
Abstract
The Safe Functional Motion Test (SFM-5) is a five item performance based clinical assessment tool quantifying habitual daily movement that may increase the risk of osteoporosis and fractures. Fractures are a major cause of hospitalization and contributor to increased health care utilization costs. A sample of 1,700 adults, aged 40 and older, from an osteoporosis specialty clinic were evaluated to determine if the initial SFM-5 score had predictive utility for determining inpatient hospitalization at 12, 24, and 36 months post fracture. When adjusted for sex, age, and prior hospitalization, logistic regression analyses indicated that the SFM-5 score significantly predicted inpatient hospitalization within 12 months, 24 months, and 36 months. For every 10 point decrease in the SFM-5 score, the 1 year risk of hospitalization increased by 24%. The SFM-5 is a tool to use when assessing habitual functional movements and hospitalization risk among high-fracture risk adults.
Introduction
Hospitalization due to osteoporosis pose a significant threat to the older adult population. Osteoporosis is estimated to be responsible for 1.5 million fractures annually (Becker et al., 2010) and are one of the leading causes of mortality in industrialized countries (Lippuner et al., 2011). Often the fracture is resultant from a fall; in fact, Berry and Miller (2008) indicate that 10 to 15% of falls result in fracture among older adults. According to the CDC (Centers for Disease Control and Prevention, 2016), emergency departments treat 2.5 million older adults for fall related injury and 700,000 of these individuals are hospitalized. Cauley et al. (2016), found that vertebral compression fractures (VCF) were associated with higher risk for hospitalization (40%), and longer hospitalizations (50%), as compared to those with no fracture. Osteoporotic fracture can have a significant impact on the lives of older adults and on the hospital system in terms of cost and utilization.
Issues related to fracture and hospitalization will surely magnify as the population continues to age (Cauley, 2013). Unlike age, many risk factors associated with fragility fracture are modifiable. The key is identifying risk factors and designing necessary intervention strategies to reduce hospitalization and other adverse outcomes. The goal of the current paper is to examine the utility of the SFM in predicting hospitalization among older adults with osteoporosis as the primary diagnosis and are patients in a specialty osteoporosis clinic. The paper also tests the assumption in the literature is that functional assessments (Nayak et al., 2013) and questionnaire-based assessments. This paper follows Eisman et al.’s (2012) call to make the first fracture the last fracture and to work to reduce the risk of the first fracture. The SFM is a five item test of habitual motion designed to test daily tasks around the house which have shown an elevated risk of future fracture and kyphosis (see authors for full definition).
Osteoporosis and other age related changes related to posture and movement can significantly impact movement patterns. MacIntyre et al. (2009), explain that older adults are more likely to develop kyphosis, which can alter movement patterns associated with everyday tasks, making these individuals more susceptible to vertebral fracture (MacIntyre et al., 2014). In fact, SFM is predictive of VCF at 1 and 3 years, as is FnBMD (MacIntyre et al., 2013). These altered movement patterns can make older adults more susceptible to falls, leading to hospitalization for falls including due to fracture, or simply movement-related injury (Budhia et al., 2012). What makes the SFM novel is the analysis of everyday movement in predicting fracture and hospitalization. Habitual movement patterns involve varying levels of whole body movement, which requires strength, balance, coordination, and flexibility. Analyzing normal and compensatory movement due to osteoporosis offers practical insight and allows for more individualized intervention. The prior literature indicate that the SFM is an effective way to measure habitual motion and predicts future fracture (MacIntyre et al., 2013, 2014; Recknor et al., 2019).
Predicting hospitalization has several implications, namely, improving utilization rates in other areas of healthcare and decreasing associated costs. Hospitalization due to fragility fracture can be costly. Using Medicare claims information, Becker et al. (2010), were able to outline patterns of health service utilization associated with fragility fracture and the cost associated with each type of fracture. Ultimately, they found that acute hospitalization significantly increased following fragility fracture, “even among the least severe fracture type. . .there is a 20 percentage point increase in the rate of acute hospitalization (Becker et al., 2010).” Increased hospitalization means increased expense. Ensrud (2013) estimates that fragility fractures cost approximately $20 billion dollars annually. The average patient can expect costs ranging from $7,788 to $31,547 depending on fracture type and severity. This does not include post-acute care and any necessary physical or occupational therapy (Becker et al., 2010). The Centers for Disease Control and Prevention (2016) estimates that two-thirds of direct medical costs associated with fall injuries directly connected to hospitalization.
A comprehensive literature analysis conducted by Budhia et al. (2012), examining the costs associated with osteoporotic fractures. Health resource utilization and decreased productivity following fracture translates to very high costs, in fact, a recent analysis found 2.05 million fractures cost the US more than $16.9 billion (Budhia et al., 2012). The aforementioned Cauley, (Cauley et al., 2016) study also found that patients with fracture had 1.6 to 6.2-fold higher cost than those with no fracture and that the greatest cost is associated with hip fracture. Using SFM to identify those at greatest risk for hospitalization offers an opportunity for intervention, which could lower heath service utilization, decrease non-productive time following the event of a fracture, and reduce overall costs of treatment and rehabilitation. Findings indicated predictive utility up to 36 months post fracture, which allows for a significant intervention period.
Little research examining the direct connection between movement assessments (fracture-related and otherwise) and predicting hospitalization exists. Perhaps it is implied that fracture leads to hospitalization, but the direct implications of such are scantly discussed. By looking not just at predicting fracture, but looking at predicting hospitalization directly, clinicians can work to decrease both fracture rates and overall healthcare costs.
As stated, previous research with the SFM-5 has shown predictive validity regarding osteoporotic fracture (MacIntyre et al., 2014). This study, however, focuses on utility in predicting hospitalization at 12, 24, and 36 months. Hospitalization can be a very challenging event for many older adults. A study by Gardner et al., (2008), note that hospital stays result in a two-fold increase in fracture with risk increasing after each subsequent hospitalization. Hospital stays often result in some decline in lower extremity function, which may result in decline in overall health and/or nursing home placement (Balachandran & Signorile, 2015). In fact, Fisher et al. (2009), found that “30 to 50% of patients aged 65 or older lose some lower body function while hospitalized” (p.2). Poor lower extremity function performance is also predictive of hospitalization (Penninx et al., 2000; Studenski et al., 2003). Tests like the SPPB have validated these findings using samples of hospitalized older adults (Fisher et al., 2009). Research does support that the SPPB is predictive of self-reported and observed disability, nursing home admission, and mortality (Cesari et al., 2009; Guralnik et al., 1994; Vasunilashorn et al., 2009), however, there is limited research regarding the predictive ability of the SPPB on hospitalization directly. The ultimate goal is to use assessments like SFM to predict fracture before it happens, implement preventive interventions, and to avoid hospitalization altogether.
The use of functional assessment tools can help to identify people at risk for fragility fracture in a variety of ways. For example, the TUG measures the time it takes a person to rise from a chair, walk 3 meters, and return to sitting position in the chair (Zhu et al., 2011) whereas the SPPB measures lower extremity function through a timed 4-meter walk, five timed chair stands and a balance test (Fisher et al., 2009). Several sources emphasize the predictive ability of gait speed alone as compared to the entire SPPB batter (Balachandran & Signorile, 2015; Guralnik et al., 2000; Volpato et al., 2008, 2011). The TUG and SPPB are not the only fracture risk assessments. Other assessments, such as the FRAX and FRACTURE, utilize bone mineral density measurements in combination with lifestyle factors to determine fracture risk through Biochemical bone markers (Unnanuntana et al., 2010) smoking behavior, and maternal fracture history (Black et al., 2001). The Safe Functional Motion test (SFM) is a newer test, and unlike its predecessors, the Continuous-scale Physical Function Test and the Physical Performance Test, it measures not only quantitative data associated with movement, but also qualitative aspects of movement. It also measures factors associated with spine loading (Recknor et al., 2019) (IONMed Systems, 2016) and balance (MacIntyre et al., 2009) (VanSwearingen et al., 1998).
The goal of the current study is to examine the utility of the SFM on predicting hospitalization over 36 months among a sample of adults in an orthopedic clinic in Georgia.
Methods
During the study period, 1,700 participants presented to the clinic located in the Gainesville Georgia area of the United States for an initial SFM test. We conducted a retrospective review of anonymized charts for adults who attended an osteoporosis specialty clinic in northeast Georgia between 2004 and 2014 for initial assessment and had 1 year and 3 years follow-up data in the clinic’s database registry. Both men and women were included if they had baseline data for SFM and covariates of interest (age, gender, femoral neck BMD (fnBMD), history of fragility fracture, history of injurious falls, use of osteoporosis medication), and incident fracture(s) at 1 year and/or 3 years follow-up. Medications other than for treatment of Osteoporosis were not included in calculations. Of these individuals, 1,517 were females and 183 were male (Recknor et al., 2019). Actual ages ranged from 47 to 97, with the mean age being 72.3 years. In regards to hospitalization, 1,491 participants (87.7%) had no hospitalizations with 5 years prior to the study, with 209 individuals (12.3%) hospitalized during the length of the study.
The SFM-5 measures physical function based on habitual movements. The SFM-5 is for use by clinicians to analyze habitual movements among people with osteoporosis. The goal of predicting fracture, and in turn, hospitalization (Recknor et al., 2019). The SFM-5 measures specific tasks, including putting on footwear, reaching for a magazine from the floor, sitting to floor task in which the participant sits on the floor with legs out and then comes to a full stand either with or without the use of a chair, carry climb which simulates carrying groceries up stairs, and night walk simulating getting up at night to retrieve an object (for full discussion of each task, see Recknor et al. (2013, 2019). We have provided a Figure 1 (1 About here) to show the layout of the tasks. These tasks specifically mimic activities of daily living (ADLs) for individuals with osteoporosis. A trained clinician monitors tasks, and the computer program assigned a score. Overall SFM scores are assigned to determine patient’s level of risk with potential scores ranging from zero, or no risk, to 100 significant risk. The five items were selected by a clinician as parsimonious and because of reduced and ultimately eliminated reimbursement from Medicare Choice plans in Georgia.
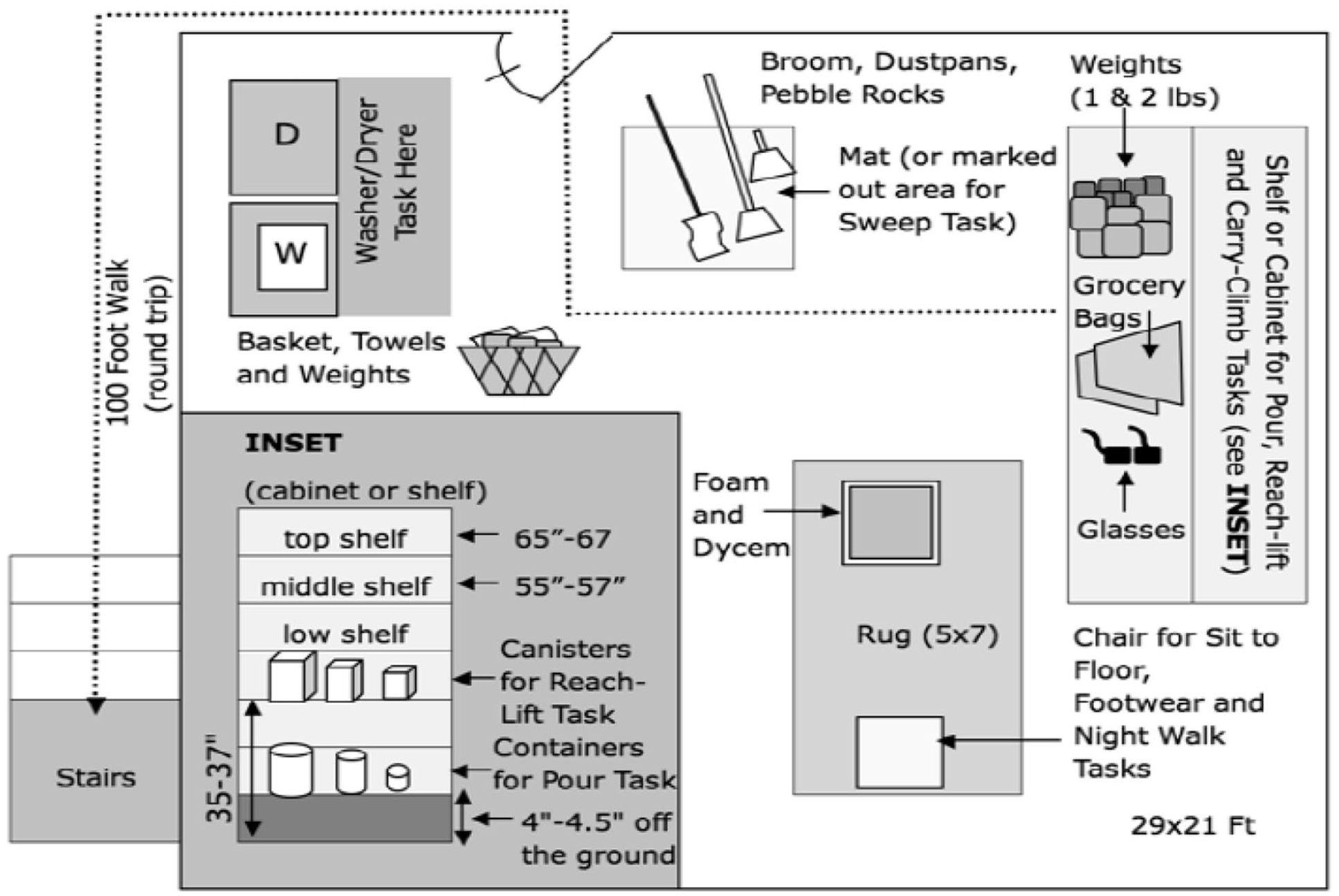
The safe functional motion test room set up.
Statistical Analysis and Results
The sample (see Table 1) was 89.2% female, 10.8% male, and a mean age of 72.3 years (range 47–97). This is not surprising as females are more often diagnosed with osteoporosis. Within the 36-month period of this study, 209 people were hospitalized. The mean SFM score for hospitalized patients was 61.1 versus 76.1 for those not hospitalized at 12 months. At 24-months, SFM scores remained lower for those hospitalized (64.9 vs. 77.5) and at 36-months (65.9 vs. 71.9). Hospitalized patients also tend to be older than those not hospitalized throughout the study.
Demographic Characteristics for Hospitalization within 12 Months, 24 Months and 36 Months Analyses.

Note. Twelve months: Percentages in the Hospitalization/No Hospitalization columns are based on the totals in the All column. Percentages in the All column are based on the total sample of 1,700. V:\Julie\Studies\Hospital Data\programs\Demog.sas ran September 2, 2015 at 14:55.
Twenty-four months: Percentages in the Hospitalization/No Hospitalization columns are based on the totals in the All column. Percentages in the All column are based on the total sample of 1,330. V:\Julie\Studies\Hospital Data\programs\Demog.sas ran September 2, 2015 at 14:55.
Thirty-six months: Percentages in the Hospitalization/No Hospitalization columns are based on the totals in the All column. Percentages in the All column are based on the total sample of 1,058. V:\Julie\Studies\Hospital Data\programs\Demog.sas ran September 2, 2015 at 14:56.
We used Logistic regression to examine inpatient hospitalization at 12, 24, and 36 months. At 12 months, prior hospitalization and SFM scores reached statistical significance see Table 2. SFM score (p < .0001 OR 3.818) and prior hospitalization (p < .0001; OR 1.235 adjusted −10). For every 10-point decrease in the SFM score, the odds of hospitalization within one year increased by 24%. Age and sex pointed toward significance, however did not reach statistical significance within the first 12 months.
Logistic Regression Analysis on Inpatient Hospitalization within 12 Months, 24 Months, and 36 Months Years Using SFM-5.

The next step was to examine 24-month follow up data. Age (p < .5097 OR = 1.184; Wald’s 95% Confidence Ratio: 0.716, 1.958) was significant at the <.05 level. Sex failed to reach statistical significance. Prior hospitalization p < .0001; OR = 3.332 Wald’s 95% Confidence Interval: 2.384, 4.658) were statistically significant. Prior SFM scores (p < .0001; OR = 1.195 (unit = −10); Wald’s 95% Confidence Ratio: 1.100, 1.299) were also statistically significant. For every 10-point decrease in the SFM score the odds of hospitalization within two years increased by 20%.
Finally, we examined 36-month inpatient hospitalization. Female sex (p < .0219; standard error = 0.127; OR = 1.786; 95% Wald’s Confidence Ratio: 1.087, 2.932) was significantly associated with inpatient hospitalization at 36 months. Increased age was significantly associated with inpatient hospitalization (p < .0313; standard error = 0.009; OR = 1.212 (unit = 10); Wald’s Confidence Ratio: 1.017, 1.443).
Prior hospitalization and baseline SFM scores were also significantly associated with subsequent inpatient hospitalization p < .0001; OR = 1.263; Wald’s 95% Confidence Interval: 1.160, 1.375; SE = 0.004. For every 10 point decrease in the SFM score, the odds of hospitalization within 3 years increased by 26%.
Discussion
Functional tests that predict hospitalization are few. SFM has shown to predict fractures (Recknor et al., 2013) and now can predict hospitalization. Findings from this study provide a base from which new research can grow. It has been found that the SFM-5 can significantly predict hospitalization within 12 months using a performance based test that explicitly examined performance and hospitalization. Researchers can use this to look at predictive ability over longer 36 month periods. Clinicians can also use this research base to implement more effective screenings and interventions in their practice. Traditionally, functional assessments like the SPPB have been looked to as predictors of adverse health effects among older adults (Cesari et al., 2009), (Guralnik et al., 1994) . The SFM offers a more comprehensive, practical approach to functional assessment. Future research should investigate which test demonstrates more clinical significance based on criteria such as hospitalization risk and utilization, other forms of elevated healthcare utilization, and fracture risk. Additionally future research should examine potential cost savings versus the cost of administration of each tool.
The SFM tool is a convenient method clinicians can use for assessment of osteoporotic community-dwelling older adults. This test can routinely be utilized and its results incorporated into the evaluation of patients’ risk for hospitalization. This is in addition to its’ utility for predicting fracture (Recknor et al., 2013).
The current research suggests it is necessary to consider the quality of habitual functional movements when assessing hospitalization risk among high fracture risk older adults. These movements are measured using the SFM-5 and mimic everyday tasks allowing assessment and physical therapy techniques to intervene.
The SFM-5 is a tool that can be used to predict vertebral compression fracture at both 1 and 3 years (Recknor et al., 2013), and it has now been shown to predict hospitalization over 36 months. This tool should be used by clinicians and can be used by data analysts within hospitals to identify and reduce hospitalizations.
The results from this study provide an evidence base from which the five item Safe Functional Motion (SFM-5) test significantly predicts subsequent hospitalization at 12, 24, and 36 months. Additionally, prior hospitalization is associated with subsequent hospitalization throughout the 3 years covered by this study. Sex is significant at 24 and 36-month follow up, but not at 12 months. One possible explanation is that time is necessary to examine the trajectory from lower SFM scores to hospitalization remains similar among men and women then diverges.
Clinical Significance
The SFM gives the opportunity to provide early intervention to this at-risk population. The results indicate that one’s function influences their health and hospitalization risk over a three-year period. A person’s function influences health and if they are sick enough to require hospitalization. Function can contribute to wellness. Conversely, a decline in functional status can contribute to events and conditions that may lead to hospitalization, poorer health, and disruption of everyday life due to being in the hospital and the recovery period upon release. A lower SFM score is indicative of decreased function, and elevated hospitalization risk.
SFM is further evidence that functional impairment can increase hospital admission. For clinicians, it is evidence that examination of function is important. The results of this study present strong evidence for the clinician to consider a decline in function in hospitalization prevention. If we can predict a higher likelihood of hospitalization based on a quick test of physical function based on every day, or habitual, motion, it is worth the time based on the potential for decreased hospitalization. This is in addition to evidence that the SFM also helps predict fracture risk (Recknor et al., 2013).
This tool provides an important opportunity for clinicians to implement interventions to prevent the hospitalization, rather than only treating the osteoporosis, and dealing with the immediate and lasting effects of hospitalization. The literature suggests effects of hospitalization on older adults include loss of lower extremity function, decline in overall health, and nursing home placement (Fisher et al., 2009), (Volpato et al., 2008). Early intervention using tools like the SFM-5 can help to mitigate these consequences and keep patients healthy and delay or prevent nursing home placement.
One significant overarching benefit of a potential decrease in hospitalization rate is a decrease in healthcare costs (Stevens et al., 2006). Reducing hospital stays reduces risk of hospital-based infection and preferred by older adults.
There were several strengths of this study. This study retrospectively evaluated all patients enrolled in a larger study and determined the SFM score of those who were hospitalized within a year. The results mirror a similar study by Volpato et al. (2011) yet has a larger number of participants (n = 140 compared to n = 87). Another strength was with the SFM testing procedure itself. The SFM evaluates functional status by a clinician performing hands-on tests of patients rather than relying on patients’ self-report of their ability.
Conclusions
Clinicians should consider adopting this tool to help reduce the risks of hospitalization among older adults with prior factures. The cost savings, according to Becker et al. (2010) range from $7,788 and $31,547 per patient excluding post-acute and therapy costs. The CDC (2016) estimates that two-thirds of direct medical costs associated with fall injuries can be directly connected to hospitalization this represents a significant potential savings of the estimated $20 billion annual cost of fracture care (Ensrud, 2013). This 5-10-minute test may help save costs, and time lost to patients during their hospitalization along with the risks of hospital-based infections and potential lost wages and productivity. Consideration of the improvement of quality of life for those not hospitalized is also important.
Limitations and Directions for Future Research
The SFM is a relatively new clinical assessment. Its utility has now been examined in predicting hospitalization and subsequent fractures (Recknor et al., 2013). Clinicians may now be able to use this tool to assess future risk of hospitalization based on patient performance on the SFM which mimics everyday tasks to examine habitual motion. If changes or limitations occur in the individual performing these tasks, physical therapy or other interventions may be recommended by the clinician to reduce risk of future hospitalization or fracture.
The current study is not without limitations. The sample is from one area of northern Georgia and needs replication in other populations. The sample is primarily white and female. Additional research focusing on minorities and men is necessary. Future research should design and test interventions for specific types of hospitalization using the Safe Functional Motion test by clinicians to reduce subsequent hospitalizations. The focus of the paper is on overall all cause hospitalization, and we acknowledge that the causes of hospitalization are limits of the current paper, and provide an opening for future research. Future research should examine the predictive utility of the SFM-5 on long term care utilization. Exercise and occupational therapy interventions may help at risk older adults compensate for changes in health to make everyday tasks safer. Additional interventions could involve home modifications along with service interventions such as incorporation of direct in-home care assistance and exercise programs targeting habitual motion.
Additional research should also examine the SFM’s utility in predicting other adverse outcomes. These outcomes may include long-term care utilization, medication and falls associated with decrements in safe habitual motion.
Funding for such interventions may come from the Older Americans Act based upon eligibility criteria or through other funding sources. An intervention using these data holds potential to reduce the financial and suffering costs associated with hospitalizations. The research should include specific examination on the types of costs prevented.
Footnotes
Acknowledgements
The authors would like to thank Amy J. Plant, Jessica Moore, Shannon Coyne, and Amber Durkin for their assistance in the formatting and background on this paper. Thank you to everyone who has encouraged us, provided feedback, and guidance on this publication. We would also like to thank Dr. Norma MacIntyre for her help on the development of the original Safe Functional Motion test.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs. Christopher and Julie Recknor are the owners of the United Osteoporosis Centers and helped develop the Safe Functional Motion Test. Dr. Van Dussen was supported by Youngstown State University travel and Faculty Improvement Leave funding. Hospitalization in High Fracture Risk Older Adults with Osteoporosis Using the Safe Functional Motion Test: A Longitudinal Analysis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a Youngstown State University Faculty Improvement Leave and Research Grant to the [DVD]. A brief and earlier version of these data was presented at the International Congress of Geriatrics and Gerontology in 2017 in San Francisco California.
Institutional Review Board Approval
The Northeast Georgia Medical Center’s Institutional Review Board Approved the Protocol FY12-12-397. Every patient was asked if their data could be used for quality metrics and was documented in the EMR system. The data for available patients was gathered from those giving verbal permission.