
Abstract
Introduction
Aged care homes play an integral part in the way society provides care for older people (those aged 65 years and older) who require a level of clinical or self-care which they or their caregivers are unable to provide (Sanford et al., 2015). Facilities where older people receive care are known by several differing names, including nursing homes, care homes, long term care, residential aged care facilities and aged care homes (Benczes & Burridge, 2015; Sanford et al., 2015). The latter term (aged care homes) will be used throughout this paper as it is commonly used in Australia, where the study was conducted.
Internationally, systems for providing services for older people vary greatly and can range from government-funded systems to wholly privatized user-pays facilities (Dyer et al., 2019). The degree of medical, nursing, and allied support services offered by systems can also vary (Armijo-Olivo et al., 2020; Barker et al., 2018; Brett et al., 2019; Scannapieco et al., 2017). The adverse events, however, facing residents and aged care systems, such as injuries, social isolation and complex care needs may be similar despite the localized differences in aged care systems. There is an increasingly complex needs profile of residents entering aged care homes that is common across many countries (Barker et al., 2021; Borotkanics et al., 2017). Worldwide, a high proportion of aged care residents use multiple medications daily, (Pont et al., 2018) have cognitive decline (Dyer et al., 2018) and have difficulty communicating their needs (Cameron et al., 2020). Residents in aged care homes are also particularly vulnerable to the consequences of physical injury, poor mental health, and social/relationship disruptions (Barbosa Neves et al., 2019; Berry et al., 2016; Cresswell et al., 2007; Doupe et al., 2011; Shi et al., 2020). Even a minor incident may cause physical harm and even death (Bergeron et al., 2006). However, not all adverse incidents have a physical effect. There can also be significant social and interpersonal challenges which affect older people once they enter the aged care home such as loss of independence (Walker & Paliadelis, 2016), loneliness (Gardiner et al., 2020), and resident-to-resident aggression (Joyce, 2020). Outside factors such as the built environment (Carver et al., 2020) and climatic changes (McInnes & Ibrahim, 2013) can also have an adverse effect on older people.
Adverse Events or Adverse Incidents?
The term “adverse event” is a term widely used in healthcare yet employed differently across other care settings. Definitions developed in clinical settings focus on a measurable event or error which, by the provision of healthcare services, caused harm to the person receiving the healthcare service (Runciman et al., 2009; Thomas & Petersen, 2003). When applying the term to aged care settings this definition may not always adequately cover the breadth and range of “adverse” triggers which create harm. The terminology used throughout this paper is “adverse incidents.” The definition for adverse incidents used within this scoping review is: any event (single or multiple), episode or factor that contributes to physical, social, or psychological harm (these may be permanent or non-permanent) which adversely impacts on a resident living in an aged care home. Our definition combines clinical definitions (Runciman et al., 2009) along with social and environmental factors (Brownie & Nancarrow, 2013; Toit et al., 2021).
Adverse Incidents in Aged Care Homes
Adverse incidents are well studied within acute care settings (Brady et al., 2009; Kellogg & Havens, 2003) however less so within aged care homes. The aged care home environment is complex. These facilities combine health care and social care and are also the residential home for the older person. The approach to adverse incidents thus requires service providers to balance controlling risks versus affording residents the right to take reasonable risks in their home environment (dignity of risk) (Ibrahim & Davis, 2013).
The effects of adverse incidents in aged care homes have flow-on effects to other areas of the health care system. Hospitalizations due to adverse incidents among people living in aged care homes are a major contributor to the burden on the acute sector (Hillen et al., 2011; Leutgeb et al., 2019; Russell et al., 2015). Yet many adverse incidents occurring in aged care homes are preventable (Hibbert et al., 2021). Using adverse incident information to identify the types of incidents which occur in aged care homes and the context of the aged care home environment can provide useful insights into the challenges, safety, and environment of aged care homes (Simmons et al., 2016). A greater understanding of the ways physical, social, and environmental factors intersect and impact on older people is required to prevent adverse incidents while upholding residents’ rights to choose how they live their lives.
Objectives
This study seeks to undertake a broad examination of the peer-reviewed research that has been undertaken on adverse events or incidents within aged care homes. The aim is to describe what is known about the types of adverse incident research conducted within aged care homes and define the gaps within the literature to inform and strengthen future research directions within this area.
Methods
This scoping review followed the PRISMA Extension for Scoping Reviews (PRIMA-ScR) Checklist (Tricco et al., 2018) and JBI Manual for Evidence Synthesis (Peters et al., 2020). A scoping review was utilized to bring rigor to the research interrogation while allowing for broader investigation of the topic (Munn et al., 2018). The review was undertaken through the lens that good health is determined by the interplay of a range of biological, behavioral, sociocultural, economic and ecological determinants (AIHW, 2014). This scoping review, therefore, seeks to understand how this broader conceptualization of health has been captured in adverse event research in aged care.
Eligibility Criteria
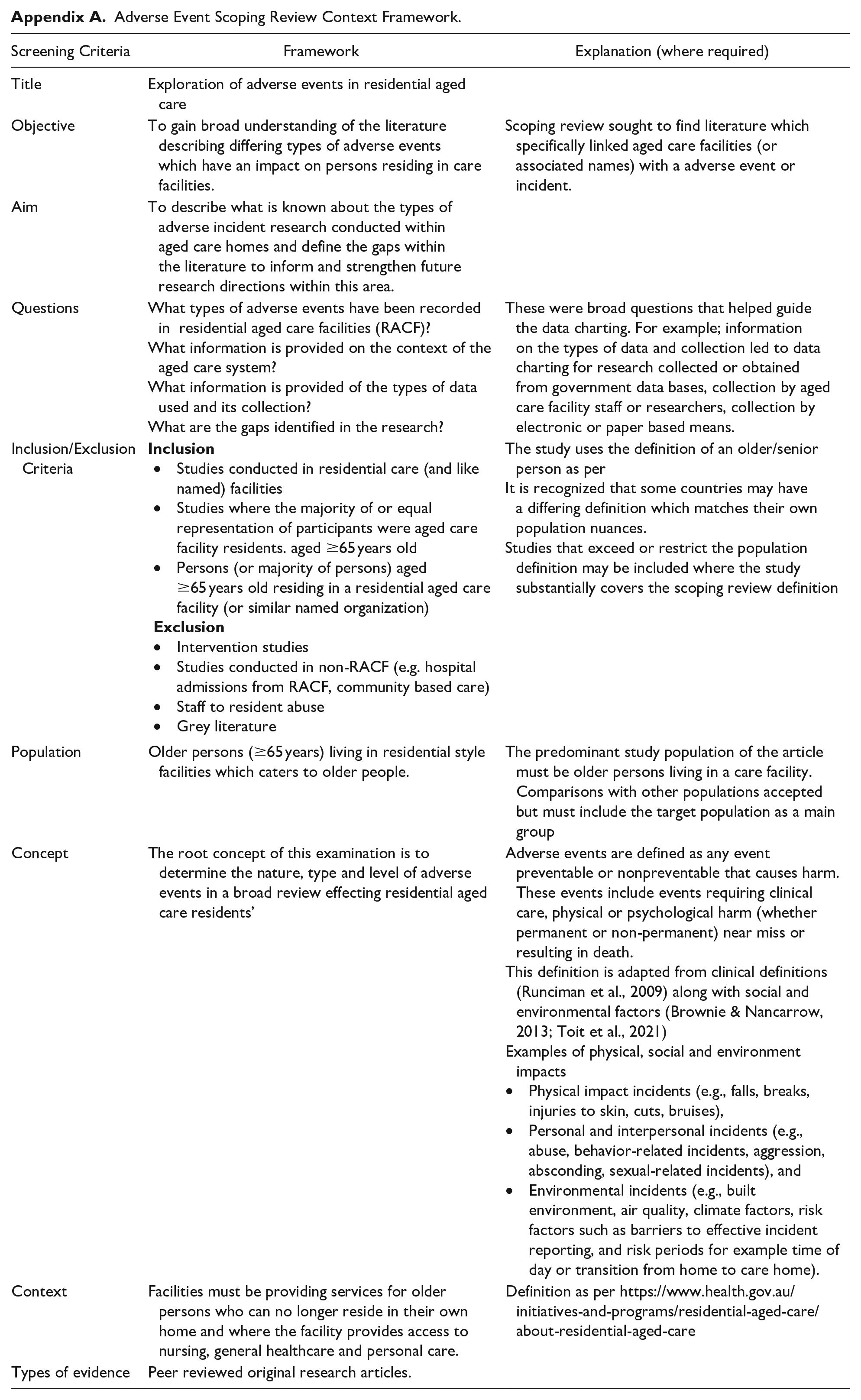
To be included in the review, papers needed to examine adverse incidents or impacts on residents that occurred within an aged care facility. The definition of adverse incidents, described earlier, is broad and draws from the traditional medical model while including a social-ecological perspective (Bornstein & Davis, 2014). This review includes peer-reviewed articles of original research written in the English language, which describe and/or measure the adverse impact and were published between 2000 and 2020. Both quantitative and qualitative articles were included. Articles were excluded if they were not aligned with the scoping review concept framework developed for this review and not peer-reviewed (Appendix A).
Information Sources
The following databases were searched: MEDLINE, CINAHL, and EBSCOhost. Initial searches were conducted in 2018 and updated in 2020 to include articles published to the end of 2020. The database search was augmented by hand searches in the following high impact gerontology journals: Age and Aging, BMC Geriatrics and Ageing, and Society. All editions between 2000 and 2020 were searched using the in-journal search function with combinations of the keywords listed in the search strategy section below. All articles included in the scoping review were peer-reviewed. All searches were conducted by a single researcher (BSC).
Search Strategy
The search strategy used keywords of “aged care” or “nursing home” or “residential aged care facility” or “Homes for the Aged” or “Long Term Care” coupled with either “Incident$”, “adverse event$”, “adverse outcome$”. Additional searches were conducted using keywords based on types of adverse incidents that are the most commonly reported in Australian aged care homes (e.g., falls) (St Clair et al., 2021).
Selection of Sources of Evidence
The search inclusions and exclusions were agreed by all authors. A single author (BSC) was responsible for the selection of evidence based on the search results and comparison against the inclusion/exclusion criteria. The results of searches were exported into EndNote where duplicates were removed. All articles were examined against the Adverse Event Scoping Review Context Framework (Appendix A) and those meeting the inclusion criteria were charted for analysis.
Articles examining interventions were not considered as there are existing systematic reviews examining these associations (Ali et al., 2021; Francis-Coad et al., 2018).
Data Charting Process
Data charting was conducted using an Excel spreadsheet. The data charting form was discussed regularly among co-authors during the data charting process. The items included in the form were allowed to evolve as part of the refining process. Co-author discussions were also used to ensure the project stayed aligned to the overall objectives and questions that this review aimed to address.
Data Chart Items
All articles were charted for year of publication, country where the study was conducted, type of methodology used (i.e., qualitative, quantitative, or mixed methods), data source (retrospective data, real time data), and study population (e.g., high care/low care, inclusion of residents with dementia, age range, gender mix, number of participants).
Adverse incidents were categorized into three domains depending on the area of health impacted. These were physical impact incidents (e.g., falls, breaks, injuries to skin, cuts, bruises), personal and interpersonal incidents (e.g., abuse, behavior-related incidents, aggression, absconding, sexual-related incidents), and environmental incidents (e.g., built environment, air quality, climate factors, risk factors such as barriers to effective incident reporting, and risk periods for example, time of day or transition from home to care home).
Further charting was conducted to evaluate the papers for the level of contextual information provided on the aged care system in which the study was conducted. Articles were evaluated for information relating to whether the data were government held or generated through research, data capture method (electronic or paper and researcher or care worker), ownership of homes being studied (e.g., government funded, for profit and not-for-profit) and whether the population used in the study was a representative sample of the demographics of the country’s aged care home population. Descriptions of the aged care system included in the article were evaluated against a three-point scale (1. articles containing details of the country’s aged care system which were sufficient for the reader to understand the system in which the study took place; 2. articles which provided some limited details about the aged care system; and 3. articles which did not provide details of the aged care system).
Synthesis of Results
Descriptive statistics were used to synthesize the data chart items described above. A summary of the charted items can be found in Table 1 (Study population characteristics and health domains) and Table 2 (aged care system context and data capture methods).
Study Population Characteristics and Health Domains of Included Adverse Incident Studies.
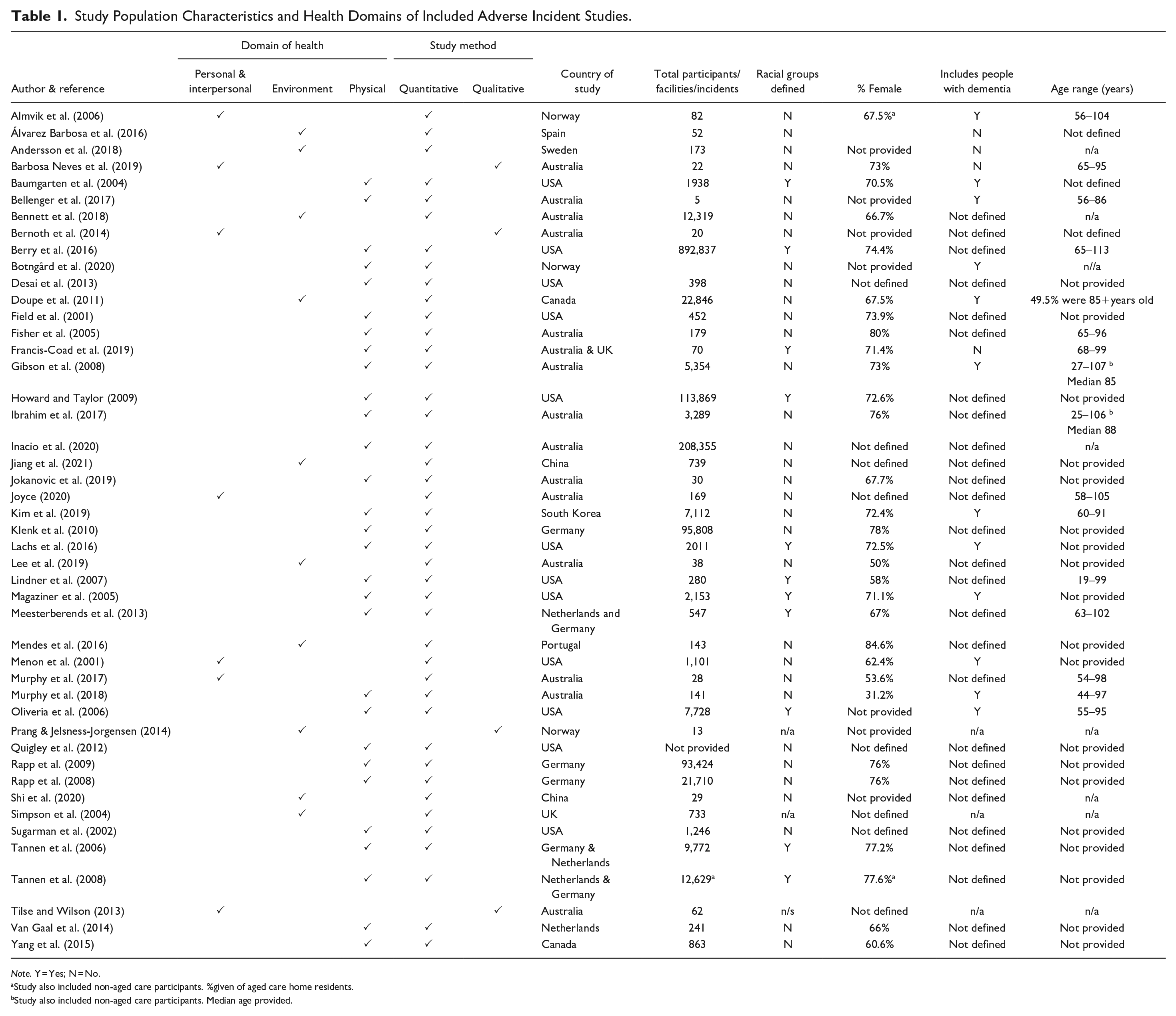
Note. Y = Yes; N = No.
Study also included non-aged care participants. %given of aged care home residents.
Study also included non-aged care participants. Median age provided.
Aged Care System Context and Data Capture Methods.

Results
Selection of Sources of Evidence
The combined searches yielded 3,051 articles (Figure 1). Duplicates were removed (n = 5) and those not meeting the eligibility criteria (Appendix A), 2,970 articles were excluded. Descriptive characteristics (title, journal, date of publication, aim, adverse event) of abstracts for 76 papers were charted prior to further exclusion. This allowed for preliminary thematic analysis for the development of the categories for further data charting.

Scoping review exclusions chart.
Full text versions for articles were sourced. Full text versions for five articles could not be sourced and were excluded from further charting.
The time-period for the review was narrowed to a 21-year range (2000–2020) in line with the research question. Thirteen articles were removed as they fell outside this data range. Five articles were excluded as they were conducted in a setting outside of a care home or with a non-permanent resident cohort (one acute care, two community-based care and two respite care). A further two studies were excluded as they were outside the aims of the review (one on a clinical issue and one on a lifestyle issue). For the purposes of this study, reviews were also excluded (n = 7), leaving 46 articles included in the analysis (Table 1).
Characteristics of the Sources of Evidence
Methodologies used in the studies
Table 1 provides a synopsis of the data charted for the included studies. Of the 46 papers examined, 91% were quantitative (n = 42) and 9% were qualitative (n = 4). Qualitative articles used free text response surveys, interviews and a case study combined with thematic analysis. Quantitative articles were all based on retrospective analysis of data extracted from management information systems or government held data sources.
Study participants
Articles reporting study participants (n = 40, 87%) all included mixed binary (female/male) gendered participants (Table 1). There were no studies focusing on a single gender exclusively or including non-binary gender classifications.
The majority of studies conducted in the United States of America (USA) (Table 1) defined the racial demographics of people in the study population. Within the non-USA articles, racial demographic information was only reported in articles with a study population drawn from two or more countries (n = 4). Racial demographic information was not reported in any of the studies conducted in Europe, the United Kingdom, Asia, or Oceania.
Participants with dementia were included in 11 of the studies (Table 1, 24%), with one study (Kim et al., 2019) specifically examining adverse events for aged care home residents with dementia. Two studies excluded residents with dementia. Twenty-nine (63%) articles did not include information about the cognitive status of participants.
Aged care homes in rural areas were reported on in 17% of studies (Table 2, n = 8). Aged care homes located in urban areas were the focus in nine (20%) of the articles included in this review. Sixty-one percent (n = 28) did not define the locality of aged care homes or residents.
Domains of health
The majority of studies (n = 29, 63%) focused on incidents which impacted on participants’ physical health (Table 1). Fifteen percent (n = 7) of the papers related to social and interpersonal issues, and 10 articles (22%) looked at the environmental impacts (such air quality, flooring type, risk factors or safety issues associated with the care home) and the adverse effects of these on residents.
Synthesis of Results
What types of adverse events or adverse effects, occurring in aged care homes, have been recorded within the research?
The types of adverse incidents examined (refer to Table 1) in the retrieved articles were broad however four types of incidents were dominant: deaths (n = 8), falls (n = 6), pressure injuries (n = 5) and fractures (n = 5). These four incident types made up 52% of the retrieved articles. Forms of abuse (n = 7, 15%) including both physical abuse (e.g., aggression, resident-to-resident) and psycho-social abuse (e.g., forms of elder abuse and financial abuse) were also described. The identification of a sole outcome such as a medication error or fall was described in 34 articles (74%).
Less common were articles which included a contributing factor or causes of an outcome (26%, n = 12). Of these articles five (11%) described the interplay of impacts based on a combination of adverse incidents. Bennett et al. (2018) described rates of infection and how antimicrobial prescribing can influence this outcome. Klenk et al. (2010) described the interplay of environmental factors and adverse impacts through their study of heat-related death, demonstrating that high ambient maximum temperatures increased mortality.
A further four articles examined risk factors such as time of day (Doupe et al., 2011), environmental hazards (Jiang et al., 2021), air quality (Mendes et al., 2016), and flooring. (Simpson et al., 2004) The final two articles (Almvik et al., 2006; Botngård et al., 2020) describe the role of aggression contributing to incidents.
Country of origin and aged care system context
Articles were critically evaluated for the level of information provided about the jurisdictional system in which the aged care facilities operated. All articles provided information of the country where the study was undertaken (Tables 1 and 2). However, specific information about the features of the aged care system in which the study was conducted, such as whether funded privately or by government, was reported in under half of included articles (44%, n = 20). Four articles (9%) provided a detailed description of how the national aged care system worked. Sixteen articles (35%) provided details which described contextual parameters of the aged care system relevant for the reader to be able make comparisons. Thirteen articles (28%) provided information as to whether the study was conducted in a public, private or within both systems.
Six articles (13%) reported how well their study population represented their national aged care home population. Three (7%) were representative of the national aged care cohort of the country the study was conducted in. Two articles (Bennett et al., 2018; Francis-Coad et al., 2019) acknowledged that the sample population was not a representative sample. One article (2%) Yang et al. (2015) reported that their population was a representative cohort for the state in which it was conducted.
Resident and staff inclusion and use of qualitative techniques
A small proportion (n = 5, 11%) of the studies recruited residents as study participants. This included resident-only studies (n = 4) and a study which combined resident and staff views (n = 1)(Menon et al., 2001). No studies included both the resident and their family or other informal caregivers. Francis-Coad et al. (2019) evaluated resident knowledge on falls using a mixed-methods approach, demonstrating that the residents’ perspective of risk and prevention strategies may be out of alignment to the messaging of health prevention programs (Francis-Coad et al., 2019). Staff-only perspectives were used in three of the retrieved articles (Shi et al., 2020; Tilse & Wilson, 2013; Winsvold Prang & Jelsness-Jørgensen, 2014).
Four articles utilized qualitative research techniques to explore the themes of loneliness (Barbosa Neves et al., 2019), elder abuse (Bernoth et al., 2014), incident reporting (Winsvold Prang & Jelsness-Jørgensen, 2014), and financial abuse (Tilse & Wilson, 2013).
Barbosa Neves et al. (2019) used resident interviews and observations to explore how residents understood and perceived loneliness. Their findings indicated that while descriptions of loneliness were consistent across their sample, the coping strategies adopted by residents to deal with loneliness were individualized (Barbosa Neves et al., 2019).
Bernoth et al. (2014) used a case study to highlight the vulnerability of residents to financial abuse and demonstrated residents’ desire to be listened to and heard (Bernoth et al., 2014).
Two articles (Tilse & Wilson, 2013; Winsvold Prang & Jelsness-Jørgensen, 2014) highlighted challenges for staff when faced with adverse incidents in aged care homes. Winsvold Prang and Jelsness-Jørgensen (2014) explored the barriers which prevent staff from reporting adverse incidents. They revealed that organizational culture coupled with individual confidence are important factors in reporting adverse incidents. Tilse and Wilson (2013) undertook scenario testing with aged care staff to evaluate their knowledge and responses to financial abuse of residents. Their findings highlighted the complexity of dealing with situations that have an adverse impact on residents yet fall outside the realm of a physical incident.
Discussion
This scoping review describes the range of adverse incident research within the aged care home environment. We found that while the types of events being examined was broad, the existing evidence has tended to focus on incidents that have a physical impact (such as falls and pressure injuries) rather than social (such as, loneliness and resident-to-resident interactions) and environmental (such as climate or effects of built environment) type incidents. The scoping review also found that information about aged care systems, which can assist in contextualizing and assist in translation of research across countries and jurisdictions, could be strengthened. Inclusion of resident perspectives were also found to be minimal yet can play an important role in understanding what “adversely” impacts aged care residents. The review describes potential gaps and limitations in research that could be used as a roadmap for future research to strengthen our understanding of the impact of adverse incidents on older people in aged care homes.
Learnings
Adverse incidents in aged care is more than physical injuries
Our review has demonstrated that there is a range of incidents and impacts seen in the literature in aged care homes. Yet, adverse incident research still predominately focuses on events with a measurable outcome and specifically a clinical outcome. Interpersonal interactions (such as aggressive behaviors and elder abuse) and the environment could be viewed as having an adverse impact on an older person, yet they are less commonly examined in the literature. Physical impacts, effects of personal and interpersonal relationships, and environmental impacts can all play a role in determining the health and wellbeing of a resident. These areas have been considered to be interconnected within models of health (Davis & Chapa, 2015; Hatala, 2012). While it is important to have detailed research on physical injuries, a focus on clinical outcomes alone misses the nuances of the interplay between social and environment influences on physical health and vice versa (Ostaszkiewicz et al., 2018).
Residential aged care requires a delicate balance between creating a comfortable yet safety-conscious built environment along with appropriate physical and mental health care. Balancing these factors can ensure older people living in these facilities maintain dignity, respect, and quality of life. There is an opportunity for research into adverse incidents in aged care homes to further examine the scope of behavioral, environmental, and sociocultural factors while also considering clinical measures and quality indicators.
Context of the aged care system matters for comparison
We found that information on the context of the aged care system in which the studies took place was varied, and in 56% of studies was not included at all. Research can provide an understanding of an issue and indicate areas to potentially intervene to improve health and wellbeing. For research to be able to be translated into practice or best practice quality indicators, sufficient detail of the context of the study is needed (Nilsen, 2020). More granular information on the specifications of aged care systems, descriptions of source of the data (government versus research) and how the data were collected (by whom, electronic or paper based) would allow for better translation and implementation of research into practice.
International comparisons or benchmarking can be useful for identifying countries with similar systems to increase understanding of what works and areas for improvement in aged care. Quality measurement and indicators currently in use mainly focus on clinical aspects of care (Inacio et al., 2020; O’Reilly et al., 2010) and have often originated from those developed within other areas of the health care system (Jeon et al., 2019). The ability of these systems to capture incidents and impacts on residents within the aged care setting is not well understood (Jeon et al., 2019; Winsvold Prang & Jelsness-Jørgensen, 2014). There remains a need for effective quality of care and quality of life measurements (Cleland et al., 2021; Gilbert et al., 2021; Kane, 2001). Further contextual information in aged care adverse incident research would aid in translating the research findings and providing generalizability of approaches, outcomes, and measurements to enable settings across different countries to learn from each other.
Gaps
Opportunities for qualitative research and inclusion of resident perspectives
This scoping review has highlighted that there are gaps within the body of research that offer opportunities for future aged care adverse incident research. This includes increasing the use of qualitative and mixed methods research techniques to ensure the voice of the residents of aged care homes is heard.
Research has shown that areas of concern for older people differ from the clinical objectives of policy makers and aged care staff (Ludlow et al., 2020). Residents of aged care homes place importance on meaningful social interactions and care that affords dignity to their cultural value system (Cleland et al., 2021; Ludlow et al., 2020). The prioritizing of clinical care and safety goals by facilities or regulations can often override the preferences of residents (Ludlow et al., 2020). It has also been demonstrated that without resident inclusion in the development of programs designed to reduce adverse incidents, the types of questions posed or incentives used, often do not engage residents to participate (Francis-Coad et al., 2019).
Qualitative research adds to research depth through examining the “why” and “how” type questions which flesh out the “what” and “where” aspects of quantitative research (Williams et al., 2019). A balance of both these methodologies helps provide a richer picture of the issue (Everest, 2014). This scoping review found that only 7% of studies on adverse incidents in care homes used a qualitative methodology and only 11% of studies included residents themselves. This presents an opportunity to expand the aged care adverse incident research through the increased use of qualitative and mixed methods techniques and the inclusion of residents’ voice. Combining both aspects can help to create a dignified yet safety-conscious environment within care homes that addresses the issues that are important to residents and their families.
Challenges
Inclusion of high-risk populations
Expanding the range of research to include the resident perspective of adverse incidents provides another challenge, namely the ability to include people with high care needs such as those with dementia and those unable to communicate verbally. This type of research faces many challenges such as recruitment difficulties, finding effective ways to communicate, gaining consent and the pathways to ethics approval (Lam et al., 2018). Internationally, the prevalence of dementia has been difficult to accurately assess (Prince et al., 2016), however studies from Australia (Harrison et al., 2019) have reported that residents with dementia make up nearly half of all residents in aged care homes. Inclusion of this group is important for ensuring all voices are equally heard. Strategies such as using caregivers as co-participants (Hellström et al., 2007) or inclusion of observational methods (Hubbard et al., 2003) may be important in the engagement of this cohort. Future research to address this challenge may lead to valuable insights and expand the breadth of adverse incident research.
Limitations of the review
This scoping review was intended to provide a descriptive account of the international literature where resident experiences or outcomes were described as “adverse events” or “incidents.” It does not cover the broader range of services available to older people such as care within the home setting, hospital, or other healthcare facilities, or those utilizing a combination of care services. While a broad range of incident types were retrieved, there is a possibility that some evidence was not captured by our search parameters, where articles were not indexed or described as “adverse events” or “incidents.” The intention of the scoping review was to be specific in its search parameters but broad in its outlook so as to identify key issues and directions for the future specific to our research aim.
Conclusions
The scoping review presented here has provided a snapshot of adverse incident literature. This contributes to broader understanding of the types of adverse incidents studied in aged care, along with the context of the current research, and allows for the identification of gaps which can direct the focus for further work. This review shows aged care adverse incident research is growing and an understanding of the contributors and outcomes of events such as falls and medication errors is being advanced. However, there is growing recognition of the role of interpersonal and personal impacts (e.g., aggression and elder abuse) on adverse outcomes on older people in aged care homes. Understanding the broader ways in which older people may be adversely impacted in their lives while living in residential style aged care can assist in developing resident-centric policy approaches that consider the differences between clinical care and the broader care provided by aged care homes.
Aged care policy and adverse incident research needs to expand through the inclusion of a broader definition of what is “adverse” to an older person’s health and well-being. A greater level of specific contextual information within aged care adverse incident research could assist in international comparisons and transferability of research. Importantly, greater inclusion of voices of older people themselves through qualitative and multi-method research would provide a key missing perspective on the concept of “adverse” incidents in aged care homes.
Footnotes
Appendix
Adverse Event Scoping Review Context Framework.
| Screening Criteria | Framework | Explanation (where required) |
|---|---|---|
| Title | Exploration of adverse events in residential aged care | |
| Objective | To gain broad understanding of the literature describing differing types of adverse events which have an impact on persons residing in care facilities. | Scoping review sought to find literature which specifically linked aged care facilities (or associated names) with a adverse event or incident. |
| Aim | To describe what is known about the types of adverse incident research conducted within aged care homes and define the gaps within the literature to inform and strengthen future research directions within this area. | |
| Questions | What types of adverse events have been recorded in residential aged care facilities (RACF)? |
These were broad questions that helped guide the data charting. For example; information on the types of data and collection led to data charting for research collected or obtained from government data bases, collection by aged care facility staff or researchers, collection by electronic or paper based means. |
| Inclusion/Exclusion Criteria | The study uses the definition of an older/senior person as per |
|
| Population | Older persons (≥65 years) living in residential style facilities which caters to older people. | The predominant study population of the article must be older persons living in a care facility. Comparisons with other populations accepted but must include the target population as a main group |
| Concept | The root concept of this examination is to determine the nature, type and level of adverse events in a broad review effecting residential aged care residents’ | Adverse events are defined as any event preventable or nonpreventable that causes harm. These events include events requiring clinical care, physical or psychological harm (whether permanent or non-permanent) near miss or resulting in death. |
| Context | Facilities must be providing services for older persons who can no longer reside in their own home and where the facility provides access to nursing, general healthcare and personal care. | Definition as per https://www.health.gov.au/initiatives-and-programs/residential-aged-care/about-residential-aged-care |
| Types of evidence | Peer reviewed original research articles. |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.