
Abstract
The current study examined if living alone is associated with self-perceptions of aging (SPA). The study used two-wave longitudinal data, sampled from the Health and Retirement Study (HRS), and collected in 2014 and 2018. In total, 6506 older adults aged 60–99 years at baseline were followed up with a 4-year lag. Results indicated that there was no significant change in SPA at follow-up regardless of changes in living arrangements. However, at follow-up, there was a significant cross-sectional difference in SPA between older adults who remained in partnership and those who transitioned to living alone due to widowhood or separation/divorce over a 4-year period. Findings suggest that SPA is relatively stable over time and is barely affected by living alone.
Keywords
Positive attitudes toward or satisfaction with own aging are a unique aspect of aging, as well an important indication of older adults’ potential for psychological resilience and subjective well-being (Beyer et al., 2015; Klusmann et al., 2019; Levy et al., 2002; Robertson et al., 2016; Steverink et al., 2001). The existing literature has shown that older adults’ self-perceptions of aging (SPA) or attitude toward their own aging varies depending on gender and health conditions and tends to change with age (Boeder & Tse, 2021; Diehl et al., 2021; Hausknecht et al., 2020; Kim et al., 2021; Kleinspehn-Ammerlahn et al., 2008; Sargent-Cox et al., 2012). For example, Sargent-Cox et al. (2012) showed that declined capability to perform activities of daily living negatively influenced SPA. Diehl et al. (2021) examined three aspects of SPA (i.e., perceptions of physical losses, social losses, and ongoing development) among older adults in Germany and found that with age, older adults tended to demonstrate more negative perceptions of their physical and social functioning and ongoing development. They further pointed to health variables (e.g., chronic diseases), negative affect and loneliness, and positive affect as strong predictors for change in perceptions of physical losses, perceptions of social losses, and perceptions of ongoing development, respectively. According to Kim et al. (2021), a decline in physical health and spousal strain were significantly associated with a lower level of positive SPA; however, when comparing married men and women, the former were more likely to be affected by spousal strain and chronic conditions, while the latter were more likely to be affected by functional limitations. However, little is known about how living arrangements and transition to different living arrangements due to changes in marital status contribute to older adults’ SPA over time.
As dependency increases with age, maintaining a partnership and living with a spouse or a partner plays a significant role in promoting health and quality of life in older adults (Bolina et al., 2021; Henning-Smith, 2016; Khodabakhsh, 2021; Mazzuco et al., 2017). According to Henning-Smith (2016), older adults who live with a spouse were more likely to report better quality of life compared to those who live alone. Mazzuco et al. (2017), examined the role of living arrangements in the cognitive health of European older adults, and found that, in Sweden, Denmark, Netherlands, and Belgium, those who lived with others (including a partner and/or children) were less likely to report cognitive decline over time. Relatedly, living alone is often considered a risk factor for social isolation, loneliness, depression, and cognitive decline in older adults (Carney et al., 2016; Fingerman et al., 2021; Montayre, et al., 2019; Russell & Taylor, 2009; Stahl et al., 2017). Bolina et al. (2021) showed that older adults who lived alone demonstrated a significantly lower level of quality of life, particularly in the social intimacy domain, compared to those who lived with their spouse. Srivastava and Muhammad (2021) reported that older adults who experienced a transition in living arrangements were more likely to score low on subjective well-being. Psychological distress and limited social support due to changes in marital status and living arrangements might restrain positive attitude toward ones’ own aging.
Yet, there is an opposing view that living alone does not necessarily lead to negative consequences (Evans et al., 2019; Lou & Ng, 2012; Warr et al., 2004; Yigen et al., 2018). For example, according to Evans et al. (2019), even though older adults living alone were more likely to report loneliness and isolation from family, they did not seem to experience a significant decline in cognitive function compared with older adults living with others. Similarly, Lim and Kua (2011) reported that older adults who lived alone were more likely to experience loneliness and depression compared to those who lived with others; however there was no significant difference in the two groups for social, productive, and health-related activities and various health measures (e.g., medical problems, activities of daily living, and cognitive function). Yigen et al. (2018) showed that there was no significant difference between the overall quality of life of Turkish older adults who lived with a spouse and their counterparts who lived alone. Zhou et al. (2018) revealed that compared with living alone, living with a spouse did not make any significant contribution to better health perception but it was rather significantly related to a higher level of activities of daily living disability. That is, older adults living alone might maintain better health, engage more in social and leisure activities outside their home environment, and develop a higher level of resilience and coping skills to compensate for any disadvantage from living alone (e.g., lacking intimate social contact and immediate social support in a household). The existing literature thus calls for more research on various correlates and the consequences of living alone in later life.
Building on this, the current study aimed to examine if there is a significant difference in SPA between older adults living alone and older adults who were living with a partner, and if SPA changes over time based on living arrangements. To more precisely examine the effect of living alone, we also differentiated between the two groups of older adults who lived alone based on their living arrangements at baseline and follow-up. That is, one group included those who lived alone at baseline and also at follow-up (i.e., no change in living arrangements) and the other group included those who lived with a partner at baseline but lived alone at follow-up (i.e., marital status had changed from married to widowed or separated/divorced). Our findings would provide a better understanding of the challenges and opportunities encountered by older adults living alone.
Methods
Study Design and Sample Frame
A two-wave longitudinal study was employed using data sampled from the Health and Retirement Study (HRS). The HRS has collected information about SPA using a self-administered psychosocial and lifestyle questionnaire that allowed respondents to provide subjective evaluations about their lifestyle, social relationships, work, and well-being. As HRS recruits same subsample with a 4-year intervals, the current study used data collected in 2014 and 2018 (i.e., a 4-year gap) with the latter including the most recent data on SPA. The HRS survey data are publicly available (https://hrsonline.isr.umich.edu/) and a detailed description of the main survey design, data collection procedure, and informed consent can be found elsewhere (see Faul & Smith, 2017; Smith et al., 2013). As the current analysis used a publicly available database, the Ethics Committee of the authors’ institutions waived the need for approval.
Of the participants who completed the leave-behind survey questionnaires in both data collections, those aged 60 years and older at baseline were first identified (N = 8753). Then, we examined the living arrangement status of the respondents. Participants were excluded if 1) they were married or partnered but did not live with a spouse/partner, 2) they were not married or partnered but lived with another unrelated adult, 3) they were not married or partnered but lived with a relative (including minor children) or with an unrelated minor child, or 4) their living arrangements were unknown. Those who were living with a partner (married or partnered, N = 5343) or living alone (not married or partnered, N = 2104) at baseline were selected. Accordingly, a total of 7477 respondents were followed-up after a 4-year period.
Of the respondents who were living with a partner at baseline (N = 5343), 82% (N = 4355) had the same living arrangement at follow-up, while 7% (N = 353) reported they were living alone at follow-up. Of the respondents who were living alone at baseline (N = 2104), 85% had the same living arrangement at follow-up (N = 1798). Regardless of the baseline living arrangement, respondents were excluded (N = 941) if their living arrangement at follow-up met either one of those conditions 1) married or partnered but not living with a spouse/partner, 2) not married or partnered but living with another unrelated adult, 3) not married or partnered but living with a relative (including minor children) or an unrelated minor child, or 4) living arrangements unknown (see Figure 1). Accordingly, the final sample consisted of those respondents living with a partner (married or partnered) or living alone at follow-up (N = 6506). Figure 1 shows the process through which the study sample data were selected. Study sample selection. * Cases were excluded if 1) they were married or partnered but did not live with a spouse/partner, 2) they were not married or partnered but lived with another unrelated adult, 3) they were not married or partnered but lived with a relative (including minor children) or with an unrelated minor child, or 4) their living arrangements were unknown.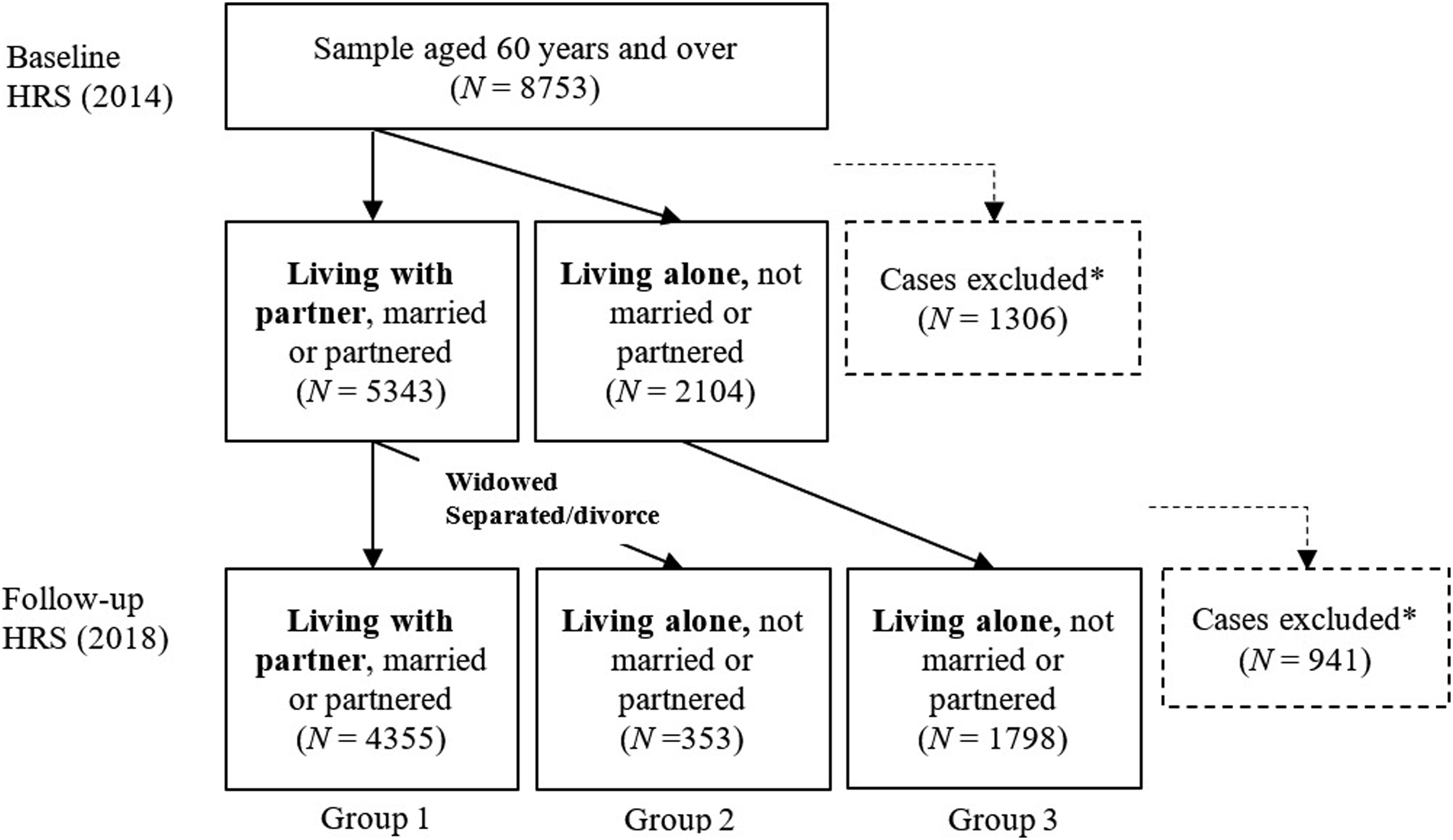
Measurement
A unidimensional construct of SPA was assessed using eight questionnaire items that were derived from the Philadelphia Geriatric Center Morale Scale and the Berlin Aging Study (Kleinspehn-Ammerlahn et al., 2008; Lawton, 1975; Liang & Bollen, 1983). Using a 6-point Likert scale, participants were asked to indicate how much they agreed or disagreed with each given statement; the responses ranged from 1 (strongly disagree) to 6 (strongly agree). A higher score indicated a more positive evaluation of and attitude toward respondents’ experience of aging. The multi-item scale of SPA had satisfactory internal consistency at both baseline and follow-up (Cronbach’s α = .78 and .78, respectively). The items used were as follows: “Things keep getting worse as I get older.” (reverse coded) “I have as much as pep as I did last year.” “The older I get, the more useless I feel.” (reverse coded) “I am as happy now as I was when I was younger.” “As I get older, things are better than I thought they would be.” “So far, I am satisfied with the way that I am aging.” “The older I get, the more I have had to stop doing things that I liked.” (reverse coded) “Getting older has brought with it many things that I do not like.” (reverse coded)
Data Analysis
Descriptive statistics were used to examine demographic structure of the sample. A one-way analysis of covariance (ANCOVA) was used to examine if there was a significant mean difference in SPA at baseline between older adults living with a partner and their counterparts that lived alone while controlling for the potential effect of demographic variables (i.e., gender, age, race/ethnicity, and education) and baseline self-rated health. ANCOVA was also used to compare SPA scores among the three groups at follow-up: Group 1—remained living with a spouse/partner, Group 2—transitioned to living alone, and Group 3—remained living alone. Covariates included demographic variables (i.e., gender, age, race/ethnicity, and education) and baseline measures of SPA and follow-up measure of self-rated health. Levene’s test and normality test were performed to determine if the assumptions for the analyses were met, if the residuals were normally distributed, and if the variances were similar for the groups. With significant ANOVA results, post hoc tests were performed to determine which groups differed (pairwise comparisons). As the three groups had different sample sizes, Scheffe post hoc test was employed. To examine any change in SPA over time based on different living arrangements, paired samples t-test was used for each group. The sampling weights at the individual respondent level were applied to adjust for selective non-responses; the sampling weights were based on birth cohort and 2014 households that were post-stratified to the 2014 American Community Survey (ACS) database. Data preparation and analyses were conducted using IBM SPSS Statistics version 20.
Results
Demographic characteristics of the sample (N = 6506).

aAge is reported as age at follow-up.
bOther included American Indian, Alaskan Native, Asian, Native Hawaiian, and Pacific Islander.
cA separate questionnaire item was used to identify the Hispanic populations. Respondents were asked to indicate either non-Hispanic or a specific type of Hispanic.
Mean difference in SPA at baseline was examined comparing two groups, a sample of Groups 1 and 2 (living with a partner) with a sample of Group 3 (living alone). Levene’s test and normality test satisfied the assumptions of the normality and equal variances. The ANCOVA indicated that there was no significant mean difference in SPA at baseline between older adults who were living with a partner and those who were living alone (M = 4.15, SD = 1.16 to M = 4.03, SD = 1.19) whilst adjusting for age, gender, race/ethnicity, education, and baseline self-rated health.
Mean difference in SPA between baseline and follow-up.

Note. Group 1: married/partnered, living with a partner in 2014 and remained in partnership in 2018 (N = 4355); Group 2: married/partnered, living with partner in 2014 but lived alone in 2018 (N = 353); and Group 3: lived alone in 2014 and remained living alone in 2018 (N = 1798). Self-perceptions of aging used a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree).
To determine time effect on SPA, a paired samples t-test was performed for each group. The results indicated that there was no significant change in the measure of SPA between baseline (M = 4.15, SD = 1.16) and follow-up (M = 4.19, SD = 1.27) among the total sample. There was also no significant difference observed between baseline and follow-up across the three groups: Group 1‐remained living with a spouse/partner (M = 4.19, SD = 1.15 to M = 4.25, SD = 1.27), Group 2‐transitioned to living alone (M = 3.97, SD = 1.19 to M = 3.98, SD = 1.11), and Group 3‐remained living alone (M = 4.03, SD = 1.19 to M = 4.05, SD = 1.28). Table 2 shows the mean difference in SPA over a 4-year follow-up period among the sub-groups.
Discussion
The current study examined whether living arrangements or transitions in living arrangements affected SPA. Our sample data showed that neither older adults living alone nor those who recently transitioned to living alone demonstrated a significant change in SPA over a 4-year follow-up period. This might suggest that SPA is relatively stable over time and is barely affected by the living arrangement status. The results also indicated that there was no significant difference in SPA between participants living alone and those living with a partner both at baseline and follow-up. Warr et al. (2004) found that older British adults living alone demonstrated a similar level of emotional well-being to those of their married or partnered counterparts. According to Zhou et al. (2018), living with a spouse did not have a significantly positive effect on self-rated health and cognitive health compared with living alone when controlling for sociodemographic variables and health behaviors. Klinenberg (2016) pointed to an increased number of older adults living alone in developed countries and argued that living alone should not be considered a synonym of social isolation or loneliness. Our results, together with those of previous studies, suggest that not all older adults living alone are vulnerable or disadvantaged, thus, it might be too early to attach a stigma to living alone in later life or solo aging. Living alone in later life might influence aspects of older adults’ way of living, as it can be significantly correlated with a lack of positive spousal support and family care. However, if older adults receive compensating resources (e.g., support from friends or neighbors or health care services) they might be able to remain independent and active in their given (or chosen) living environment.
At follow-up, a significant cross-sectional difference in SPA was observed between the groups. For older adults who became widowed or separated/divorced and started living alone over the 4-year follow-up period, the level of SPA was significantly lower than that of those who remained married and lived with their partners. However, as there was no significant change in SPA within Group 2 over time, we are cautious to conclude that this statistically significant cross-sectional difference indicates a meaningful difference in change between the groups over time. As data showed, the SPA of older adults who remained living with their partners/spouses slightly increased over the 4-year follow-up period, which could lead to statistically significant group differences. Therefore, our findings might point to benefit of maintaining partnership and living with a partner in later life, rather than negative effects of living alone. Interestingly, at baseline, more than 90% of the sample living alone (Group 3 – remained living alone at follow-up) indicated their marital status as either widowed or separated/divorced. However, there was no significant difference in SPA compared with those who were living with a partner. That is, changes in marital status and living arrangements are not sufficient to explain the cross-sectional difference between groups and no significant difference between baseline and follow-up measures. Future studies should extend these results and employ a long-term observation to more precisely examine how trajectories in marital status and living arrangement play a role in SPA over time, either as a direct antecedent for SPA or rather serve as a moderator between SPA and other substantial predictors.
In addition, significant demographic variations across groups are worth mentioning. For example, compared with those who maintained their partnership, a higher proportion of females was notable in groups where participants were living alone at follow-up. This is consistent with existing literature on demographic trends in aging populations—older women are more likely to be widowed and living alone (e.g., Bolina et al., 2021; Poulain et al., 2020). Thus, preventive healthcare and policy including bereavement care require attention toward gender perspectives. In addition, some older adults who transitioned to living alone because of later-life divorce or separation might experience difficulties with material resources and adaptation to different social roles and environments. The development of policies including psycho-social intervention and re-entry programs for retirees can help alleviate the negative effects of late-life marital transition on positive SPA.
Although the study findings helped improve our understanding of how living arrangements and changes to these in later life are associated with SPA, there remain several questions. To simplify the comparisons between groups, our analysis deemphasized other types of living arrangement, including living with children or relatives. A handful of studies showed that older adults living with others (without spouse) often reported poorer health conditions compared to those living alone (e.g., Henning-Smith, 2016). Also, relatedly, living arrangements in later life may greatly depend on socio-cultural factors. In societies where older adults’ dependency (material and emotional) on kinship (e.g., adult child) is relatively high, they might have less tolerance for living alone. Thus, the meaning of living alone may differ based on personal, physical, and social situations that might further influence SPA. As the current study used a sample of older adults in the United States, living alone (living independently) might be more pervasive, thus, the effect on SPA might be meager. Future studies should better contextualize differences in SPA by considering more information about different behaviors and social expectations/experiences associated with socio-cultural specificities. Furthermore, as a preliminary observation, we used two waves of data collected in 2014 and 2018, which allowed us to focus on the most observable life changes between two time points (i.e., changes in living arrangements) while being less affected by different life trajectories that could happen if a longer period of time was considered. Considering HRS’s recruitment of the same subsampling with 4-year intervals, it would be interesting to access the data from 2010 for those older adults who lived alone between 2014 and 2018 and examine how their living arrangements and marital status changed over time, and if such change was related to changes in SPA across the three time points.
Footnotes
Author Contributions
S. Lee designed the study, performed all statistical analyses, and wrote and revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
SL was funded by The Czech Science Foundation (19-11418Y GAČR). None of the funding bodies had any role in study design, data collection, data analysis, data interpretation, or writing of the report.
Ethics Review
The current study employed publicly available secondary data. The Ethic Committee of the Faculty of Physical Culture, Palacký University Olomouc waived the need for approval.