
Abstract
Family carers increasingly take on the responsibility of self-management of dementia as the condition progresses. However, research on this topic is scarce. This scoping review aimed to identify the key characteristics related to self-management of dementia by carers including its components, theoretical/conceptual frameworks that underpinned these components and measurements. A scoping review was conducted in 8 databases and 16 publications met the inclusion criteria. Twenty-two components were identified and grouped into two categories: activities and carer characteristics and skills. The identified theoretical/conceptual frameworks were numerous and varied as were the measures. There was a little consistency of the key characteristics of self-management of dementia by carers. The findings assist carers and healthcare providers to understand the components involved in self-managing dementia which will guide the development and delivery of self-management support interventions for carers. Further research is required to validate these findings and to develop specialized conceptual frameworks and measures.
Introduction
Healthcare providers worldwide are challenged to deliver care to people living with chronic conditions (Grover & Joshi, 2015). In the past the person with the chronic condition was a passive recipient of health care yet this approach is no longer preferred (Grover & Joshi, 2015). It is now recommended that healthcare providers enable people to undertake an active role in the management of their chronic condition, which means they must be more informed, involved, and empowered to manage their condition. The involvement by people in the management of their chronic conditions is referred to as self-management (Barlow et al., 2002; Newman et al., 2004). Effective self-management is the foundation of optimal management of chronic conditions; however, it has different meanings according to the context of its use (McGowan, 2012; Newman et al., 2004). For example, self-management of asthma focuses on preventing the exacerbation of coughing and wheezing while self-management of arthritis focuses on reducing pain (Newman et al., 2004). Self-management is often confused with the self-care concept (Nichols et al., 2020). However, increasingly self-care is defined as the ability of individuals, families, and communities to promote health, prevent disease, and maintain health while, as mentioned above, self-management relates only to chronic health conditions (Nichols et al., 2020).
Self-management of dementia is an emerging concept (Quinn et al., 2015; Taylor et al., 2014). Factors such as difficulties in getting a diagnosis, loss of hope, and shortages in health and social support services have hindered its development (Mountain, 2006). Most dementia literature has focused on self-management by people in early stages (Martin et al., 2013; Quinn et al., 2016; Shehadeh, 2019). Possibly because the labeling of this concept implies that it is only the responsibility of the person diagnosed with dementia. However, it is recognized that another person can be involved in the self-management of the chronic health condition (Ryan & Sawin, 2009; Sattoe et al., 2015). For example, self-managing children’s asthma is carried out by their parents. People with dementia are expected to live between 3 and 14 years after the diagnosis (Onyike & Diehl-Schmid, 2013). During this period, they gradually lose their ability to care for themselves and managing the symptoms of dementia increasingly becomes the responsibility of unpaid or family carers (Huis In Het Veld et al., 2015).
Effective self-management of dementia by carers requires carers to preserve the personhood of their care recipients regardless of the progressive degenerative nature of the disease (Berenbaum et al., 2017; Chung et al., 2017). In this case, carers are required to meet the needs, preferences, and wishes of care recipients while managing their caregiving role. Carers may find their role satisfying since they are taking care of their loved ones. Nonetheless, the caregiving role can result in considerable adverse physical, psychological, and social consequences on the carer and also impacts on the person with dementia (Huis In Het Veld et al., 2015). Given the complex nature of this concept, and in order to effectively support the self-management of dementia by carers, a clear and a comprehensive description of the constituents of this concept is needed. This review aimed to identify key characteristics related to self-management of dementia by carers including its components, theoretical frameworks that underpin its descriptions and the way effective self-management of dementia by carers is determined.
Methods
A scoping review design was used (Arksey & O’Malley, 2005). This type of reviews answers broad questions and is used to clarify concepts (Peters et al., 2015).
Search Strategy
Eight databases were searched including Medline, PsychInfo, and CINAHL (Supplemental File 1). The used search terms were: “self-management” AND (“dementia” OR “Alzheimer”) along with relevant Subject Headings. Other relevant terms, such as caregiving, self-care, self-efficacy and resiliency, were not used in order to investigate the uniqueness of self-management concept. Each database was searched from inception until April 2020. A manual search was performed by reviewing the reference lists of the included publications.
Inclusion and Exclusion Criteria
Several types of scholarly publications were included if they provided a clear description of self-management of dementia by carers. These were: peer-reviewed research articles, protocols, book chapters, a review, and a case study. Publications about self-management by people in early stages of dementia only or by both the person with dementia and the carer together were excluded because this review focused on carers. We also excluded publications in languages other than English or were primarily focused on related concepts such self-efficacy, self-care, or care management.
Search Results
The search resulted in 656 unique publications. Three hundred and eight were not about dementia, 299 were not about self-management of dementia by carers based on examining their titles and abstracts. The full texts of the remaining 49 publications were examined. Twenty-seven were conference abstracts that did not provide enough information to be included, and six did not provide a clear description of self-management of dementia by carers. The remaining 16 were included. The inclusion and exclusion of publications was done by the first author and verified by the other two authors. Disagreements were solved by consensus. Supplemental File 2 shows the PRISMA flow diagram.
Data Extraction
Text and tables were used to extract the following data:
(1) The publications’ types, aims, originating disciplines and locations, sample size and stage of dementia, and outcome measures of self-management.
(2) The descriptions of self-management which consisted of words or strings of words that constituted a clear description of self-management of dementia by carers. The length of the descriptions depended on the provided details in the original source. The wording of the descriptions was kept as close as possible to the original wording to remain close to the raw data to delineate the components.
(3) The theoretical/conceptual frameworks.
(4) Measures of self-management of dementia by carers.
All authors were involved in data extraction and disagreements were solved by consensus.
Data Analysis
The analysis involved organizing and summarizing the extracted data by using text and tables to meet the aims of this review (Tables 1 and 2; Supplemental Files 3 and 4). Content analysis (Graneheim & Lundman, 2004) was used to clarify the elements of self-management of dementia by carers. This type of analysis is used to determine the presence of certain words or within texts or sets of texts (Graneheim & Lundman, 2004). First, essence-capturing codes were used to group the words and sentences that described the same aspect in the extracted descriptions and the frequencies of their occurrences were counted. The codes revealed the essential components of self-management of dementia by carers. Then, the codes were further grouped into overarching themes. After that, the theoretical/conceptual frameworks, and ways of measuring self-management of dementia by carers were extracted, categorized, and frequencies counted. All authors were involved in data analysis and synthesis. To minimize the risk of bias, the authors’ pre-understanding as nurses were bracketed and disagreements were solved by consensus.
The Components of Self-Management of Dementia by Carers in the Included Publications.

Theoretical and Conceptual Frameworks of Self-Management of Dementia by Carers.

Results
Characteristics of the Included Publications
Supplemental File 3 lists the included publications’ originating discipline, location, design, aim, sample size, stage of dementia, the extracted descriptions of self-management of dementia by carers, the used theoretical and conceptual frameworks, and the outcome measures. All except three have been published since 2015. There were five qualitative, three feasibility studies. There were two protocol papers, two quantitative studies, two book chapters, one mixed methods study, one meta synthesis review. The originating discipline of most of the publication was psychiatry (n = 6) and public health (n = 6). The others originated from medicine, nursing, and social sciences. Most of the publications were from Europe (n = 12), three from China and Taiwan, and one from USA.
The range of samples for the qualitative studies was 20-31 while for the quantitative 28 to 81 participants. Six publications recruited carers of all dementia stages (mild, moderate, and severe), half of them based their classification of stages from when the first symptoms were noticed (e.g., <2 years; 2 to 4 years; and >4 years) while the other half did not provide a criterion. Five publications did not specify a stage of dementia. Four publications addressed self-management of dementia by carers in mild stages, half of them based their classification on the score of care recipients on the Clinical Dementia Rating scale by Morris (1997) while the other half did not provide a criterion. Only one publication addressed self-management of dementia by carers in severe stages based on the time since the dementia was first diagnosed, 10 years.
Description of Self-Management of Dementia by Carers
Descriptions of self-management of dementia by carers for the included publications are contained in Supplemental File 3. Content analysis of these descriptions revealed 22 components of self-management of dementia by carers (see Table 1). The resulted components were grouped into activities and carer characteristics and skills. Table 1 lists the components and the publications in which they were described. Supplemental File 4 provides detailed descriptions of the identified components for each publication. No single publication described all of the components. The most frequently described component was carers maintaining their and care recipients’ psychological wellbeing (n = 13/16). The least described component was sustaining behavior changes that facilitate care of the recipients (n = 1/16). Many of the publications missed describing many of the components. For instance, eight publications did not describe either understanding the disease or managing the relationship with care recipients. Also, seven publications did not describe either the carers keeping themselves and care recipients physically well, or the carers maintaining their social relations, the care recipients, and as a couple. Surprisingly, only six publications described carers using health and social support services for themselves and care recipients. Characteristics and skills were also not frequently described in the included publications. For instance, only two publications described goal-setting and making decisions.
Activities
Three categories of activities emerged from the descriptions provided by the included publications. These were activities related to dementia, living with dementia and psychosocial wellbeing.
Dementia: These activities were performed by carers to manage the disease, dementia, for the person living with dementia and included the following four actions: (1) carers understanding the disease; (2) carers responding to changed behaviors and other symptoms on the care recipients; (3) carers getting the diagnosis and helping care recipients to accept it; and (4) carers managing symptoms of early cognitive declination.
Living with dementia: These activities were performed by carers to manage the day-to-day living with dementia and included the following four actions: (1) carers keeping themselves and care recipients physically well (such as monitoring of health status, acquiring information about nutrition, and staying active); (2) carers using health and social support services for themselves and care recipients; (3) carers managing care recipients’ medications; and (4) carers planning for care recipients’ future.
Psychosocial wellbeing: Activities grouped in this category were actions that carers performed to manage their caregiving role, to maintain their relationship with the care recipient and their own and the care recipient’s emotional wellbeing. These included the following five actions: (1) carers maintaining their and care recipients’ psychological wellbeing; (2) carers managing their relationship with care recipients; (3) carers maintaining their social relations, the care recipients’, and as a couple; (4) carers understanding the caring role; (5) carers engaging themselves and care recipients in enjoyable activities.
Carer Characteristics and Skills
The included publications described nine personal characteristics and skills required by carers for successful self-management. These included: (1) being positive; (2) problem solving; (3) being self-aware; (4) tailoring information; (5) goal setting; (6) making decisions; (7) being confident; (8) having an ability to cope; and (9) sustaining behavior changes that facilitate care of the recipients.
Theoretical and Conceptual Frameworks
The theoretical and conceptual frameworks that guided the descriptions of self-management of dementia by carers in the included publications are listed in Table 3. Six publications referred to Bandura’s (1986, 1997) Social Cognitive Theory, four of which also included the Theory of Stress and Coping by Lazarus and Folkman (1984). Twelve publications were underpinned by five models of self-management of chronic conditions. Four publications used a model of self-management of dementia by people in early stages. There was no conceptual framework described about self-management of dementia by carers.
Instruments Used to Measure Self-Management of Dementia by Carers.
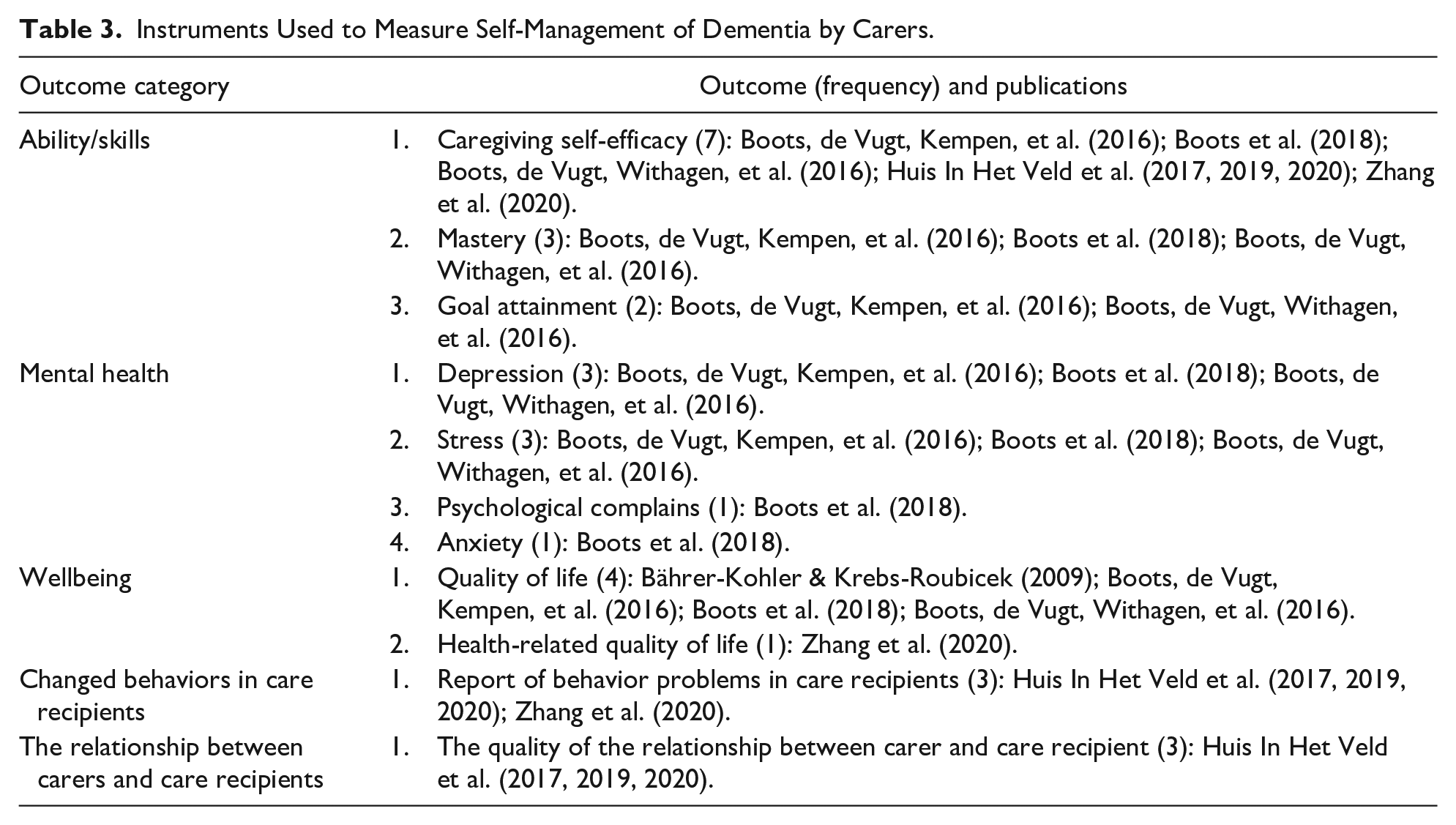
Measures
Table 3 summarizes the measures used in the included publications. Nine publications conducted quantitative studies and eight described several measures of self-management of dementia by carers. The most frequently used measures focused on carers’ abilities and skills mainly caregiving self-efficacy (n = 7/8). Others included carers’ wellbeing (n = 5/8), changed behaviors in care recipients (n = 4/8), and carer’s mental health (n = 3/8), and the relationship between carers and care recipients (n = 3/8).
Discussion
Psychosocial interventions aimed to support the skills and capacity of self-management of dementia are increasingly offered to carers (Huis In Het Veld et al., 2015). However, the components of self-management of dementia by carers are not well described in the literature, hence poorly applied. Further, the effectiveness of these interventions is measured using various instruments that may not necessarily be relevant to self-management (Mountain, 2017). Research has also shown that the effectiveness of these interventions was not consistent or conclusive (Mountain, 2017; Nolte & Osborne, 2013). Addressing these issues is important to better support carers self-manage dementia. This review addresses this gap and adds new knowledge in that it clarifies the constituents of this type of self-management and advances the development of this concept.
The included studies were mostly (n = 13/16) conducted in countries such as the Netherlands, Switzerland, and Finland with maximum sample size of 81 carers, which clearly indicates that more studies with bigger samples in other parts of the world are warranted. The publications originated from various disciplines which shows the importance of self-management of dementia by carers for various healthcare providers. This review demonstrates that self-management of dementia by carers is incipient as most of the included publications were published since 2015 and were either protocols for psychoeducational interventions, feasibility studies, qualitative reports, or discussions.
An exhaustive search of the literature revealed 22 components of self-management of dementia by carers. These components were categorized into three types of activities, and carer characteristics and skills. The identified activities related to dementia, day-to-day living with the dementia, and psychosocial wellbeing. The dementia related activities were those performed by carers for their care recipients. While the day-to-day living with dementia and the psychological wellbeing activities described actions performed by carers that focused on themselves as well as their care recipients. One of the psychosocial wellbeing activities, carers maintaining social relations, addressed the couplehood (i.e., the togetherness) of carers, and their care recipients. No single publication in this review described all the components, and many missed describing most of the activities. Moreover, the carer characteristics and skills were infrequently described. Given the limited studies that capture self-manage dementia by carers on behalf of person with dementia, and the fragmented approached within existing studies, conceptualization could be further enhanced with targeted studies about the experiences of carers and healthcare providers. The findings from this review highlight the limitations of the existing approaches examined in studies to help carers and healthcare providers, and the areas to be focused on in future endeavors.
Different theoretical and conceptual frameworks guided the descriptions of self-management of dementia by carers. Most descriptions were guided by general models of self-management. Some recent publications based their descriptions on a model of self-management of dementia by people diagnosed with it in early stage (n = 4/16). It is interesting to note that even when this framework was used, the components were not comprehensive. For instance, a meta-review that used this model did not describe most of the day-to-day living with dementia activities, such as carers keeping themselves and care recipients physically well, and some of the psychosocial activities, such as understanding the caring role, were not identified (Huis In Het Veld et al., 2015). Nor were any of the carer characteristics and skills described (Huis In Het Veld et al., 2015). As theoretical and conceptual frameworks should align with the components of the concept clearly (Serlachius & Sutton, 2009), the development of a conceptual framework that aligns with the components identified in this review is required.
Eight of the included nine quantitative studies described measures of self-management of dementia by carers. The most frequently described were abilities and skills related to caregiving self-efficacy (n = 7/8) and quality of life (n = 4/8), which are distal measures of self-management (Nolte & Osborne, 2013). Using distal measures to determine the effectiveness of self-management support interventions can lead to inconsistent findings (Nolte & Osborne, 2013). Changes in self-efficacy and the quality of life are subjective and require time to develop. Proximal measures, such as the scores on a knowledge test, and intermediate measures, such as evaluating self-management capability, are considered less subjective and more likely to produce conclusive results (Nolte & Osborne, 2013). This review found that most measures were not focused on the components of self-management of dementia by carers, whilst tools that measure the components of self-management of other chronic condition are available. For example, self-management of asthma, mental conditions, and diabetes (Bursch et al., 1999; Coulombe et al., 2015; Modi et al., 2010; Schmitt et al., 2013). The development of a measure which is more objective and related to the capability of self-management of dementia by carers as described by this review would seem an appropriate future research focus (Mountain, 2017).
The included publications provided descriptions that were based on differing stages of dementia. Six included all stages, four only the early stage, and one the late stage. Five publications did not describe the stage of dementia. In the early stage, the person with dementia has the capacity to be more involved in self-management activities (Mountain, 2006; Mountain & Craig, 2012). However, this changes as the disease progresses and tasks of self-management become increasingly the responsibility of carers (Huis In Het Veld et al., 2015). Carers also report increased levels of burden and lower levels of mental health as dementia progresses (Farina et al., 2017; Martins Gratao et al., 2010; Wawrziczny et al., 2017). Further validation of self-management of dementia by carers is required by examining the perceptions of people with dementia across all stages, carers, and healthcare providers. This will lead to a more comprehensive and universal understanding.
The findings of this review provide a thorough delineation and a deep understanding of the unique and complex nature of self-management of dementia by carers. This will help healthcare providers develop, administer, and evaluate relevant and comprehensive self-management support interventions for carers (Lucero et al., 2019; Mountain, 2017). These interventions will enable carers to effectively cope with their role and provide better care for people with dementia (Huis In Het Veld et al., 2015; Laakkonen et al., 2016; Van Het Bolscher-Niehuis et al., 2016). Having a self-management paradigm specific for carers is also essential to guide research and policies in this field (Mountain, 2017).
Limitations
The findings may be limited by including publications in English language only. Many publications were excluded because they focused on self-efficacy or the person with dementia. Only the publications that provided clear descriptions were included which may have limited the findings. However, this was justified given that this review aimed to clarify self-management of dementia by carers. This review did not explore the characteristics of self-management in different stages of dementia.
Conclusion
Self-management of dementia by carers was clarified by synthesizing the descriptions of its characteristics from the included publications. These publications highlight the intricate and complex nature of self-management of dementia by carers. This review demonstrates that self-management of dementia by the carers involves three types of activities and personal qualities. The activities mainly describe the carer self-managing for the care recipient. They also include the carer focusing on themselves and the carer-care recipient couple. This review found the fragmented approaches in helping carers given that no single publication included all components and the explanation for these components was based on many theoretical and conceptual frameworks. Self-management of dementia by carers was measured frequently by the distal measures of self-efficacy or quality of life and not of the described components. Further, research is required to validate these findings from the experiences of care recipients, carers, and healthcare providers.
Supplemental Material
sj-pdf-1-ggm-10.1177_23337214211016694 – Supplemental material for Self-Management of Dementia by Family Carers: A Scoping Review
Supplemental material, sj-pdf-1-ggm-10.1177_23337214211016694 for Self-Management of Dementia by Family Carers: A Scoping Review by Anas Shehadeh, Sharyn Hunter and Sarah Jeong in Gerontology and Geriatric Medicine
Supplemental Material
sj-pdf-2-ggm-10.1177_23337214211016694 – Supplemental material for Self-Management of Dementia by Family Carers: A Scoping Review
Supplemental material, sj-pdf-2-ggm-10.1177_23337214211016694 for Self-Management of Dementia by Family Carers: A Scoping Review by Anas Shehadeh, Sharyn Hunter and Sarah Jeong in Gerontology and Geriatric Medicine
Supplemental Material
sj-pdf-3-ggm-10.1177_23337214211016694 – Supplemental material for Self-Management of Dementia by Family Carers: A Scoping Review
Supplemental material, sj-pdf-3-ggm-10.1177_23337214211016694 for Self-Management of Dementia by Family Carers: A Scoping Review by Anas Shehadeh, Sharyn Hunter and Sarah Jeong in Gerontology and Geriatric Medicine
Supplemental Material
sj-pdf-4-ggm-10.1177_23337214211016694 – Supplemental material for Self-Management of Dementia by Family Carers: A Scoping Review
Supplemental material, sj-pdf-4-ggm-10.1177_23337214211016694 for Self-Management of Dementia by Family Carers: A Scoping Review by Anas Shehadeh, Sharyn Hunter and Sarah Jeong in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
We would like to thank the funding body and the librarian for their support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The University of Newcastle International Postgraduate Research Scholarship. The funding body has no role in the design of the study, collection, analysis or interpretation of data, and in writing the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.