
Abstract
Introduction
Humans are built for activity (Szostak & Laurant, 2011). Engaging in adequate physical activity (PA) is important for improving and maintaining health. The recommended PA level for healthy older adults is a minimum of 150 min of moderate-intensity aerobic activity per week (Piercy et al., 2018; Sparling, Howard, Dunstan, & Owen, 2015; Sun, Norman, & While, 2013). Maximum benefits appear to accrue from lifelong PA engagement, yet evidence suggests that significant benefits can be obtained from even moderate levels of activity begun and maintained in old age (Piercy et al., 2018). Physical inactivity in all age segments of the population is a growing public health concern. Physical inactivity both hastens and exacerbates many common comorbidities of later life (Kohl et al., 2012; Lee et al., 2012). Increased PA in older adults, however, has been shown to ameliorate or delay the onset and progression of many of these same comorbidities (Taylor, 2014).
Programs designed to increase PA in community-dwelling older adults often use multiple strategies, including face-to-face counseling or training sessions followed by remote contact via telephone, Internet, or standard mail (Zubala et al., 2017). Some programs involve remote contact only, typically directed at individuals as opposed to groups (Müller & Khoo, 2014). Almost all PA interventions incorporate some form of health education or lifestyle counseling. These programs appear to have positive effects on PA levels and self-efficacy, with some studies also suggesting improvement in mood and quality of life (Zubala et al., 2017).
Despite the known benefits of PA, few older adults achieve recommended PA levels, and even fewer participate in programs designed to increase PA (Bethancourt, Rosenberg, Beatty, & Arterburn, 2014; Nguyen et al., 2008). Although access to and affordability of PA programs can play a role, low rates of participation are common even when older adults are referred by a health care provider to a low-cost or no-cost exercise program (James et al., 2008; Nguyen et al., 2008). Many older adults subscribe to the belief that exercise is unnecessary and may even be harmful (Franco et al., 2015). Barriers to PA participation reported by older adults include health concerns such as fear of falling and pain, and attitudinal factors, such as social awkwardness (i.e., feeling intimidated or embarrassed when performing physical activities) and dislike of PA (Bethancourt et al., 2014; Franco et al., 2015).
The “A Matter of Balance” (MOB) program was developed in the 1990s to reduce fear of falling, one of the major barriers to increased PA, and to increase physical, social, and functional activity in older adults (Tennstedt et al., 1998). Originally designed to be implemented by health care professionals, MOB is a group-based program that uses cognitive-behavioral techniques to decrease fear of falling and associated activity restrictions (Haynes, League, & Neault, 2014; Tennstedt et al., 1998). The primary factor contributing to fear of falling is experiencing a fall, with other identified risk factors including self-perceived physical limitations, poor health status, and depression (Lach, 2005; Scheffer, Schuurmans, van Dijk, van der Hooft, & de Rooij, 2008; Vellas, Wayne, Romero, Baumgartner, & Garry, 1997). Of the adverse health consequences that older adults who have fear of falling may experience, decreased PA and increased risk of falling are two of the most serious (Scheffer et al., 2008). Thirty-five percent of older adults report restricting their activity as a result of fear of falling (Fletcher, Guthrie, Berg, & Hirdes, 2010).
Because use of health care professionals for MOB implementation made the intervention expensive and difficult to sustain (Haynes et al., 2014), MOB was adapted for delivery by lay volunteers as the Matter of Balance Volunteer Lay Leader (MOB/VLL) model program (Healy et al., 2008). The MOB/VLL program is administered in a classroom environment employing both didactic and participatory elements (MaineHealth, 2019; Tennstedt et al., 1998). It is an eight-session, in-person, cognitive-based intervention designed to modify multiple factors theorized to influence PA level, including fear of falling, outcome expectations, self-efficacy for PA, and perceived behavioral control. Participants are directly engaged by the Volunteer Lay Leader and the health professional guest presenter through a variety of methods including group discussion, guided problem-solving in how to improve home safety and safely increase PA, role-playing and skill building, exercise training, demonstrations of how to get up from the ground, and setting of realistic goals.
The program has been widely disseminated to communities across the United States, with MOB/VLL classes offered to thousands of community-dwelling older adults (Haynes et al., 2014). However, researchers have not used validated instruments to provide evidence concerning the extent to which the original MOB or the MOB/VLL are effective for increasing PA among older adults. In assessing the effects of the original MOB on PA, the researchers employed a seven-item self-reported intended activity measure rather than a direct measure of activity (Tennstedt et al., 1998). In the study translating MOB to MOB/VLL (Healy et al., 2008), the researchers assessed PA using a modified version of the Physician-Based Assessment and Counseling on Exercise (PACE), which was designed as a readiness for exercise measure (Calfas et al., 1996). In another study, researchers investigating implementation and dissemination of the MOB/VLL program in Texas reported increased PA (from 3.2 to 3.5 days/week of at least 30 min of moderate-intensity PA, p < .001, Cohen d = 0.27) using an unvalidated variant of the Behavioral Risk Factor Surveillance System (BRFSS) survey items to assess PA (Ory et al., 2010). More recently, researchers examined changes in falls efficacy and PA among oldest-old and young-old MOB/VLL participants in Texas (Cho et al., 2014). They measured PA using a single self-report item of the number of days that the participant had been physically active in the previous 7 days (possible scores ranged from 0 to 7). The change in the number of days of reported PA from baseline to post-intervention was used to categorize participants into one of two groups: improvement (scored 1) and no improvement (scored 0).
The primary aim (Aim 1) of the current study was to evaluate the effectiveness of the MOB/VLL program in increasing PA, as measured by a standardized, self-report measure of PA (Rapid Assessment of Physical Activity, Part 1 [RAPA1]) and the MOB/VLL program’s PA measure (MOB-PA). A secondary aim (Aim 2) was to explore, for a separate cohort of older adults recruited from a local senior center, correlations between the self-report MOB-PA and RAPA1 instruments and step counts obtained using an ankle-attached accelerometer (StepWatch™). Our study is important because it provides new evidence concerning the effectiveness of the MOB/VLL program in achieving one of its key intended outcomes, increased PA.
Methods
Research Design
This was a non-randomized pre–post intervention study of a cohort of older adults who participated in the MOB/VLL course (MOB cohort). The study also included an observational component with a separate cohort of community-dwelling older adults (Community cohort) to permit analyses of relationships between MOB-PA and RAPA1 scores and accelerometric data.
Study Participants
Participants were community-dwelling adults age 60 years or older who were recruited from two sources. A MOB cohort (for Aim 1) was recruited from the registration rolls of MOB/VLL classes scheduled to take place in North Carolina over an 18-month recruitment phase. A Community cohort (for Aim 2) was recruited from community-dwelling older adults in Chapel Hill, North Carolina and surrounding communities. Participants were excluded only if unable to comprehend the English-language recruitment information or other study materials. The study was approved by the University of North Carolina at Chapel Hill Institutional Review Board (IRB), and all potential participants were given a description of the study prior to participation.
Recruitment
Researchers recruited individuals into the MOB cohort by providing recruitment packets to be distributed to participants enrolled in upcoming MOB/VLL classes by the organizations enrolling them. Eligible enrolling organizations were identified by phone inquiries of MOB/VLL class providers and hosting organizations involved in previously offered MOB/VLL classes. Each recruitment packet included an introduction letter; a study information sheet; a single survey booklet, including a demographic and health history questionnaire and the RAPA; a gift card selection form; and a pre-addressed postage-paid return envelope. As approved by the IRB, return of completed surveys and other study materials implied consent.
A separate Community cohort was used for Aim 2 because recruitment of subjects for step counter monitoring from among MOB/VLL enrollees was found to be impractical. This impracticality stemmed from the decentralized planning, scheduling, and implementation of MOB/VLL classes in the state of North Carolina, which created a situation in which class enrollees could not be identified and consented within the time frame necessary to obtain a full week of step counter wear prior to the first class. Community cohort participants were recruited by use of bulletin board postings and on-site recruitment at a local senior center. Solicitation materials for the Community cohort employed recruitment language similar to that of materials used by the MOB/VLL program for participant recruitment. Community cohort participants signed a written consent form approved by the IRB.
Procedures
The timeline for the study is illustrated in Figure 1. The MOB cohort was recruited to participate in the study beginning 1 to 2 weeks prior to the first scheduled MOB/VLL class session, when enrollees received the recruitment packet. Enrollees who consented to be in the study completed the survey booklet and the gift card selection form and returned them via the postage-paid envelope. After the end date of the MOB/VLL class (eight sessions delivered over a period of either 4 or 8 weeks), MOB cohort subjects were mailed a second packet with another survey booklet containing the post-intervention data collection booklet and a gift card selection form, to be completed and returned in a postage-paid return envelope. Mailing of the second packet was timed so that the subjects would receive the packet within 1 week of MOB/VLL class completion, when the maximum intervention effect was expected. Subjects who completed and returned the survey booklet were classified as “followed”; the others were classified as “lost to follow-up.” Up to US$15 in gift card incentives (US$5 for baseline survey and US$10 for follow-up survey) were provided for each MOB cohort participant.

Timeline for the study, illustrating procedures for both cohorts.
In addition, the researchers reviewed MOB/VLL program records for MOB cohort participants to obtain study data. These records included attendance records and the first and last session surveys administered and collected by the MOB/VLL Coaches as part of the program’s established self-evaluation procedures. The MOB/VLL PA measure (MOB-PA) is included in both the first and last session surveys. Access to program records was provided to the researchers by the Be Active North Carolina organization, the data collection agency for the MOB/VLL program administration records in North Carolina at the beginning of the study, and later by the North Carolina Prevention Partners, the interim MOB/VLL data collection agency, or by the MOB/VLL hosting organizations.
The Community cohort was recruited from the local community to wear the StepWatch™ step counter for 7 days (Berlin, Storti, & Brach, 2006) at baseline and at a 4-week follow-up. Potential participants provided contact information to the principal investigator, who arranged to meet at a local senior center to obtain consent, administer the baseline survey (including the RAPA and the MOB-PA), configure the step counter, and give instructions in step counter wear and care. Participants were instructed to wear the step counter when not sleeping or bathing during the next 7 days (Berlin et al., 2006; Matthews, Ainsworth, Thompson, & Bassett, 2002), and to record in a study diary when the step counter was put on and taken off. They were contacted by phone at least once during the week of recording to promote adherence to the study protocol and to answer questions. The researcher left voicemail messages when participants could not be reached directly. At the end of the recording interval, the researcher met briefly with each participant to collect the step counter device and diary. Data were downloaded from the device for analysis. These procedures were repeated after a 4-week period to obtain the follow-up RAPA, MOB-PA, and step counter data. Community cohort participants received up to US$20 in gift card incentives (US$10 at the completion of the baseline data collection and US$10 at the completion of the follow-up data collection) for their participation.
Data Sources
The MOB-PA incorporates a truncated and modified version of the PACE instrument. The PACE in its original form was developed based on a Stages of Change model for adopting a new health behavior (Calfas et al., 1996); no validation has been reported in the literature for its use as a PA measure. The MOB-PA consists of six statements of exercise level, with only one to be selected (Instructions: “Mark only one circle to tell us how much you are walking or exercising now.”). An example item, “I do not exercise or walk regularly, but I have been thinking of starting.” Scores range from 1 to 6.
The RAPA (Topolski et al., 2006) is a self-administered, validated questionnaire that quantifies PA level (duration) and intensity (light, moderate, or vigorous). The RAPA consists of the RAPA1, an assessment of aerobic activity, and the RAPA2, an assessment of activities to improve strength and flexibility. The RAPA1 was used in this study as the validated outcome measure of PA. The RAPA1 is a single item with seven statement selections in response to the question “How physically active are you?” The subject is asked to indicate, by answering either “yes” or “no,” whether each statement is true for him or her. An example statement is as follows: “I do moderate physical activities every week, but less than 30 min a day or 5 days a week.” The statements progress from describing very low PA (Statement 1) to very high PA (Statement 7). The subject’s score, which is the highest numbered statement with a “yes” response, can range from 1 to 7.
The StepWatch™ step counter is validated to provide both average total daily step counts (TDSC) and daily minutes of moderate physical activity (DMMPA). The device is a small ankle-attached water-submergible battery-operated commercial product with no moving parts or user controls. The StepWatch™ has been found acceptable for long-term wear by older adults in multiple studies (Bergman, Bassett, Muthukrishnan, & Klein, 2008; Busse, van Deursen, & Wiles, 2009; Coleman, Smith, Boone, Joseph, & del Aguila, 1999; Foster et al., 2005; Resnick, Nahm, Orwig, Zimmerman, & Magaziner, 2001). The device detects, stores, and retains minute-level step counts for up to 1 month of wear.
Statistical Analyses
All statistical analyses were conducted using SPSS v16.0 for Windows.
Sample size
The study was powered based on the primary aim (Aim 1) of determining the effectiveness of MOB/VLL classes in increasing PA for older adults. An intraclass correlation coefficient (ICC) estimate of .025 was used to adjust sample size for multiple subject per class recruitment, based on values of similar measures in a similar population (Smeeth & Ng, 2002). To detect a moderate effect size of 0.5 (Rosenthal, 1996) with power at 80% and the estimated ICC, a follow-up sample size of 37 was calculated. Using a conservative 30% survey response rate, along with a 35% attrition rate, we estimated that we might need to distribute surveys to as many as 190 MOB/VLL class participants.
Aims 1 and 2
Baseline characteristics were computed (mean, range, and distribution) for all participants in both cohorts. Comparisons of baseline demographic, self-rated health, and falls variables were made using chi-square for categorical variables and t tests for continuous variables. For Aim 1, paired t test statistics and confidence intervals in an available case analysis were computed to assess change from pre- to post-intervention in MOB-PA and RAPA1 scores. For Aim 2, relationships between the step counter measures (TDSC, DMMPA) and the self-report measures (MOB-PA and RAPA1) were calculated at both baseline and follow-up for the Community cohort using Pearson’s r correlations. In addition, Pearson’s r correlations between MOB-PA and RAPA1 scores were calculated at both baseline and follow-up for both cohorts in a complete case analysis. The alpha level was set at .05 for all analyses.
Results
Results for Aim 1
Nine MOB/VLL class provider organizations agreed to assist with subject recruitment by distributing recruitment packets to class enrollees. A total of 108 recruitment packets were delivered to the MOB/VLL class provider organizations, and the provider organizations addressed and sent 93 of these packets to individuals enrolled in upcoming MOB/VLL classes (see Figure 2 for study flow diagram). Fifty-six valid baseline surveys were returned (60.2% response rate, double our estimate of 30%), all containing valid RAPA1 scores. Due to lost or incomplete records from the provider organizations, MOB/VLL first session surveys (including the MOB-PA) were missing for 14 subjects, resulting in a total of 42 subjects from the MOB cohort with complete baseline data for both the RAPA1 and the MOB-PA.
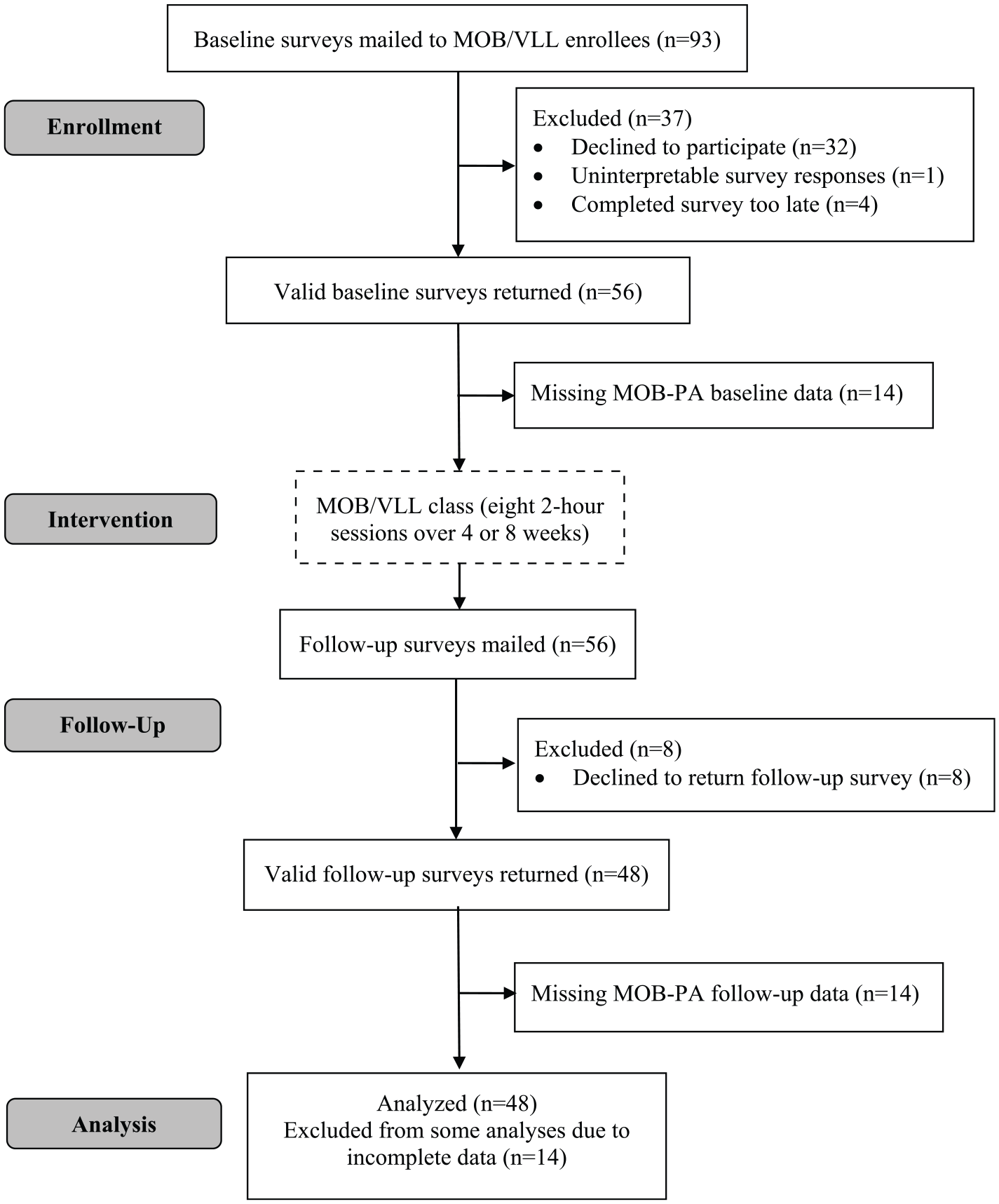
Flow of MOB cohort participants through the study.
Follow-up surveys were mailed to all 56 subjects who returned a baseline survey. Forty-eight (85.7%) returned a valid follow-up survey (attrition rate = 14.3%). All of these subjects had valid RAPA1 scores. Thirty-five of the subjects had valid MOB-PA scores. There were 34 subjects with complete baseline and follow-up RAPA1 and MOB-PA scores.
The baseline descriptive statistics are shown in Table 1. There were no differences between the followed (n = 48) and the lost to follow-up (n = 8) groups for age, ethnicity/race, BMI, self-reported health status, Activities-specific Balance Confidence (ABC) scale scores, or baseline RAPA1 scores. All eight subjects lost to follow-up were female, compared with 77.0% female in the followed group. The lost to follow-up group had higher baseline MOB-PA scores (p < .001) and fewer injurious falls in the previous year (p < .01).
Sample Characteristics of the MOB Cohort.

Note. Health status assessed by self-report using 0-10 Likert-type scale with anchors of “poor” and “excellent.” MOB = matter of balance; BMI = body mass index; ABC = activities-specific balance confidence score; RAPA1 = Rapid Assessment of Physical Activity, Part 1; MOB-PA = Matter of Balance physical activity measure.
Significant at p < .05.
Results of the paired t tests comparing baseline and follow-up scores on the PA measures are shown in Table 2. No significant effects of the MOB/VLL intervention were found for either the RAPA1 (p = .37, Cohen’s d = 0.17) or the MOB-PA (p = .33, Cohen’s d = 0.17). Two post hoc analyses were conducted, the first with subjects with baseline RAPA1 scores below 6 (to address ceiling effects) and the second with subjects attending five or more of the eight MOB/VLL classes. We chose a minimum attendance of five sessions because the original MOB developers considered attendance at five or more sessions necessary for achieving a treatment effect (Tennstedt et al., 1998), and this criterion is used by MOB/VLL for determination of class “completion.” Results of the post hoc analyses are shown in Table 3. These analyses revealed a significant improvement in RAPA1 score from baseline to follow-up for subjects who had a baseline RAPA1 score of 5 or lower.
Results of Statistical Comparisons of Baseline to Follow-Up Scores for the MOB Cohort.

Note. MOB = Matter of Balance; RAPA1 = Rapid Assessment of Physical Activity, Part 1 score; MOB-PA = Matter of Balance physical activity score.
Results of Post Hoc Analyses for the MOB Cohort.

Note. MOB = Matter of Balance; RAPA1 = Rapid Assessment of Physical Activity, Part 1 score; MOB-PA = Matter of Balance physical activity score.
Significant at p < .05.
Results for Aim 2
A total of 25 subjects were recruited from the community to wear step counters. Twenty-three of these subjects successfully completed the baseline survey and the wearing of the step counter for at least 4 of the 7 days during the baseline period. Of these 23 subjects, 14 were available to participate in the 4-week follow-up survey and completed the second wearing of the step counter for at least 4 of the 7 days. One of these subjects failed to complete the follow-up RAPA1.
The Community cohort had a mean (SD) age of 71.7 (6.7) years, significantly younger than the MOB cohort (p < .01). They also had a higher self-rated health status, as measured by an 11-point Likert-type scale rating of “current physical health” with anchors of “poor” (0) to “excellent” (10). The two cohorts did not differ significantly by race, ethnicity, falls history, or baseline RAPA1 scores.
For the Community cohort at baseline (n = 23), the correlation between the MOB-PA scores and the step counter–derived measure of TDSC was significant (r = 0.44, p = .03), as were the correlations between the RAPA1 and both the TDSC (r = 0.57, p < .01) and the DMMPA (r = 0.44, p = .04) (see Table 4). Among the followed subjects (n = 14), correlations between the MOB-PA and the step counter measures (TDSC, DMMPA) could not be computed at baseline because all baseline MOB-PA values had a score of 6, the highest possible score. The correlation between RAPA1 and the TDSC at baseline approached significance (r = 0.52, p = .06) for the followed subjects. No significant correlations between the MOB-PA or the RAPA1 and the step counter measures were found at follow-up.
Correlations Among Physical Activity Measures for the Community Cohort.

Note. MOB-PA = Matter of Balance physical activity score; RAPA1 = Rapid Assessment of Physical Activity, Part 1 score; TDSC = average total daily step counts; DMMPA = daily minutes of moderate physical activity.
Value could not be calculated; baseline MOB-PA scores had the same value (6) for all followed subjects.
Missing RAPA1 score for one participant at follow-up.
Significant at p < .05.
Correlations Between MOB-PA and RAPA1 Scores
MOB-PA scores were not significantly correlated with RAPA1 scores for the MOB cohort at baseline or follow-up. The largest Pearson’s r value for this relationship in the MOB cohort was r = 0.30 for followed subjects at baseline. Although MOB-PA scores were significantly correlated with RAPA1 scores for the Community cohort at baseline (n = 23, r = 0.72, p < .001), this relationship was no longer present at follow-up (n = 13, r = 0.04, p = .91).
Discussion
The results of this study do not support a significant increase in PA for older adults who participate in MOB/VLL classes. One explanation for this finding is that the MOB/VLL program’s recruitment and enrollment processes (which were independent of study enrollment) resulted in a sample of participants with relatively high levels of PA (mean baseline RAPA1 score = 5.0, where 5 = “I do vigorous physical activities every week, but less than 20 min a day or 3 days a week.”) and relatively high balance confidence, as indicated by a mean ABC score of 69.8, which is above the cut point (67) indicative of an increased risk of falling (Lajoie & Gallagher, 2004). Inclusion of participants who had high activity levels at the time of enrollment may have obscured a true effect for the remaining, less active participants.
In the post hoc analysis of participants who scored below the maximum value on the RAPA1 at baseline, a significant, large (Cohen’s d = 1.17) improvement in scores (p < .001) was detected for the RAPA1 variable. This result supports the idea that the MOB/VLL program may be enrolling participants who are not appropriate for an intervention designed to increase PA and balance confidence, given that many participants did not appear to be limiting their activities because of concerns about balance or falls. However, the results of the post hoc analysis should be interpreted with caution, as the mean of the lower half of a normally distributed variable X may be lower than the mean of an uncorrelated variable Y which has the same range and distribution of X (a mathematically deterministic outcome).
Another explanation is that the PA instruments used in this study may not have been adequate to detect moderate individual changes. The limited range of possible scores on the RAPA1 and the MOB-PA may greatly limit responsiveness to change. Ten (20.8%) of the 48 followed participants had a baseline RAPA1 score at the maximum value of 7 (ceiling effect). Ceiling effects were even more pronounced for the MOB-PA, with 17 (50%) of the 34 participants with both baseline and follow-up MOB-PA data having the maximum score of 6 at baseline. The MOB-PA’s ceiling effects have not precluded statistically significant improvements on this measure in previous research, however. Healy and colleagues (2008) found a significant increase in MOB-PA scores 2 weeks post-intervention, (baseline score = 4.8, 2 weeks post-intervention score = 5.4, change = 0.6, p < .001). Despite a lower baseline MOB-PA score in the present study, no significant improvement occurred (baseline score = 4.6, follow-up score = 4.9, change = 0.3, p = .33).
An important difference between our study and previous research (Healy et al., 2008; Ory et al., 2010; Ullmann, Williams, & Plass, 2012) is that our data were collected independent of the MOB/VLL classroom environment (setting, instructors/coaches, other participants). When measures are administered in association with MOB/VLL sessions, participants may be more likely to report the types of changes that they believe their instructors expected or that they themselves expected (participant response bias). In non-blinded studies, self-report measures are highly vulnerable to response bias, and the size of the bias is not trivial (Wilshire, 2017).
Other possible explanations for the findings of the current study relate to the timing of the intervention and the assessments. Although the intervention interval in the present study was 8 weeks (one session/week) for all but two MOB/VLL classes (20 subjects), the MOB/VLL intervention was more intense (two sessions/week over 4 weeks) in the Texas MOB/VLL implementation and dissemination study reported by Ory et al. (2010). The intervention may be more effective for increasing PA at this higher intensity level. Individuals attending the MOB/VLL program 2 times per week may report higher levels of PA than those attending once a week simply by virtue of the PA occurring during the program sessions or associated with travel to and from the sessions. Alternatively, a longer duration of the intervention, with inclusion of a “booster session” at 2 to 6 months after program completion as recommended by Tennstedt and colleagues (Tennstedt et al., 1998), may produce better outcomes. Sartor-Glittenberg and colleagues (Sartor- Glittenberg et al., 2018) suggested that the beneficial effects of MOB participation may require more time than is available during the direct intervention, so that follow-up data should be collected at specific time points (e.g., 2 weeks, 2 months, 6 months) after program completion.
In the Community cohort, RAPA1 scores were significantly correlated with both of the step counter–derived measures (TDSC and DMMPA) at baseline, as would be expected for a validated instrument like the RAPA1. Although the correlations were not statistically significant in the follow-up group, possibly due to the smaller sample size (n = 14), the magnitude of the correlations at follow-up (r = 0.39 to r = 0.47) was generally consistent with that at baseline (r = 0.23 to r = 0.57), affirming the external validity of the RAPA1. The MOB-PA appears to have more drawbacks as a measure of PA for this population, with a more truncated range of scores, greater ceiling effects, and less consistency in magnitude of correlations across the two assessment periods. Although we expected moderate (r ≥ 0.5) concurrent validity between MOB-PA scores and RAPA1 scores, this was found only in the Community cohort (r = 0.72) and only at baseline. This may have resulted from measurement issues associated with both of these instruments, but particularly the MOB-PA.
The present study had several strengths. First, it was conducted with no direct involvement and no influence (e.g., funding) from agencies or organizations that promote MOB or provide any level of MOB training. Second, it used validated instruments (RAPA1 and StepWatch™ step counter) to quantify PA. Third, it obtained its measure of PA away from the influence of the MOB/VLL class environment.
The present study also had several limitations. First, the sample size was small, powered to detect a moderate or larger effect only. Small intervention effects may have been missed. A second limitation was the lack of a control group. In a cohort of older adults assumed to be limiting their activity due to fear of falling, it is possible that the intervention was protective of function, serving to maintain activity levels which might otherwise decline. However, given the high PA of our sample and the short interval between baseline and follow-up, control group decline, had we had a control group, seems unlikely. A third limitation was the relative insensitivity of the RAPA1 to small changes in PA levels. Given the wide activity range covered by the seven sections, a change in score of 1 point arguably represents a clinically significant change, yet clinical significance may exist at a lower (unmeasured) level. A review of the literature did not uncover reports of Minimal Detectable Change (MDC) for the RAPA. Although the RAPA was selected for its low subject burden, an activity measure such as the Community Healthy Activities Model Program for Seniors (CHAMPS) questionnaire (Stewart et al., 2001) may be a better measure to detect smaller changes in this population.
Conclusion
This study found no evidence that MOB/VLL program participation results in an increase in PA. We found some indication that individuals with lower initial PA levels may benefit. Consideration should be given to modifying MOB/VLL program recruitment and enrollment procedures to target older adults who are likely to experience meaningful improvements in PA levels. The MOB-PA may be an inappropriate instrument for measuring activity levels and/or activity level changes in the MOB/VLL program.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health (NIH), through Grant Award Number 1ULTR002222-01. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.