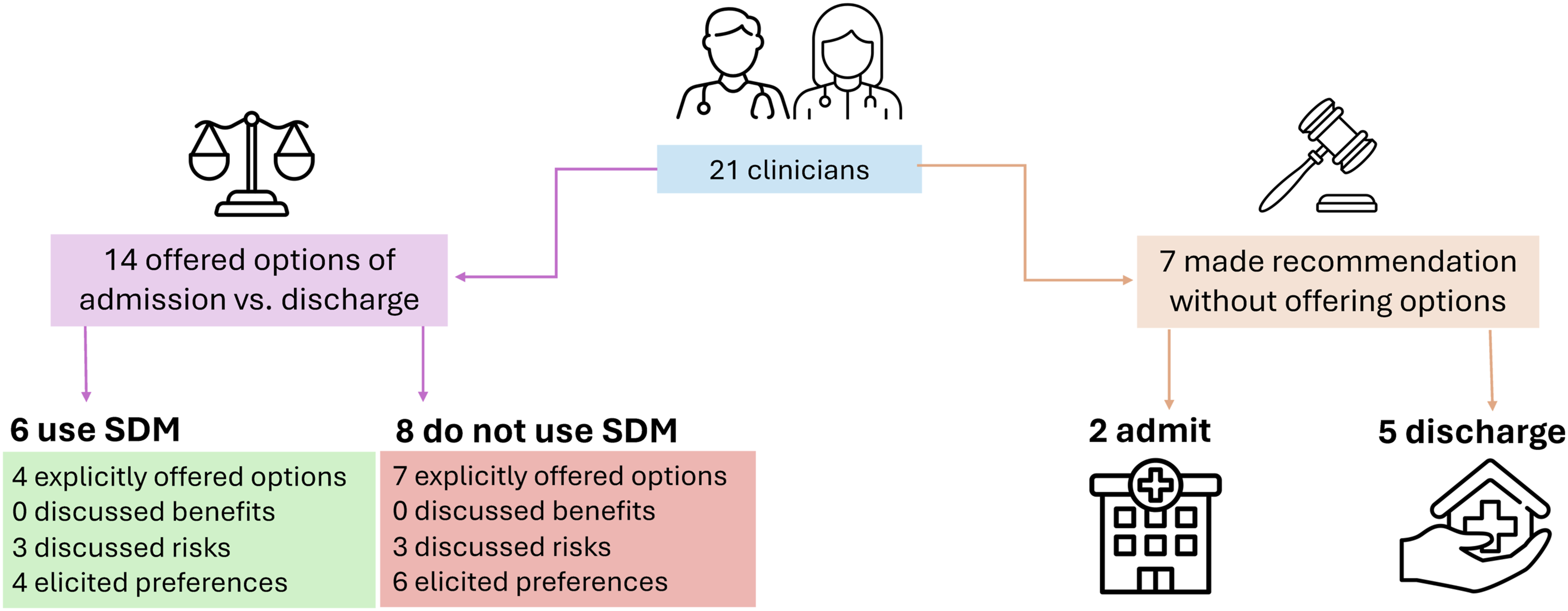
Participants Who Offered Options
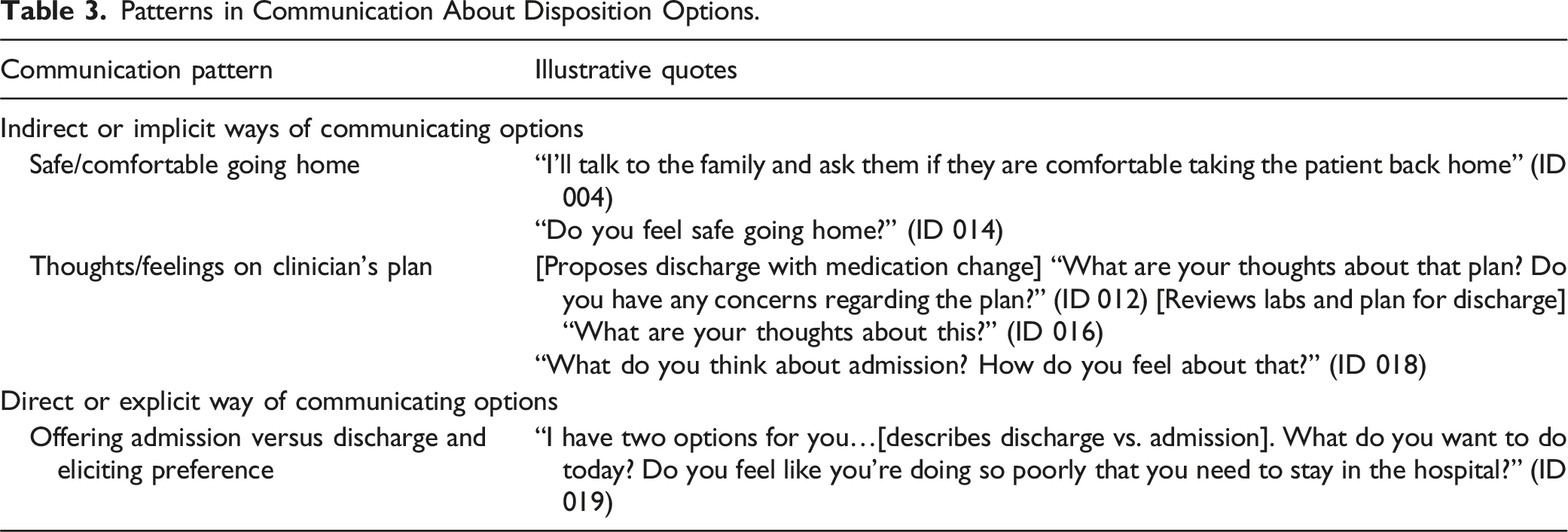
All but four participants who stated they would offer options did so indirectly through language such as, “Do you feel comfortable going home?” rather than explicitly presenting admission versus discharge as a choice. When verbalizing their communication with the patient and care partner, participants presented options in three ways: (1) Asking the patient/care partner if they felt safe or comfortable going home. (2) Presenting a plan for disposition and asking how the patient/care partner felt about it. (3) Offering admission versus discharge and asking what the patient/care partner wanted to do.
Patterns in Communication About Disposition Options.
Among the 14 physicians who stated they would offer options, 6 participants specifically stated that they would use shared decision-making. These 6 participants did not consistently describe performing the core elements of shared decision-making (described in Table 1). Four explicitly verbalized that a disposition decision had to be made and offered two disposition options of admission versus discharge. None discussed benefits of admission versus discharge. Three discussed risks of admission (delirium) versus discharge (clinical decompensation and caregiver burden). Four elicited the patient and care partner’s preference.
Of the 8 participants who offered options but did not discuss shared decision-making, use of elements of shared decision-making was similarly inconsistent. None discussed benefits of admission versus discharge. Three discussed risks of discharge related to clinical decompensation and caregiver strain. Six explicitly elicited patient and care partner preferences.
Participants Who Did Not Offer Options
The 7 participants who did not state they would offer options made recommendations for admission (n = 2) or discharge (n = 5). Those who recommended admission did so due to concerns over diagnostic uncertainty (e.g., syncope) and potential for clinical decompensation (e.g., pneumonia) and discussed associated risks of discharge with the patient and care partner. Otherwise, none discussed benefits of either disposition option, risks of admission, or preferences.
Discussion
In our qualitative study, we found that emergency physicians approached communicating about borderline dispositions with PWD and care partners in varied ways. It was common for physicians to discuss admission versus discharge without directly informing patients or care partners that a decision had to be made, rather than explicitly offering a choice and options. Those who reported they would use shared decision-making tended to clearly verbalize options of admission versus discharge but did not consistently describe using other key elements of discussing benefits, risks, and preferences.
The majority of participants attempted to involve the PWD and care partner in the disposition decision for a borderline case. However, the language they commonly used—questions about comfort returning home or thoughts about a plan—might not indicate to a patient or care partner that there is a choice to be made. Prior research has demonstrated that older adults in the ED and care partners of PWD do not feel engaged in clinical decisions, specifically about hospital admission (A. N. Chary et al., 2024). Our study suggests that ED clinicians may perceive that they are involving patients and care partners, even if patients and care partners do not feel the same way. Importantly, a multi-site survey with ED patients found that the majority want to be engaged in clinical decisions, but more than half did not feel comfortable spontaneously providing input into a clinical decision unless their physicians explicitly asked them about it (Schoenfeld et al., 2018). Taken together, these studies indicate that emergency clinicians should directly ask patients and care partners to be involved in disposition decisions, when appropriate.
Shared decision-making offers a communicative framework for explicitly engaging patients and care partners in clinical decisions (Melnick et al., 2016). It involves a clinician acknowledging a decision needs to be made and offering options, discussing the pros and cons of each option, eliciting patient preferences and values, and making a collaborative decision based on the patient’s values and individual circumstances. A concrete statement such as “we have a decision to make” can be a helpful cue to patients and care partners that they are being involved in a clinical decision and offered a choice. Furthermore, the concept of feeling “safe” going home from the ED may have different meanings to patients and care partners than they do to clinicians. ED clinicians’ disposition decisions are nuanced and involve an assessment of a patient’s mobility, ability to self-care, caregiving resources, and connections to outpatient care (Kilaru et al., 2023). Patients’ and care partners’ prior experiences of common harms of hospitalization—such as delirium and falls—may shape their understandings of home versus hospital safety (A. N. Chary et al., 2024). Explicitly discussing these factors as they relate to risks and benefits of admission versus discharge, per the shared decision-making framework, may promote a shared understanding of patient safety between patients, care partners, and clinicians. Supplement D provides potential discussion points.
A substantial minority of our participants recommended a specific disposition in the borderline case, even though they appreciated that inpatient or outpatient management could be clinically reasonable. This study did not directly ask participants about barriers to engaging PWD and care partners in disposition decisions. Other literature has demonstrated that medicolegal concerns, time constraints, and perceptions of limited patient comprehension keep ED physicians from engaging patients and care partners in clinical decisions (Schoenfeld et al., 2019). For PWD, clinicians may also have challenges determining if the patient has capacity and/or reaching care partners who are not at bedside (A. N. Chary et al., 2022), representing additional barriers to engaging patients in disposition decisions.
Limitations
Our findings are based on a think aloud exercise that occurred outside of physicians’ natural practice environment in the ED. We offer physicians’ perceptions of how they communicate with PWD and care partners, rather than objective observations. We did not include advanced practice clinicians, whose approaches to disposition should also be studied. This study occurred at a single academic site whose affiliated EDs’ practice characteristics differ from other settings but nonetheless represent a starting point in understanding communication with PWD/care partners about disposition.
Conclusion
PWD who present to the ED often have borderline cases in which outpatient or inpatient management is clinically reasonable. Shared decision-making offers a structured framework to address what matters most to patients and care partners by explicitly identifying patient/care partner preferences and priorities as well as potential lack of alignment of care with those priorities. Shared decision-making in borderline cases must be explicit, guided, and participatory. Interventions to promote shared decision-making with this patient population will likely need to provide clinician training to facilitate consistent use of its key elements—and specifically, explicitly acknowledging the decision to be made—while also addressing known barriers ED clinicians face to using this communication technique.
Supplemental Material
Supplemental Material - Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases
Supplemental Material for Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases by Anita N. Chary, Annika R. Bhananker, Rebecca Franks, Adrian Haimovich, Aanand D. Naik, Maura Kennedy, and Kei Ouchi in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases
Supplemental Material for Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases by Anita N. Chary, Annika R. Bhananker, Rebecca Franks, Adrian Haimovich, Aanand D. Naik, Maura Kennedy, and Kei Ouchi in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases
Supplemental Material for Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases by Anita N. Chary, Annika R. Bhananker, Rebecca Franks, Adrian Haimovich, Aanand D. Naik, Maura Kennedy, and Kei Ouchi in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases
Supplemental Material for Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases by Anita N. Chary, Annika R. Bhananker, Rebecca Franks, Adrian Haimovich, Aanand D. Naik, Maura Kennedy, and Kei Ouchi in Journal of Applied Gerontology
Supplemental Material
Supplemental Material - Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases
Supplemental Material for Cognitive Interviews With Emergency Physicians to Understand Disposition Decisions With People With Dementia With Borderline Cases by Anita N. Chary, Annika R. Bhananker, Rebecca Franks, Adrian Haimovich, Aanand D. Naik, Maura Kennedy, and Kei Ouchi in Journal of Applied Gerontology
Footnotes
Acknowledgments
Victoria Sofia Martell.
Author Contributions
Conceptualization: Anita N. Chary, Aanand D. Naik, Maura Kennedy, and Kei Ouchi. Methodology: Anita N. Chary, Annika R. Bhananker, Aanand D. Naik, Maura Kennedy, and Kei Ouchi. Investigation: Anita N. Chary and Annika R. Bhananker. Analysis: All authors. Resources: Anita N. Chary. Data curation: Anita N. Chary. Writing—Original draft: Anita N. Chary. Writing—Review and editing: All authors. Visualization: All authors. Supervision: Anita N. Chary. Project administration: Anita N. Chary and Annika R. Bhananker. Funding acquisition: Anita N. Chary, Maura Kennedy, and Kei Ouchi.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Institute on Aging (R33AG069822), Geriatric Emergency care Applied Research Network 2.0-Advancing Dementia Care, Emergency Medicine Foundation, and West Health Institute. Anita N. Chary receives support from the National Institute on Aging (R03AG078943). Anita N. Chary, Annika R. Bhananker, and Aanand D. Naik receive support from the Houston Veterans Administration Health Services Research and Development Center for Innovations in Quality, Effectiveness, and Safety (CIN13-413).
Sponsor’s Roles
The sponsor had no role in the design, methods, subject recruitment, data collection, analysis, or preparation of the paper.
Ethical Statement
Data Availability Statement
Study data are not publicly available to protect the confidentiality of participants. De-identified coded data may be available from the corresponding author on reasonable request, subject to ethical and institutional guidelines.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.