
Abstract
Objectives
Neighborhood environments influence falls in later life, but the role of functional limitations in this relationship is unclear. Guided by environmental gerontology theories, we examined whether functional limitations (none/mild/severe) moderated the association between neighborhood social cohesion and physical disorder and subsequent falls.
Methods
We pooled adults aged ≥65 (n = 5,075) from the 2014–2016 Health and Retirement Study and assessed falls 2 years later (2016–2018). Survey-weighted logistic regressions estimated associations at each limitation level, adjusting for sociodemographic and health covariates.
Results
Higher social cohesion and physical disorder were associated with greater odds of falls. Among those with mild limitations, both associations were attenuated, while among those with severe limitations, higher physical disorder was associated with lower odds of falls.
Discussion
Findings highlight the need to address both environmental and individual factors in fall prevention and suggest that lower risk among limited adults reflects self-restriction, underscoring supervised indoor exercise and accessible transportation.
Introduction
Falls among older adults represent a major public health concern in the US, impacting one in four individuals aged 65 and older each year and resulting in healthcare costs totaling $50 billion annually (Centers for Disease Control and Prevention, 2024). Falls are also one of the most prevalent issues addressed in emergency care, leading to over three million emergency department visits annually (Kelekar et al., 2021). Fall incidents contribute significantly to injury-related morbidity and mortality among older adults (Montero-Odasso et al., 2022). Beyond immediate physical harm, falls among older adults can also lead to long-term consequences such as loss of independence and decreased quality of life (Kelekar et al., 2021; Montero-Odasso et al., 2022). Reducing falls and fall-related negative outcomes among older adults is, therefore, a US national priority (American Public Health Association [APHA], 2024).
Functional limitations are a critical determinant of falls among older adults, reflecting declining physical functioning through difficulties in performing essential self-care tasks and managing household responsibilities (Das Gupta et al., 2025). Indicators of functional independence in later life often include activities of daily living (ADL; e.g., bathing, dressing, eating, toileting), instrumental activities of daily living (IADL; e.g., meal preparation, managing medications, transportation, housework), and constraints in physical abilities related to mobility and strength (e.g., difficulties in walking, climbing stairs, carrying heavy objects) (Das Gupta et al., 2025). Much of the literature on falls focuses on individual factors, including functional limitations (Schiltz et al., 2020), as well as other personal health factors such as impaired eyesight, hearing loss, chronic diseases, cognitive impairment, and muscle loss (Liu et al., 2024).
However, the role of environmental influences in late-life physical functioning has been central to theoretical models in environmental gerontology (Clemson et al., 2023). In synergy, empirical studies utilizing environmental gerontology theories to investigate neighborhood factors, such as social cohesion and physical environment, have demonstrated that adverse neighborhood characteristics can contribute to increased fall risk among older adults. For instance, neighborhood social cohesion has been found to have protective effects on fall risk by providing social support and fostering a sense of community, which may encourage help-seeking behaviors and access to resources (Clemson et al., 2023; Nicklett et al., 2017). Conversely, neighborhood physical disorder has been identified as a key determinant that increases fall risk by negatively affecting mobility, engagement in physical activity, and perceived safety (Lee & Lim, 2023; Nicklett et al., 2017).
Despite the significance of the above findings, a particular limitation of the research examining the link between perceived neighborhood environments and falls is its focus primarily on direct associations, often overlooking potential effect modifiers like functional limitations. Consequently, the extent to which exposure to adverse neighborhood environmental conditions contributes to falls among older adults in the presence of functional limitations has not yet been thoroughly examined in the existing research. Additionally, studies examining neighborhood factors tend to focus on either physical characteristics or social cohesion (Clarke et al., 2023; Kim et al., 2020), often neglecting the joint influence of these dimensions on fall risk. Considering both factors simultaneously could be salient, leading to a more comprehensive understanding regarding the influence of neighborhood environment on subsequent falls of older adults.
To address the above gaps, we draw upon the Collective Efficacy Theory and the Competence-Press Model to examine the moderating role of functional limitations in the relationship between perceived neighborhood environments and falls among older adults. The Collective Efficacy Theory (Sampson et al., 1997) and the Competence-Press Model (Lawton & Nahemow, 1973) suggest that older adults’ ability to maintain functional independence and prevent falls is influenced by both the physical and social attributes of their residential environments. More specifically, the Competence-Press Model suggests that in environments with excessive “press” or high environmental demands, individuals with lower competence, such as those with functional limitations, will experience the highest risk of adverse outcomes, including falls (Freedman et al., 2017). On the other hand, the Collective Efficacy Theory (Sampson et al., 1997) extends beyond physical conditions to emphasize the role of social processes in shaping environmental risks and protective factors for falls. It suggests that strong social cohesion and informal social control within a neighborhood can create safer environments, reducing exposure to hazards that contribute to falls (Hipp, 2016). Older adults with functional limitations may particularly benefit from higher collective efficacy, as supportive neighbors can assist with mobility challenges, reducing fear of falling and encouraging engagement in outdoor activities (Galinsky et al., 2012).
Therefore, in this study we address the following research questions: (1) when considered simultaneously, how does perceived neighborhood social cohesion and physical disorder influence falls among community-dwelling older adults (≥65 years)? (2) Do functional limitations moderate these associations? The specific focus of our study is on perceived neighborhood environments, whereas neighborhood environments have been captured using various approaches in prior research (Caldwell et al., 2019; Nicklett et al., 2017). Subjective perceptions are particularly relevant as they capture individuals’ lived experiences and interactions with their surroundings (Choi & Matz-Costa, 2018; Liu et al., 2022). Older adults’ perceptions of their neighborhood environment can significantly influence their ability to navigate these spaces safely (Clarke et al., 2023; Kim et al., 2020).
Methods
Data
We utilize data from the Health and Retirement Study (HRS), a nationally representative longitudinal survey of US adults aged 50 and older. Conducted biannually by the Institute for Social Research at the University of Michigan, HRS is funded by the National Institute on Aging (NIAU01AG009740) and the Social Security Administration (SSA). The study employs a complex multistage probability sampling design, with oversampling of Black and Hispanic individuals (REF). Data for our study were drawn from the HRS Core data files and the RAND HRS Longitudinal File, a harmonized dataset constructed by the RAND Center for the Study of Aging with funding from the NIA and SSA (Bugliari et al., 2024). The RAND HRS file compiles cross-wave data from all publicly available HRS waves into a single, user-friendly dataset, facilitating longitudinal analyses. Additionally, we utilized data from the HRS Leave Behind Questionnaire (LBQ), a self-administered survey focusing on psychosocial and lifestyle factors. For the LBQ Surveys, participants in the core HRS interviews are divided into two groups, with half completing the LBQ in alternate biannual years.
Study Sample
We pooled two LBQ half samples to create the baseline dataset (Time 1: 2014–2016). Data from subsequent HRS interviews conducted in 2016 and 2018 were pooled to create the follow-up dataset (Time 2: 2016–2018). Of the 10,199 participants who completed the LBQ in both 2014 and 2016, we first excluded 2,538 participants who were younger than 65 years in Time 1, yielding 7,661 older adults. This age threshold reflects the population at greatest risk for fall-related injury and morbidity (CDC, 2024; NIA, 2022). Because psychosocial measures are not completed through proxies, 93 proxy participants were then removed, resulting in 7,568 participants. To ensure adequate baseline assessment of neighborhood exposures, participants were required to have completed at least two of the four social cohesion items and at least two of the four physical disorder items (Smith et al., 2023); this criterion excluded 196 participants (n = 7,372). We next removed 345 participants who did not complete the falls assessment at both baseline and follow-up (n = 7,027). We excluded those who did not respond to all 16 items of functional limitations at baseline (n = 6,029). Participants living in nursing homes or assisted living facilities at baseline were then removed (n = 141), resulting in 5,888 community-dwelling older adults. Finally, listwise deletion of missing covariate data excluded 813 participants, yielding a final analytic sample of 5,075 participants. Supplemental Figure 2 shows the sample flow diagram. Overall, 14% of the eligible participants were excluded due to missing data on one or more covariates. Items with missing data included income and falls at follow-up (10% and 4%, respectively). Wave-specific participants’ survey weights for the HRS LBQ were applied to account for oversampling and survey non-response (Fisher & Ryan, 2018). Functional limitations, sociodemographic variables, and other covariates were drawn from the HRS Core data and the RAND HRS Longitudinal File at Time 1.
Measures
Outcome Variable
Falls were assessed using self-reported data from the HRS Core dataset at Time 2, representing the follow-up period of 2016–2018 in our study. Respondents were asked whether they had fallen in the past 2 years, with responses categorized as “Yes” (1) or “No” (0). In the HRS surveys, falls are operationalized based on widely accepted definitions as unintended events resulting in a person coming to rest on the ground or at a lower level. Previous studies support the validity of self-reported falls over a one- to 2-year recall period, showing high specificity (91-95%) and acceptable sensitivity (77–89%) (Sanders et al., 2015). The outcome includes both indoor and outdoor falls (Nicklett et al., 2017).
Explanatory Variables
Aligned with the methodology of a previous study, we used two subjective neighborhood characteristics as our exogenous predictors measured in Time 1 that included social cohesion and physical disorder (Law et al., 2025; Nicklett et al., 2017). We extracted data for both these indicators of neighborhood perceptions using LBQ responses in Time 1 corresponding to our study baseline period of 2014-2016. Participants in HRS are asked to assess their feelings about their neighborhoods within a 20-minute walk or approximately a mile from their residences.
The measurement of perceived neighborhood social cohesion in HRS employ a four-item scale that include: (1) I genuinely feel a part of this area; (2) most people in this area can be trusted; (3) most people in this area are friendly; and (4) if you were in trouble, there are lots of people in this area who would help you. Meanwhile, perceived neighborhood physical disadvantage in HRS is evaluated using another four-item scale that include: (1) There is no problem with vandalism and graffiti in this area; (2) people feel safe walking alone in this area after dark; (3) this area is kept very clean; and (4) there are no vacant or deserted houses or storefronts in this area. Responses for both scales range from 1 (strongly agree) to 7 (strongly disagree). We reverse coded the four items in the social cohesion scale and obtained the average from the individual scores to generate an index that ranged from 1 to 7 (Cronbach’s α = 0.86). A higher score indicated a greater level of social cohesion. Similarly, the four items of the physical disadvantage scale were averaged to create an index that ranged from 1 to 7 (Cronbach’s α = 0.84), with a higher score signifying a higher level of physical disadvantage. These measures of neighborhood perceptions were adapted from validated scales (Cagney et al., 2009) and demonstrated robust internal consistency within the current study sample.
Moderator Variable
Functional limitations were assessed at baseline Time 1 (2014–2016) using self-reported measures of difficulties in performing ADLs, IADLs, and mobility-related tasks in accordance with the Katz ADL, the Lawton IADL, and the Nagi Strength and Mobility scales (Das Gupta et al., 2025). ADLs included six essential personal care tasks: dressing, eating, using the toilet, bathing, getting into or out of bed, and walking across a room with IADLs encompassing five more complex daily tasks: managing money, managing medications, shopping for groceries, preparing meals, and making telephone calls. Physical functioning based on the Nagi Strength and Mobility Scale comprised of five tasks: walking several blocks, climbing stairs, stooping/kneeling/crouching, reaching/extending arms up, and lifting/carrying 10 pounds.
For each task, participants reported whether they had “any difficulty” (yes = 1, no = 0). We created a composite limitations index by summing responses across all 16 tasks (range: 0-16), with higher scores indicating greater functional limitations. To categorize functional limitations, participants in our study were classified into three hierarchical levels: no limitations (0) if they reported no difficulties in Nagi, IADL, or ADL tasks; mild limitations (1) if they reported difficulties only in Nagi tasks with no limitations in ADLs or IADLs; and severe limitations (2) if they reported difficulties in at least one IADL or ADL task, regardless of Nagi limitations. This hierarchy reflects the increasing severity of functional decline, with Nagi limitations typically emerging earlier in the disablement process, and ADL/IADL impairments signaling more advanced disability (Das Gupta et al., 2025; Verbrugge & Jette, 1994). ADL or IADL limitations are higher-level functional losses, which are unlikely to occur in the absence of Nagi limitations representing lower-level or foundational functional losses, supporting the hierarchical progression of functional decline in late life (Verbrugge & Jette, 1994).
Control Variables
Factors known to be associated with falls, including fall history, age, gender, race/ethnicity, education, marital status, household income, number of chronic conditions, depressive symptoms and sensory impairments, were considered as covariates (Das Gupta et al., 2025; Lee & Lim, 2023; Montero-Odasso et al., 2022; Nicklett et al., 2017). Prior falls or a history of falls reported at time 1 (baseline study period: 2014–2016) were controlled to account for their predictive influence. Age was measured in years, ranging from 65 and over. Gender was included as a binary variable (1 = female, 0 = male). Race/ethnicity was self-identified and in our study were included using four mutually exclusive categories: non-Hispanic White (reference group), non-Hispanic Black, Hispanic (any race) and non-Hispanic individuals of other races. Marital status was categorized into four groups: married (reference category), separated/divorced, widowed, and never married. Years of completed education were included as a continuous variable, ranging from 0 to 17 years. Total household income was log-transformed to address skewness. Chronic conditions are assessed in HRS using self-reports (yes = 1; no-0) of eight conditions: diabetes, hypertension, cancer, lung disease, heart disease, stroke, congestive problems, and arthritis. Additionally, depressive symptoms (range: 0–8) are measured in HRS using the 8-item Center for Epidemiologic Studies Depression Scale (CES-D). We dichotomized participants’ CES-D scores to obtain a binary depression indicator (yes = 1 = three or more symptoms, no = 0 = fewer than three symptoms). Participants’ cumulative disease burden was calculated by summing the total number of conditions, ranging from 0 to 9. Sensory impairment was assessed using self-reported hearing and visual function in HRS. A binary variable represented hearing difficulties based on responses to the question: “Is your hearing, using a hearing aid if applicable, excellent (reference category), very good, good, fair, or poor?” Similarly, we utilized responses to the question: “Is your eyesight, using glasses or corrective lenses if applicable, excellent (reference category), very good, good, fair, or poor?” to create a binary indicator for visual function.
Statistical Analysis
As shown in Supplemental Figure 1, a pooled cross-lagged design was used to investigate the relationships between neighborhood perceptions, activity limitations, and falls while accounting for baseline covariates. Cross-sectional study designs can yield biased estimates due to their inability to account for bidirectional relationships and temporal dynamics. To address these concerns, we carefully structured the temporal ordering of our study variables by pooling two waves of data, with predictors and moderators assessed at Time 1 (2014–2016) and the outcome (falls) measured at Time 2 (2016–2018).
Study Sample Characteristics (n = 5,075; N = 29,062,628), HRS 2014–2016 and 2016–2018 (Survey-weighted)
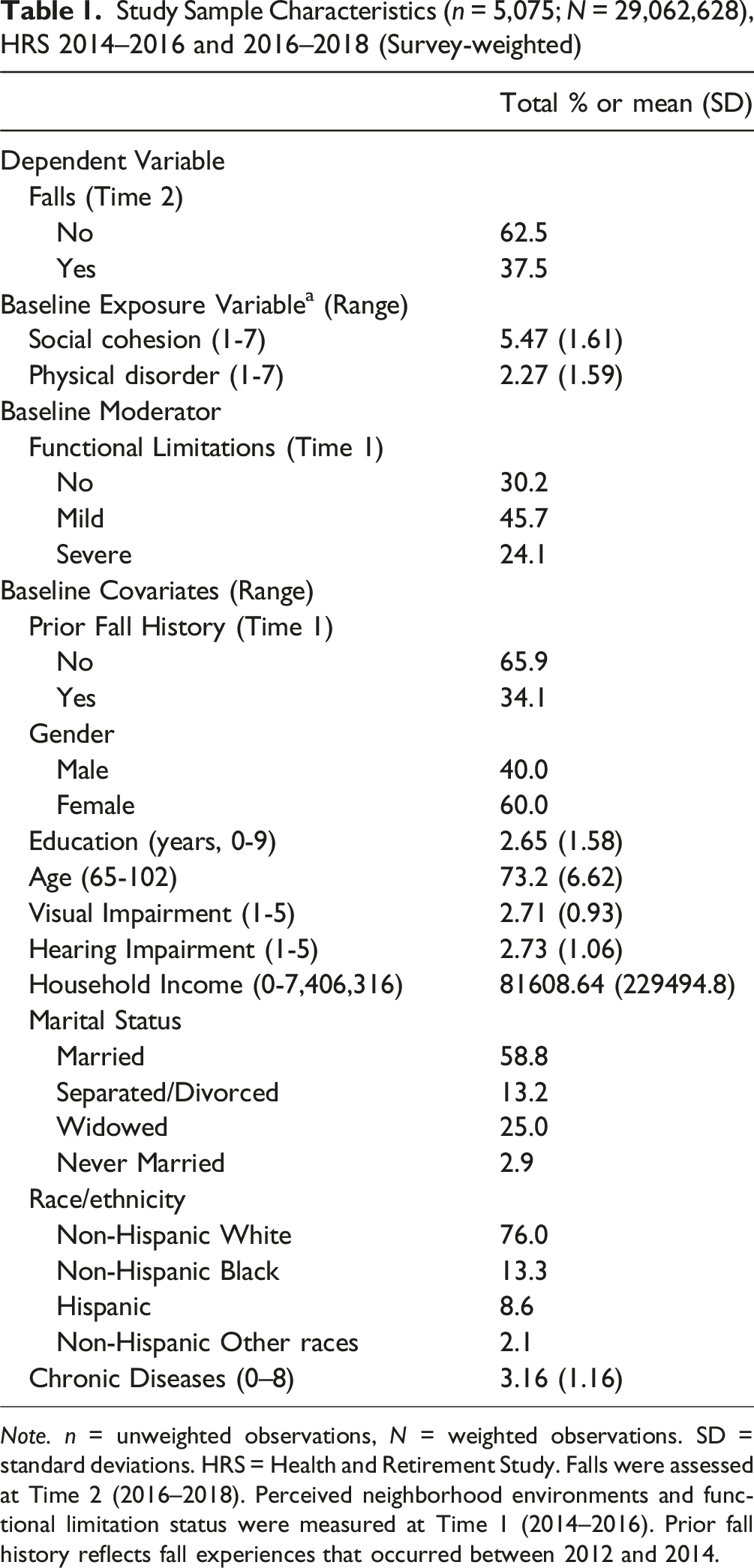
Note. n = unweighted observations, N = weighted observations. SD = standard deviations. HRS = Health and Retirement Study. Falls were assessed at Time 2 (2016–2018). Perceived neighborhood environments and functional limitation status were measured at Time 1 (2014–2016). Prior fall history reflects fall experiences that occurred between 2012 and 2014.
Perceived Neighborhood Environments by Functional Limitations Status and Falls (no versus one or more) of Older Adults (n = 5,075; N = 29,062,628), HRS 2014–2016 and 2016–2018 (Survey-weighted)
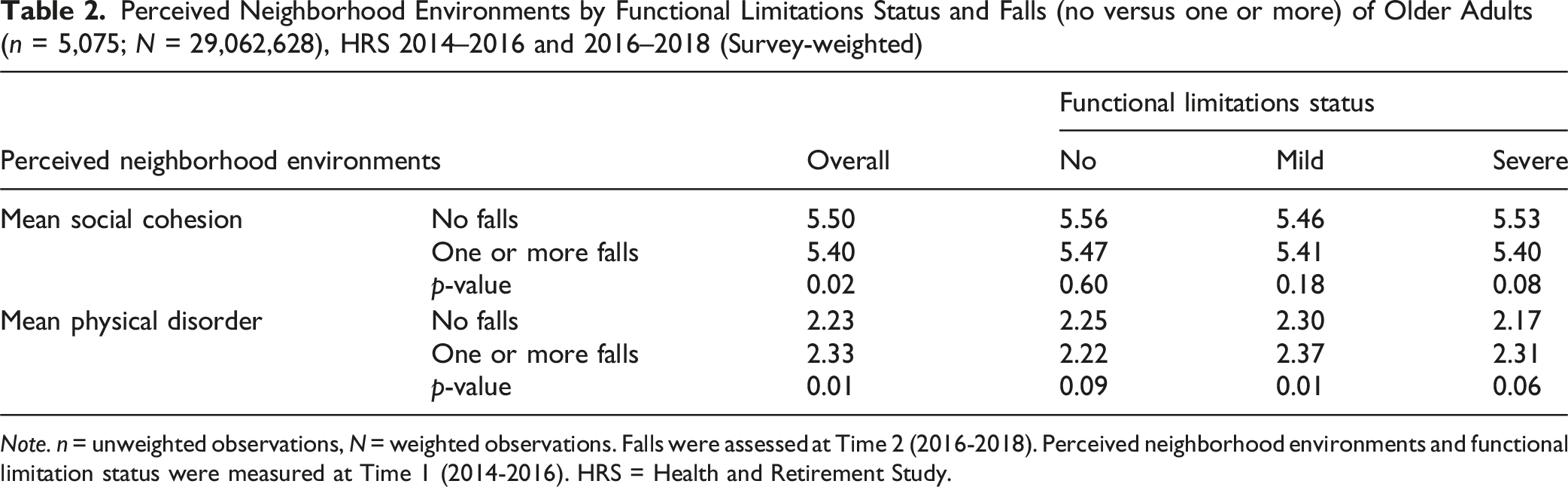
Note. n = unweighted observations, N = weighted observations. Falls were assessed at Time 2 (2016-2018). Perceived neighborhood environments and functional limitation status were measured at Time 1 (2014-2016). HRS = Health and Retirement Study.
Adjusted Odds Ratios and 95 % Confidence Intervals from Multivariable Logistic Regression of Fall Among Older Adults (n = 5,075; N = 29,062,628), HRS 2014-2016 and 2016-2018 (Survey-weighted)
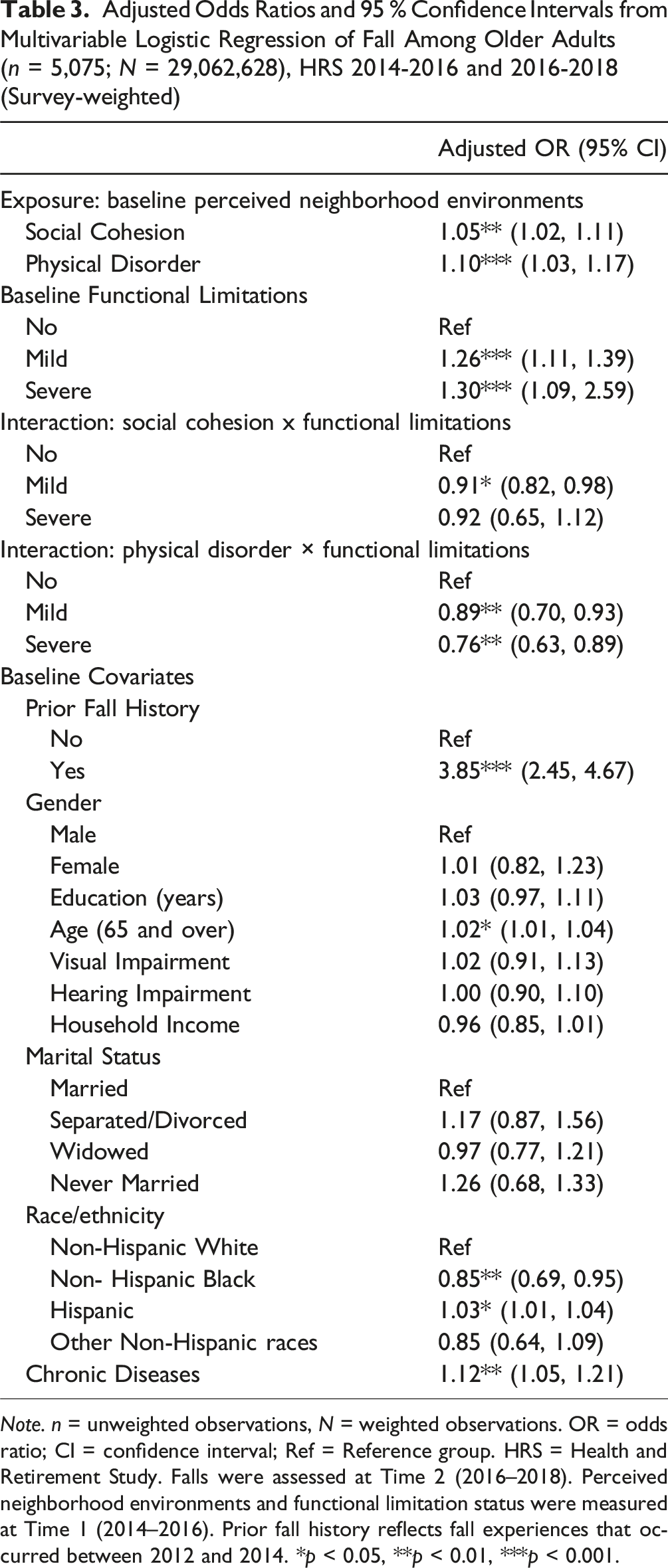
Note. n = unweighted observations, N = weighted observations. OR = odds ratio; CI = confidence interval; Ref = Reference group. HRS = Health and Retirement Study. Falls were assessed at Time 2 (2016–2018). Perceived neighborhood environments and functional limitation status were measured at Time 1 (2014–2016). Prior fall history reflects fall experiences that occurred between 2012 and 2014. *p < 0.05, **p < 0.01, ***p < 0.001.
Results
Table 1 presents the weighted descriptive characteristics of the study sample (unweighted n = 5,075; weighted N = 29,062,628). The study sample consisted mostly of females (60.0%) and non-Hispanic Whites (76.0%), with a mean age of 73.2 years. Approximately 37.5% of the older adults reported experiencing one or more falls during the follow-up period, while 62.5% reported no subsequent falls. The mean social cohesion score was 5.47 (range: 1–7, with higher scores indicating greater cohesion), and the mean physical disorder score was 2.27 (range: 1–7, with higher scores indicating greater disorder). Nearly half of the sample (45.7%) reported mild limitations, 24.1% reported severe limitations, and 30.2% reported no limitations. Additionally, individuals 65 and older reported an average of 3.16 chronic health conditions (range: 0–8). Table 2 shows bivariate associations, examining the mean levels of social cohesion and physical disorder by functional limitation status and fall outcomes. Overall, older adults with one or more falls reported significantly higher levels of physical disorder compared to those without falls (p < 0.01). In comparison, older adults with one or more falls showed marginally higher levels of social cohesion compared to those without falls, with this difference reaching statistical significance (p < 0.05). When stratified by functional limitation status, no significant differences in social cohesion or physical disorder were observed among older adults without functional limitations. However, among older adults with mild functional limitations, higher physical disorder scores were significantly associated with falls (p < 0.01), while differences in social cohesion scores remained non-significant. No statistically significant differences in neighborhood perceptions by fall status were found among those with severe functional limitations (p > 0.05).
Table 3 presents adjusted odds ratios (aORs) from the multivariable logistic regression model predicting subsequent falls among older adults. Table 3 shows both the main effects of perceived neighborhood social cohesion and physical disorder and their interactions with functional limitation status, after controlling for all covariates. For each neighborhood indicator, social cohesion and physical disorder, we calculated the combined effect of these factors at each level of functional limitation by multiplying the coefficient for the main effect with the corresponding interaction effect coefficient.
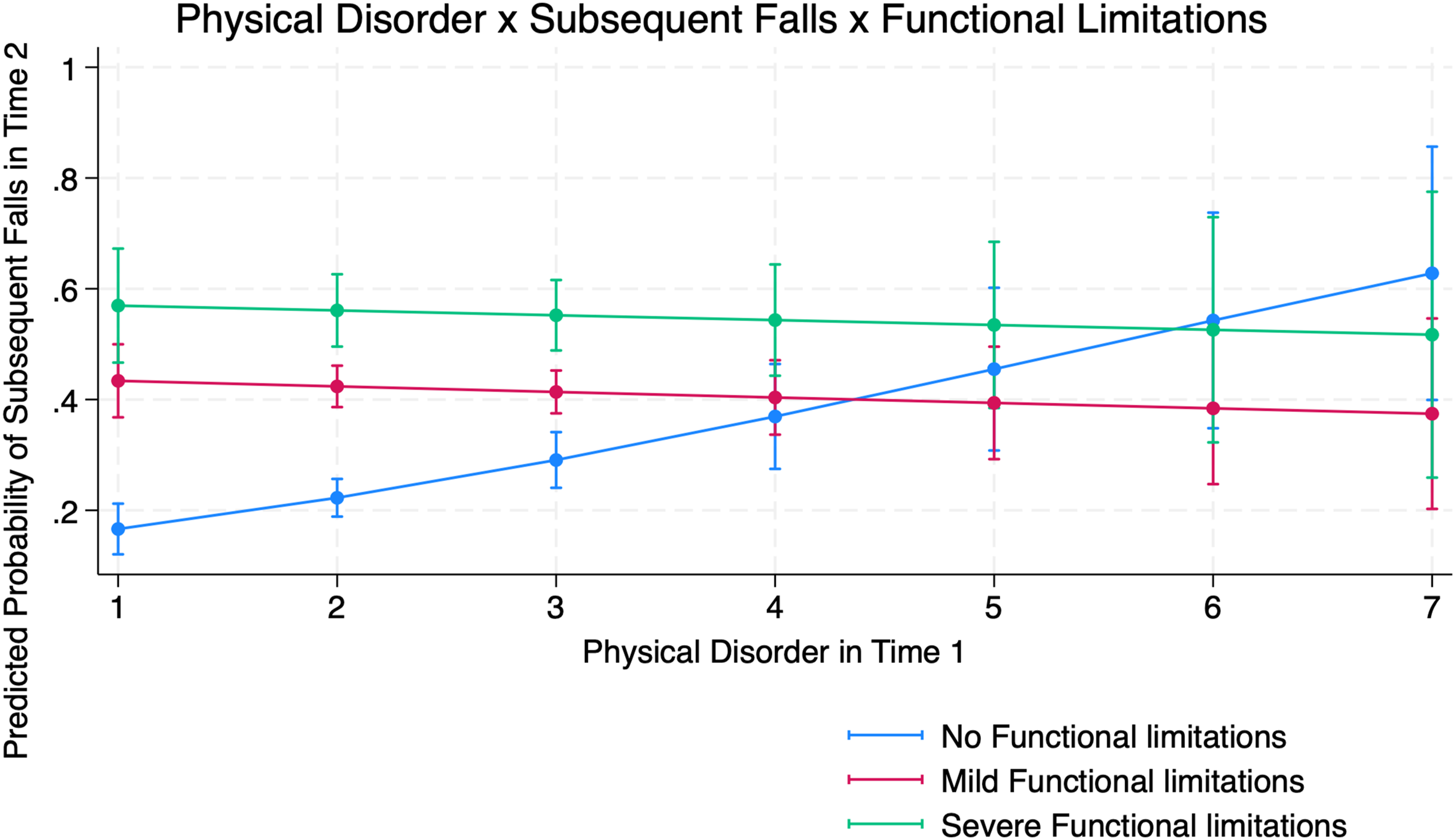
Higher levels of social cohesion were significantly associated with a higher likelihood of subsequent falls (aOR: 1.05, 95% confidence interval [CI]: 1.02-1.11). Among those with mild functional limitations, the effect of social cohesion was attenuated to an aOR of 0.96 (aOR:1.05 × 0.91), suggesting higher social cohesion was associated with less likelihood of subsequent falls among older adults with mild limitations compared to those with no functional limitations. For those with severe limitations, the combined aOR was not statistically significant. Similarly, higher levels of physical disorder were significantly associated with increased odds of subsequent falls (aOR: 1.10, 95% CI: 1.03-1.17). However, among those with mild and severe functional limitations, the effects of physical disorder was attenuated to an aOR of 0.98 and an aOR of 0.84, respectively (aOR: 1.10 × 0.89; aOR: 1.10 × 0.76, respectively), suggesting that higher physical disorder was associated with lower likelihood of subsequent falls among older adults with both mild and severe limitations compared to those with no functional limitations.
The predicted likelihood of subsequent falls: (1) by social cohesion and functional limitations is shown in Figure 1, and (2) by physical disorder and functional limitations is shown in Figure 2. Marginal effects represent changes in the predicted probability of subsequent falls associated with differences in neighborhood characteristics, holding all other covariates. Post-estimation analyses confirmed the validity of the interaction findings. The marginal effects indicated that the association between social cohesion and falls differed significantly between older adults without functional limitations and those with mild limitations, while no difference was observed for those with severe limitations. A similar result was found for physical disorder, where increases in disorder were associated with higher predicted probabilities of falls among older adults without disabilities, but these effects were attenuated among those with mild or severe limitations. Predicted probability of subsequent falls by perceived neighborhood social cohesion and functional limitation status among U.S. adults aged ≥65 Predicted probability of subsequent falls by perceived neighborhood physical disorder and functional limitation status among U.S. adults aged ≥65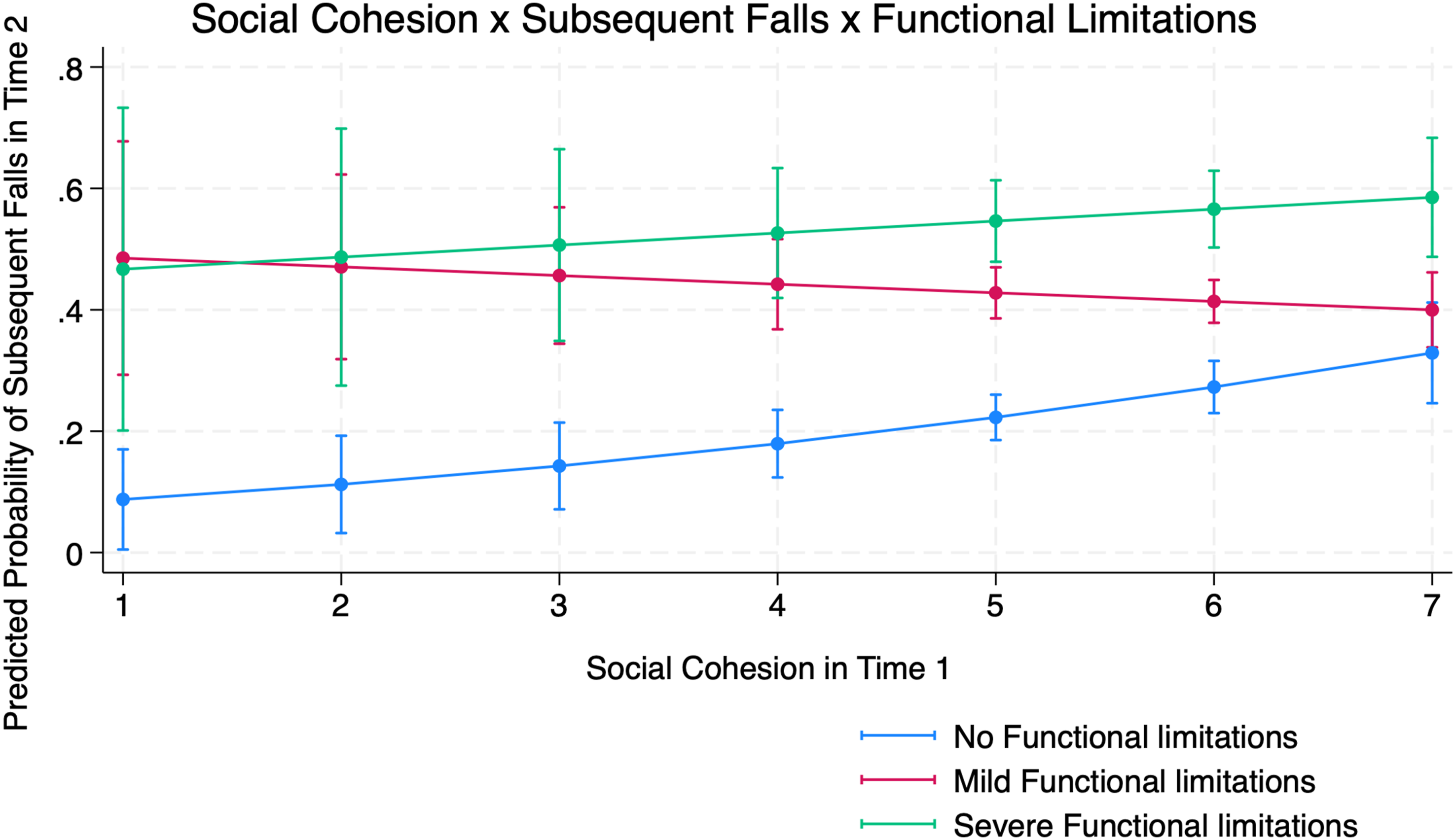
Among the covariates, mild and severe functional limitations were associated with a higher likelihood of subsequent falls (aOR = 1.26, 95% CI: 1.11-1.39; aOR = 1.30, 95% CI: 1.09-2.59, mild and severe limitations, respectively). Baseline fall history was strongly associated with subsequent falls (OR = 3.85; 95% CI: 2.45-4.67). As age increased, the likelihood of falling also increased (aOR = 1.02, 95% CI: 1.01-1.04). Compared to non-Hispanic White older adults, non-Hispanic Black older adults had significantly lower odds of falling (aOR = 0.85, 95% CI: 0.69-0.95), and Hispanic older adults had significantly higher odds of falling (aOR = 1.03, 95% CI: 1.01-1.04). A greater number of chronic conditions was significantly associated with increased subsequent falls (aOR = 1.12, 95% CI: 1.05-1.21). Female gender, years of education, visual impairment, hearing impairment, marital status, and household income were not significantly associated with subsequent falls.
Discussion
Guided by the Competence-Press Model and Collective Efficacy, this study examined the association between perceived neighborhood environments and subsequent falls among older adults, and whether this association is moderated by functional limitation status. Drawing on nationally representative data from the HRS, we constructed baseline (2014–2016) and follow-up (2016–2018) datasets using pooled LBQ half-samples. Consistent with prior HRS analyses, our falls outcome captures any fall in the preceding 2 years and includes both indoor and outdoor events (Nicklett et al., 2017). In adjusted models, both higher social cohesion and higher physical disorder were associated with greater odds of subsequent falls among community-dwelling adults aged 65 and over. These associations were moderated by functional limitations: at higher levels of functional limitation, the positive association between social cohesion/physical disorder and subsequent falls was weaker.
Although neighborhood environments are often conceptualized as determinants of outdoor mobility and hazards, they can also influence fall risk within the home (Lee & Lim, 2023; Nicklett et al., 2017). When older adults perceive their surroundings as unsafe or physically challenging to navigate, they may restrict trips outside, reduce opportunities for routine physical activity, and experience declines in balance and strength (Lee, 2024). Reduced physical conditioning can increase vulnerability to falls during daily indoor activities, such as navigating stairs, bathroom transfers, or reaching and bending tasks that require adequate strength and balance (Kelsey et al., 2010; Nicklett et al., 2017). Therefore, our findings likely reflect both indoor and outdoor fall risks that are shaped by older adults’ behavioral responses to their neighborhood context.
In our study, higher levels of social cohesion were unexpectedly associated with greater subsequent falls among older adults. Although cohesion and neighborhood disorder are inversely associated (r = −0.77), each of these indicators reflects different aspects of the neighborhood environment: disorder represents perceived environmental hazards, whereas cohesion captures trust, reciprocity, and social engagement opportunities (Law et al., 2025). This conceptual distinction suggests that the positive association between social cohesion and subsequent falls may not be related to neighborhood hazards. Instead, the positive association may be due to the fact that higher social cohesion encourages more frequent mobility and activity both inside and outside the home, where falls are more likely to occur. Living in more cohesive communities may foster a greater sense of safety, confidence, and engagement, prompting older adults to remain physically and socially active, hosting neighbors, walking to nearby destinations, or maintaining greater independence in household tasks, which can increase opportunities for falls even when environmental hazards are accounted for (Glass & Balfour, 2009; Michael et al., 2006; Yuen & Carter, 2006). This interpretation is consistent with population-based evidence showing that a substantial proportion of falls among community-dwelling older adults occur outdoors during routine mobility and social participation (Nicklett et al., 2017).
Importantly, because neighborhood environments, functional limitations, and covariates were measured at baseline, and the analyses adjusted for baseline fall history capturing falls during the preceding 2 years, the potential for reverse causation from falls to baseline neighborhood perceptions is minimized. Nevertheless, to assess the robustness of our study findings, we conducted a sensitivity analysis excluding individuals who had experienced any falls in the 2 years preceding baseline (see Supplemental Materials). The results remained consistent, indicating that the associations between study exposure and outcome variables were, in all likelihood, not driven by neighborhood perceptions that may have been shaped by recent fall experiences. Together with our main results, these findings from the sensitivity analysis suggest that higher perceived social cohesion may not uniformly protect against fall risk; rather, it may correspond to greater engagement in physical or social activities that increase exposure opportunities (Glass & Balfour, 2009; Rosenblatt et al., 2021). Future research incorporating repeated measures of social participation and fall context will help clarify these behavioral mechanisms and delineate when and how neighborhood cohesion contributes to or mitigates fall risk.
We also found that functional limitations moderated these associations. Among those with mild limitations, the association between social cohesion and subsequent falls was attenuated, suggesting that cohesive neighborhoods may provide compensatory supports, such as informal monitoring, assistance, or shared resources, that reduce subsequent falls. This is consistent with Collective Efficacy, which posits that cohesive communities can buffer environmental risks through informal check-ins and mutual aid (Cohen et al., 2008). The competence-environment model further clarifies the role of mild functional limitations in the association between social cohesion and subsequent falls, emphasizing that individuals with mild impairments can adapt by leveraging environmental and social resources to maintain functioning (Balfour & Kaplan, 2002; Baltes & Baltes, 1990).
In contrast, for individuals with severe limitations, social cohesion appeared irrelevant to the odds of subsequent falls. Severe limitations often may lead to restricted mobility or home confinement, making neighborhood resources less accessible. Verbrugge and Jette (1994) argued that severe disabilities overwhelm personal and social resources, negating cohesion’s protective effects. Gill and colleagues (2015) also demonstrated that when intrinsic impairments dominate, neighborhood context plays a limited role, which aligns with our non-significant findings for this subgroup.
Consistent with the Competence-Press Model and prior empirical work (Balfour & Kaplan, 2002; Lee & Lim, 2023; Nicklett et al., 2017), findings from this study indicated that higher physical disorder was associated with greater subsequent falls among older adults reporting no functional limitations. Previous studies showed that physical disorder in surrounding residential areas can compromise maintaining balance and physical stability (Balfour & Kaplan, 2002; Caldwell et al., 2019; Lee & Lim, 2023). For example, a study using a national sample of community-residing older adults, found that those living in areas characterized by chronic noise exposure, structural decay, or safety concerns were more likely to experience declines in lower-body functioning and report greater difficulty performing mobility-related tasks (York Cornwell, 2014). Other studies have demonstrated that uneven sidewalks and road surfaces (Li et al., 2006), as well as visible trash and perceptions of safety concerns while walking alone at night (Nicklett et al., 2017), are associated with a greater risk of outdoor falls.
The interaction results representing the moderating role of functional limitations in the relation between physical disorder and subsequent falls were counterintuitive. However, our findings, indicating that higher levels of physical disorder were associated with a lower odd of subsequent falls among older adults reporting either mild or severe functional limitations compared to those reporting no limitations, aligned with prior conceptualizations. According to the Environmental Docility Hypothesis (Morgan et al., 1984), individuals with greater functional limitations are more likely to restrict their mobility in response to environmental challenges, as they feel less safe compared to individuals without functional limitations (Velasquez et al., 2021). Consistent with this explanation, prior work has observed that older adults with mobility impairments often impose constraints on their own activity or remain confined to the home, thereby reducing exposure to neighborhood fall hazards (Gill et al., 2015; Verbrugge & Jette, 1994). As such, older adults living in visually deteriorated neighborhoods who also have mild or severe functional limitations may limit their outdoor activities more strictly, decreasing their exposure to subsequent falls compared to those without functional limitations (Chaudhury et al., 2016). Our sensitivity analyses, using both the composite functional limitation index and domain-specific binary indicators (ADL, IADL, and Nagi), validated our primary results (see Supplemental Materials), demonstrating the robustness of our findings.
Our results indicate the role of policies to prioritize and enable safe activity among older adults who currently restrict participation because of disability. Predicted probabilities from moderation results indicate that lower subsequent falls in mild or severe limitation groups likely reflect self-limiting behavior rather than safer environments. Therefore, it might be beneficial to have payers, particularly Medicare, finance evidence-based, supervised fall-prevention and low-impact exercise programs delivered in controlled indoor settings (e.g., senior centers, community recreation facilities), with adaptive pacing, qualified staff, and explicit eligibility criteria for older adults with mobility, strength, or balance limitations (Sadaqa et al., 2023). This recommendation aligns with the Administration for Community Living (ACL)-funded evidence-based falls prevention programs, such as A Matter of Balance and the Otago Exercise Program, both of which have demonstrated improvements in balance, confidence, and mobility among community-dwelling older adults (Shubert et al., 2017; ACL, 2024). Moreover, because disorderly neighborhoods often coincide with weak transit options, programs may consider bundling door-to-door transportation through senior shuttles or demand-responsive vans and allow transportation as a covered supplemental benefit, consistent with low public transit use among older adults (Gimie et al., 2022). Lastly, delivery of such programs could be tailored by limitation severity. For instance, for mild limitations, emphasizing facility-based participation to prevent functional decline while minimizing exposure to outdoor hazards could be beneficial (Sadaqa et al., 2023). On the other hand, for severe limitations, prioritizing home-based physical and occupational therapy, caregiver training, assistive devices, and basic home hazard remediation, with virtual options when travel is not feasible may be useful (Geohagen et al., 2022).
However, several limitations should be noted. First, HRS does not distinguish whether fall events occurred indoors or outdoors. As a result, we cannot directly attribute increased subsequent falls to specific environmental exposures. Our interpretation acknowledges the possibility that social cohesion may influence fall risk through different behavioral responses, such as greater engagement in community activities increasing outdoor exposure or reduced mobility due to perceived neighborhood challenges increasing vulnerability to indoor falls. Future research incorporating fall location and detailed activity patterns would strengthen the understanding of how neighborhood environments differentially shape both indoor and outdoor fall risks. Second, both predictors and moderators were based on self-reported assessments, which may be susceptible to subjective variability or reporting bias (e.g., social desirability or recall errors). For example, some respondents may overstate neighborhood trust or connectedness to present themselves or their communities more positively or may underreport minor or non-injury falls due to memory lapses. Nevertheless, perceived neighborhood measures capture personally experienced aspects of the environment that are not reflected in objective indicators and are often more strongly related to health outcomes (Lee, 2024; Qin et al., 2024). In contrast, studies using objective neighborhood measures (such as crime rates, walkability, or street and sidewalk conditions) have produced inconsistent findings regarding fall risk. Some studies observed fewer falls in safer or more walkable areas, suggesting benefits for physical activity and balance maintenance, whereas others found higher fall rates in advantaged or highly walkable settings, likely reflecting increased mobility and outdoor exposure (Hoffman & Rodriguez, 2015). These mixed findings may highlight that objective indicators capture structural or environmental risks, whereas subjective perceptions reflect lived experiences and behavioral responses within neighborhood environments, both of which contribute uniquely to fall vulnerability. Third, our analyses captured only short-term relationships between neighborhood perceptions, functional limitations, and subsequent falls. While this approach is valuable for detecting more immediate associations, future research should examine whether and how relationships evolve over the longer term, as cumulative exposure and changes in health status, including physical functioning, may alter odds of subsequent falls. Lastly, the HRS dataset did not allow us to incorporate in-home environmental factors. Future research would benefit from integrating both neighborhood and in-home environmental assessments, including qualitative or observational measures, to provide a more comprehensive understanding of the environmental determinants of falls.
Despite the above limitations, this study draws on nationally representative longitudinal data and uses a prospective design to temporally link baseline perceived neighborhood environments with later subsequent falls. By examining how functional limitation status modifies this relationship, we also add to the understanding of how individual vulnerabilities interact with environmental factors. Overall, this study contributes to the growing body of research emphasizing the role of perceived neighborhood environments in shaping subsequent falls among older adults. By integrating the Competence-Press Model and Collective Efficacy Theory, the findings highlight that perceived physical disorders influence subsequent falls differently depending on older adults’ levels of functional limitations. The results emphasize the need to address both environmental risk structures and individual vulnerabilities, ensuring that older adults across the functional spectrum can navigate their environments safely and maintain a high quality of life.
Supplemental Material
Supplemental Material - Perceived Neighborhood Environments and Falls Among Community-Dwelling Older Adults in the United States: The Moderating Role of Functional Limitations
Supplemental Material for Perceived Neighborhood Environments and Falls Among Community-Dwelling Older Adults in the United States: The Moderating Role of Functional Limitations by Jeein Law, Debasree Das Gupta, Uma Kelekar in Journal of Aging and Health.
Footnotes
Acknowledgment
Authors do not report data, and therefore, the pre-registration and data availability requirements are not applicable.
Ethical Consideration
This study used secondary data from the Health and Retirement Study (HRS). The HRS is publicly available and anonymized, with all data collection protocols approved by the University of Michigan Institutional Review Board (IRB).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.