
Abstract
Introduction
Most people with dementia live in their own homes and rely on assistance to manage activities of daily living (ADL) from family and friends (carers; Australian Institute of Health and Welfare, 2012; National Alliance for Caregiving and AARP, 2009). Assistance is commonly required to support personal ADLs (e.g., washing, dressing, grooming, toileting, eating) and instrumental ADLs (e.g., cooking, shopping, and managing finances and health care) as well as providing general surveillance to ensure the safety and well-being of the person with dementia (Alzheimer’s Disease International, 2009). A review of studies that provided information on caregiving reported that carers spent an average of 3.7 hr per day assisting with ADLs and additional time spent providing supervision (Wimo, Winblad, & Jonsson, 2007).
Although caring for someone with dementia can be rewarding, it is also challenging (Thompson, 2013) and associated with high levels of burden (Adelman, Tmanova, Delgado, Dion, & Lachs, 2014), depression (Clare et al., 2002), and reduced quality of life (Argimon, Limon, Vila, & Cabezas, 2004). Carers have reported that they want more education, skills counseling, emotional support, and respite to help them in their caring role (Black et al., 2013; Hughes et al., 2014). There are now many trials demonstrating the efficacy of nonpharmacological interventions where the interventionist predominantly works with the carer with the aim of supporting them to provide care and cope more effectively (Brodaty & Arasaratnam, 2012; Elvish, Lever, Johnstone, Cawley, & Keady, 2013; Gallagher-Thompson et al., 2012; Jones, Edwards, & Hounsome, 2012; Kales, Gitlin, & Lyketsos, 2015; Maslow, 2012; Olazarán et al., 2010; Schoenmakers, Buntinx, & DeLepeleire, 2010; Van’t Leven et al., 2013). Interventions for carers are often multicomponent and tend to involve a combination of education, support, problem solving, and skills training (Kales et al., 2015). Although carer interventions are widely considered to be effective, studies are heterogeneous and involve different participant groups, interventions, comparison conditions, and outcomes. This leads to difficulty in interpreting the evidence and ascertaining which interventions are most effective and should be translated into clinical practice.
One of the distinctions between caregiver intervention programs is whether they work with the person with dementia and carer (dyad) or whether they focus the intervention on the carer alone. A number of the interventions that have been tested are considered dyadic interventions (Van’t Leven et al., 2013). Dyadic interventions may include joint counseling, problem solving, and use of strategies to try and increase independence in ADL and engagement in meaningful activities. Working with the dyad is thought to be more effective because of the synergistic relationship between the person with dementia and the caregiver. Existing systematic reviews have examined the effect of one type of carer intervention or the effect of carer interventions more broadly on a single outcome (Brodaty & Arasaratnam, 2012; Kales et al., 2015; Maslow, 2012).
The aim of this article was to examine the efficacy of carer interventions that involve multiple components (e.g., education, problem solving, skills building, support) and compare effects based on whether or not they were dyadic in nature.
Method
Background to the Review
This review stemmed from work that was completed in the development of clinical practice guidelines for dementia in Australia (Guideline Adaptation Committee, 2016). Clinical practice guidelines should include the most recent literature and be developed in a way that is timely and resource efficient while maintaining methodological quality of the systematic reviews (World Health Organisation, 2012). To manage this, guidelines typically use existing systematic reviews as a source of primary studies and update these reviews with more recent studies where required (Woolf, Schunemann, Eccles, Grimshaw, & Shekelle, 2012). As a component of guideline development, we conducted a systematic review of the efficacy of interventions for carers of people with dementia in comparison with usual care. We identified the most recent, comprehensive, high quality systematic review and used this as a source of primary studies (Olazarán et al., 2010). We then updated this by identifying any newer studies meeting the inclusion criteria and combined all results to present an overall measure of efficacy. This work is available in the Guideline Technical Report (Guideline Adaptation Committee, 2016). Subsequent to development of the guideline, we have examined the effectiveness of multicomponent interventions that were dyadic in nature in comparison with those that were not. We have updated the searches conducted during the guideline development work, included new studies, completed additional data extraction, and conducted novel meta-analyses.
Inclusion Criteria
We included randomized controlled trials published in English. Participants in the included studies were carers of people with any type of dementia. Multicomponent interventions were defined as those that involved a number of different intervention techniques. These intervention techniques included, but were not limited to, education, counseling, information regarding services, enhancing carer skills to provide care, problem solving and strategy development, and increasing resilience and coping skills in the carer. Interventions that were conducted with the carer alone or those that also involved the person with dementia (dyad) were included. Studies were required to compare the intervention with usual care. We also searched for studies that directly compared carer focused with dyadic interventions. The outcomes included were those measuring direct impact for the carer (depression, quality of life, and carer burden and caregiver upset in relation to behavioral and psychological symptoms of dementia) and the person with dementia (ADL function, behavioral and psychological symptoms of dementia).
Search Method
We identified the most recent and comprehensive high quality systematic review. The review was updated by searching for additional randomized controlled trials published after September 2008. Databases searched were Health Technology Assessment, the Cochrane Library (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effects), Medline, EMBASE, PsycINFO, and PubMed using terms including Alzheimer’s, dementia, caregiver, carer, family, assess, treatment, therapy, intervention, support, psychosocial, nonpharmacologic, education (see the appendix for full search strategy). Searches for the guideline were conducted on May 9, 2014, and updated on October 7, 2015.
Data Collection and Analysis
One review author (K.L.) ran the searches and reviewed titles and abstracts to select articles for full text review. Two authors (K.L. and R.M.) conducted full text review to determine which studies met the criteria for inclusion in the review. One author (K.L.) extracted data into the tables and into RevMan Version 5.2 for analysis and a second person checked the data extraction accuracy. Two authors (K.L. and R.M.) independently completed an assessment of risk of bias using the Cochrane Collaboration Risk of Bias tool (Higgins & Green, 2011). This included assessment of (a) random sequence generation, (b) allocation concealment, (c) blinding of participants and personnel, (d) blinding of outcome assessment, (e) incomplete outcome data, and (f) selective reporting. Items were classified as being “low risk,” “high risk,” or “unclear risk of bias.” We did not contact authors to obtain missing information regarding study data or methods.
Study outcomes were pooled in a meta-analysis in RevMan Version 5.2 when means and standard deviations were reported or could be calculated. Where authors did not report means and standard deviations (or these could not be calculated based on the data provided) studies were described narratively. A random effects model was used for pooling all outcomes due to statistical heterogeneity (I2 ≥ 50) and obvious heterogeneity observed on forest plot. Where it was not possible to pool data for an outcome (due to data not presented in an appropriate form for use in meta-analysis) the study results were synthesized in a narrative summary.
Results
The study selection process is presented in Figure 1.
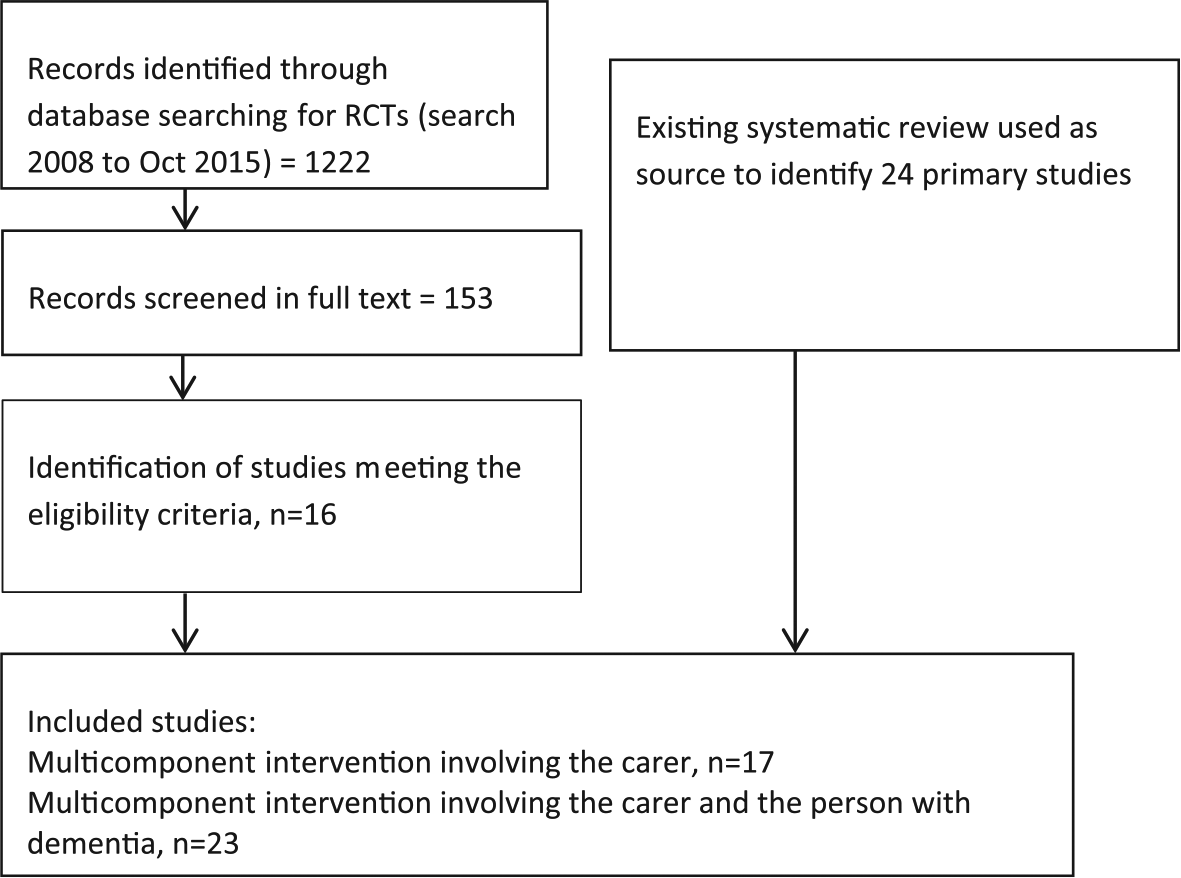
Search for studies.
The most recent high quality systematic review was conducted by Olazarán and colleagues in 2010 (Olazarán et al., 2010). This review included all forms of carer interventions and did not exclude studies based on outcomes reported. The review included six multicomponent interventions involving the carer and 18 multicomponent interventions involving the carer and the person with dementia. The review included studies published up to 2008.
We searched for additional studies published from 2008 to October 2015; 11 studies of multicomponent interventions involving only the carer and five multicomponent dyad interventions were identified. Thus, the total number of studies included in the review was 40. We did not identify any studies that compared carer focused interventions with dyadic interventions. Characteristics of included studies are summarized in Table 1.
Characteristics of Included Studies.

Note. Populations were categorized based on severity. The mean MMSE (or similar) was used where MMSE 19 to 23 was considered mild and MMSE 10 to 18 was considered moderate. REACH = Resources for Enhancing Alzheimer’s Caregiver Health; BPSD = behavioral and psychological symptoms of dementia; PWD = person with dementia; AD = Alzheimer’s disease; CG = caregiver education; NPI-Q = Neuropsychiatric Inventory–Questionnaire; OT = occupational therapist; ADL = activities of daily living; DAISY = Danish Alzheimer Intervention Study; MMSE = Mini-Mental State Examination; CTIS = Computer-Telephone Integration System; FITT-D = Family Intervention: Telephone Tracking–Dementia; FITT-NH = Family Intervention: Telephone Tracking–Nursing Home; CD = compact disc; CDR = Clinical Dementia Rating; PLST = progressively lowered stress threshold; IADL = instrumental activities of daily living; COPE = care of persons with dementia in their environments aRisk of bias: (a) random sequence generation, (b) allocation concealment, (c) blinding of participants and personnel, (d) blinding of outcome assessment, (e) incomplete outcome data, (f) selective reporting.
Summary of Included Studies
The characteristics of carers were similar across all studies. Studies typically recruited more females than males; in most studies, approximately, two thirds of the caregivers were female. Caregivers were typically aged in their 60s and 70s. The severity of symptoms in people with dementia varied widely across studies although most participants had mild to moderate dementia as indicated by Mini-Mental State Examination scores. A summary of the different interventions provided, the follow-up time for the studies, and the outcomes contributing to this review is shown in Table 1. In the dyadic interventions, the person with dementia was involved in various activities including education about dementia, joint problem solving, joint counseling, cognitive stimulation, engagement in pleasant activities, modification of the environment or tasks, peer support, and general case management duties.
Methodological Quality of the Included Studies
Overall, the quality of included studies was considered moderate as presented in Table 1. Due to unclear reporting, it was often difficult to determine methods of randomization and allocation concealment. Few studies had published protocols or were registered on clinical trial registries making it difficult to determine the presence of selective reporting. Four studies appeared to use outcome assessors who were not blinded to allocation, and in a further 16 studies it was unclear as to whether the outcome assessor was aware of allocation.
Impact on the carer’s depressive symptoms
Carer only interventions
Multicomponent interventions involving only the carer tended to reduce depressive symptoms although this was of borderline statistical significance (standardized mean difference [SMD] = −0.18, 95% confidence interval [CI] = [−0.37, 0.00], 12 trials, N = 1,527 participants). Two studies could not be included in the meta-analysis; one of these studies reported no effect on depression following treatment (Finkel et al., 2007), whereas the other study reported that carers receiving the intervention had decreased risk of depression (odds ratio = 0.15, confidence interval = [0.04, 0.65], p < .013; Kuo et al., 2013).
Dyadic interventions
Multicomponent interventions involving both the carer and the person with dementia significantly reduced depressive symptoms (Figure 2; SMD = −0.33, 95% CI = [−0.62, −0.04]; seven studies, N = 663). Four studies did not provide data that could be included in the meta-analysis. One of these studies reported no significant effect associated with intervention (Chu, Edwards, Levin, & Thompson, 2000), whereas the other three studies reported a statistically significant improvement in depressive symptoms as a result of the intervention. Buckwalter and colleagues found that those in the intervention group were significantly less depressed than caregivers receiving usual care at 6 months (p = .0007), but outcome at 12 months did not reach statistical significance (Buckwalter et al., 1999). Two other studies reported an improvement in depressive symptoms as a result of the intervention (Gitlin, Winter, Dennis, Hodgson, & Hauck, 2010; Logsdon et al., 2010), with Gitlin and colleagues reporting that 53% of carers in the intervention group reported depressive symptoms versus 68% in the control group (p = .02). There was no statistically significant difference between carer only interventions and dyadic interventions (p = .41).
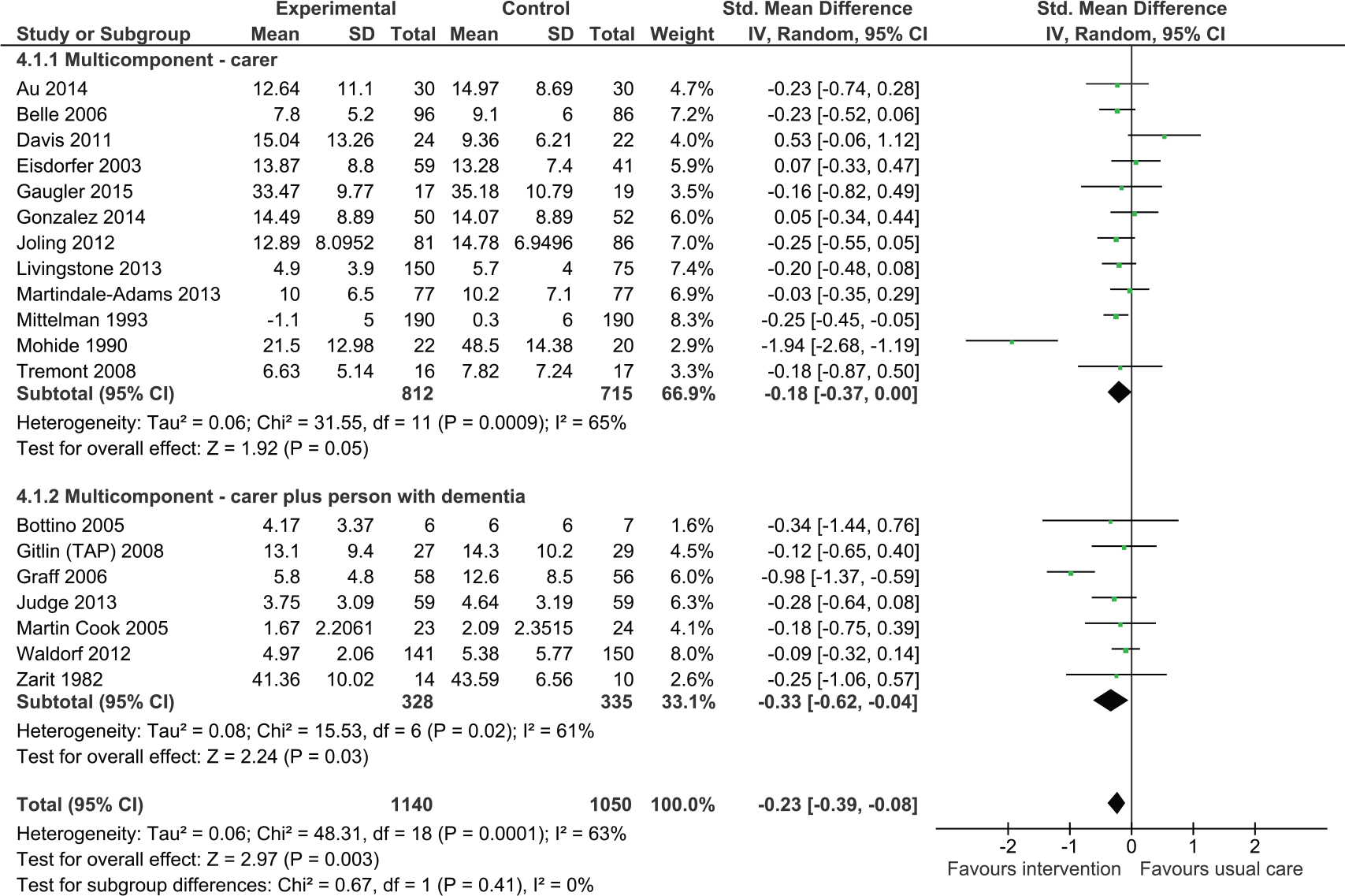
Multicomponent intervention versus usual care: Effect on depression postintervention.
Impact on the carer’s quality of life
Carer only interventions
Although the overall effect on quality of life was not statistically significant, there was a trend in favor of intervention (SMD = 0.14, 95% CI = [−0.06, 0.34], three studies, N = 412). One study that did not report data suitable for contributing to the meta-analysis found no significant improvements in quality of life of carers postintervention (Davis, Tremont, Bishop, & Fortinsky, 2011).
Dyadic interventions
Analysis revealed a trend toward improved quality of life associated with intervention (Figure 3); however, the confidence intervals were wide and the effect was not statistically significant (SMD = 0.32, 95% CI = [−0.04, 0.68], four studies, N = 589). A study conducted by Logsdon and colleagues could not be included in the analysis; this study found no significant differences between treatment and control groups in quality of life (Logsdon et al., 2010).
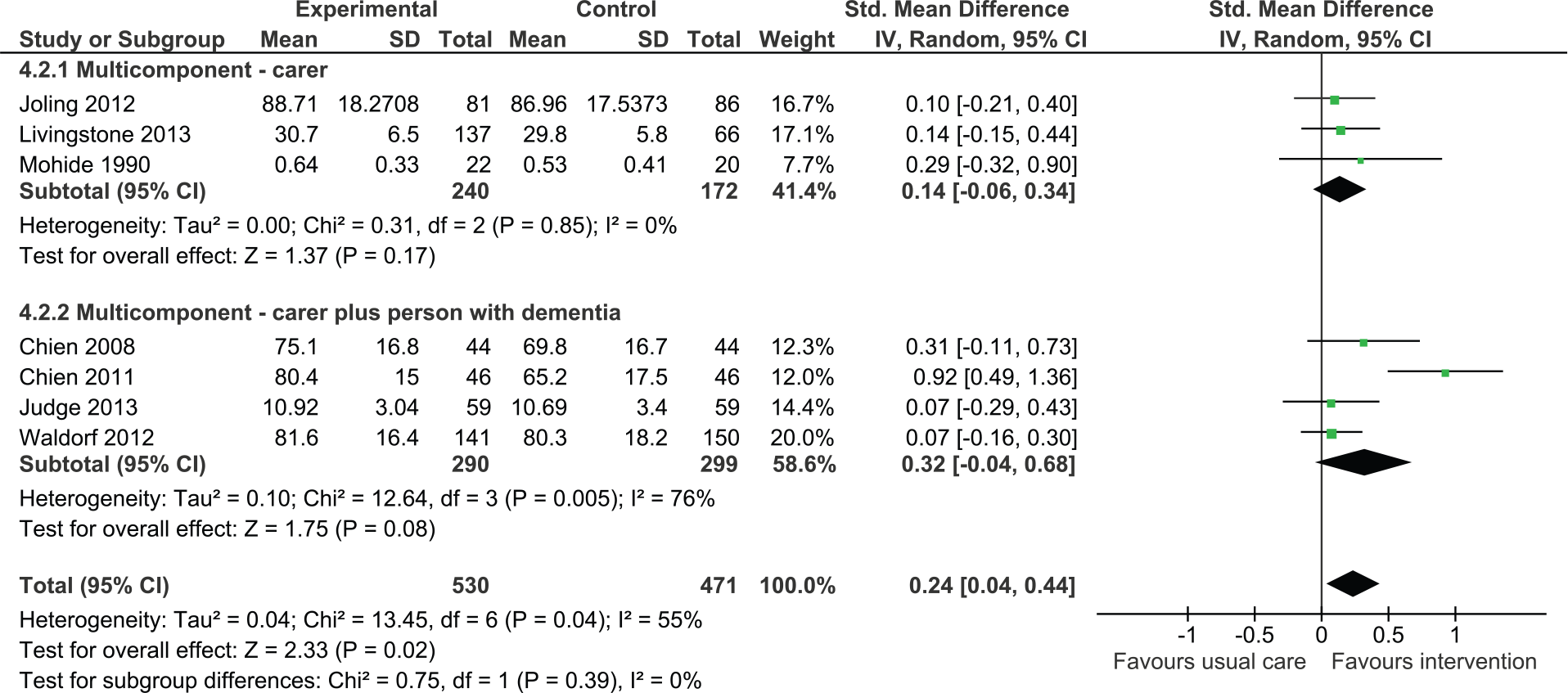
Multicomponent interventions versus usual care: Effect on quality of life postintervention.
When considering all multicomponent interventions (carer only plus dyadic), the analysis demonstrated an overall positive effect (SMD = 0.24, 95% CI = [0.04, 0.44]). There was no statistically significant difference between carer only interventions and dyadic interventions (p = .39).
Impact on level of carer burden
Carer only interventions
The analysis found there was no significant effect on carer burden (Figure 4, SMD = −0.10, 95% CI = [−0.40, 0.20], six studies, N = 497). A study conducted by Logsdon and colleagues, which could not be included in the analysis, similarly found no significant reduction in levels of burden (Logsdon et al., 2010).
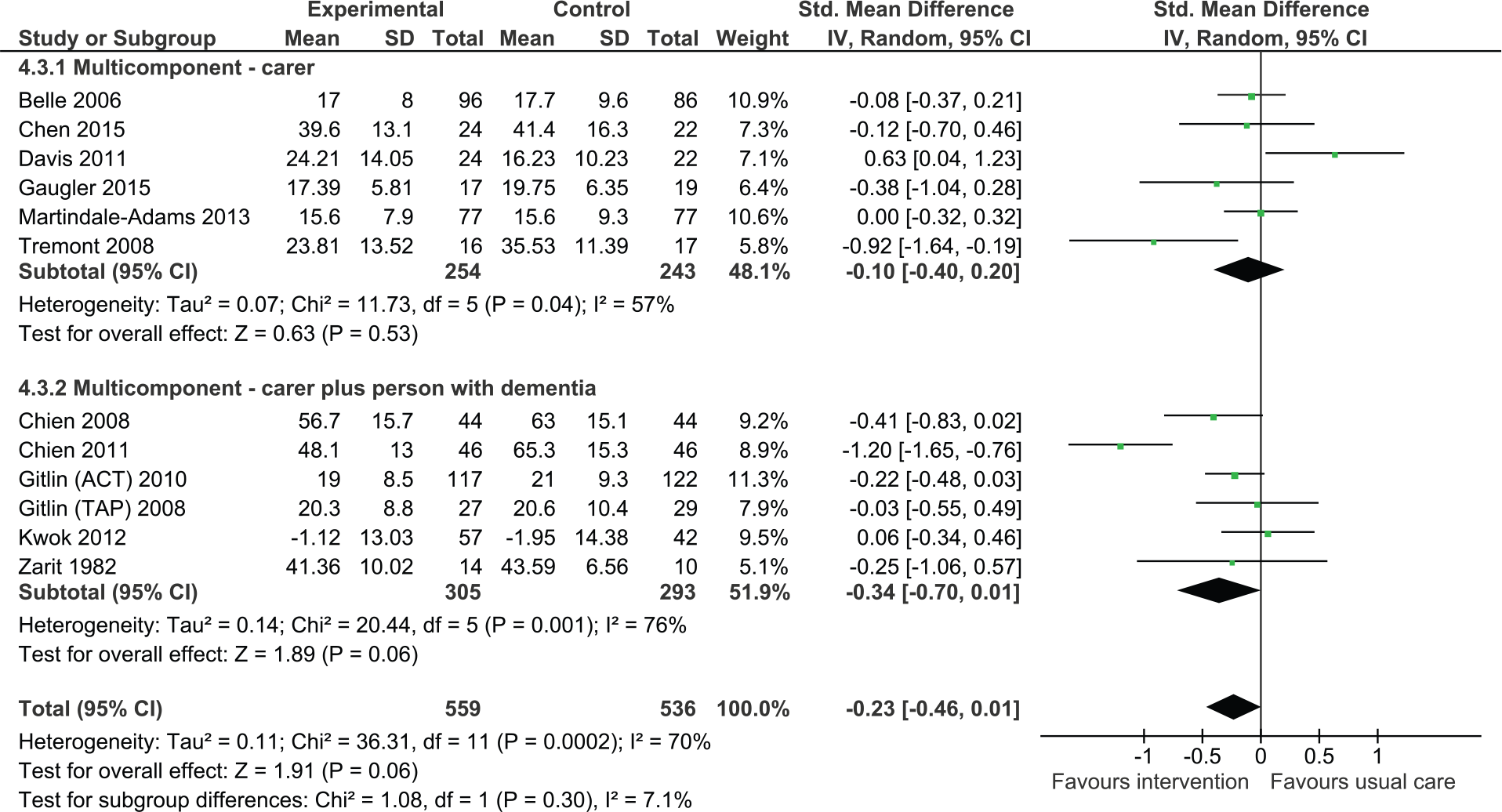
Multicomponent interventions versus usual care: Effect on carer burden postintervention.
Dyadic interventions
Six studies were pooled to examine the efficacy of dyadic training on carer burden. The result was statistically not significant due to wide confidence intervals. However, there was a strong trend suggesting efficacy of intervention (SMD = −0.34, 95% CI = [−0.70, 0.01], six studies, N = 598). One study that could not be included in the analysis found that following intervention there was a significant reduction in carer burden in the intervention group relative to those in the control group. However, at 6 months, there were no differences between groups (Chu et al., 2000). There was no statistically significant difference between carer only interventions and dyadic interventions (p = .30).
Impact on behavioral and psychological symptoms of dementia
Carer only interventions
We pooled three studies evaluating the effects of intervention on behavioral and psychological symptoms of dementia measured using a tool such as the Neuropsychiatric Inventory or the Revised Memory and Behavior Problem Checklist (Figure 5). Overall, the effect was not significant although the analysis suggested positive effects on intervention (SMD = −0.41, 95% CI = [−0.85, 0.03], three studies, N = 317).
Multicomponent interventions versus usual care: Effect on behavioral and psychological symptoms of dementia postintervention.
Dyadic interventions
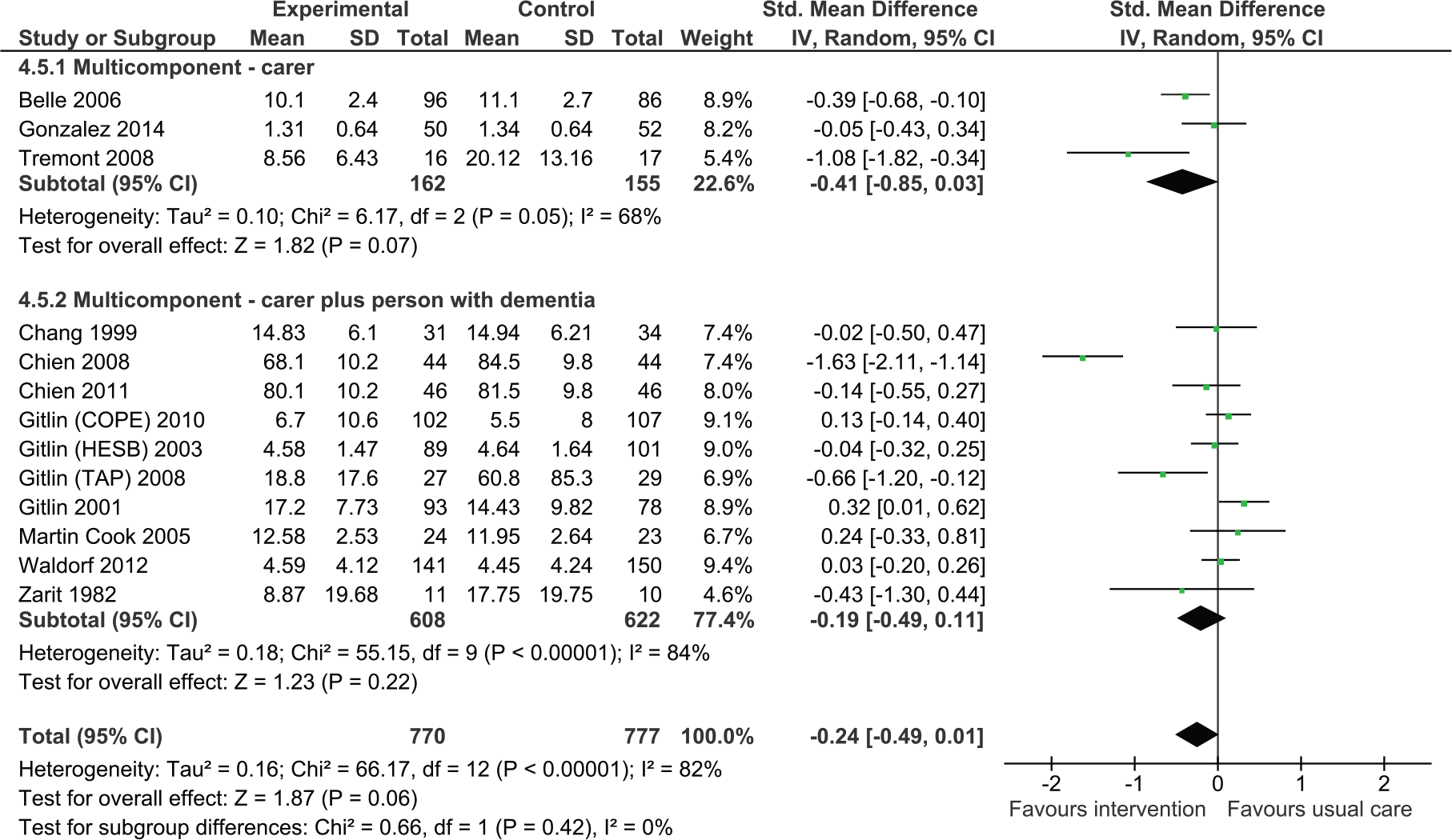
We also found that dyadic interventions appeared to be beneficial. However, the results were statistically not significant (SMD = −0.19, 95% CI = [−0.49, 0.11], 10 studies, N = 1,230).
Overall, the meta-analysis suggested a reduction in behavioral and psychological symptoms of dementia (SMD = −0.24, 95% CI = [−0.49, 0.01]). There was no statistically significant difference between carer only interventions and dyadic interventions (p = .42).
Impact on caregiver upset with behavioral and psychological symptoms of dementia
Fewer studies examined caregiver reaction or upset with symptoms. Overall, we found that multicomponent interventions were effective in reducing caregiver reaction or upset (Figure 6, SMD = −0.26, 95% CI = [−0.42, −0.10], seven studies, 867 participants). The statistical heterogeneity in the analysis was lower than in the other analyses (I2 = 21%).
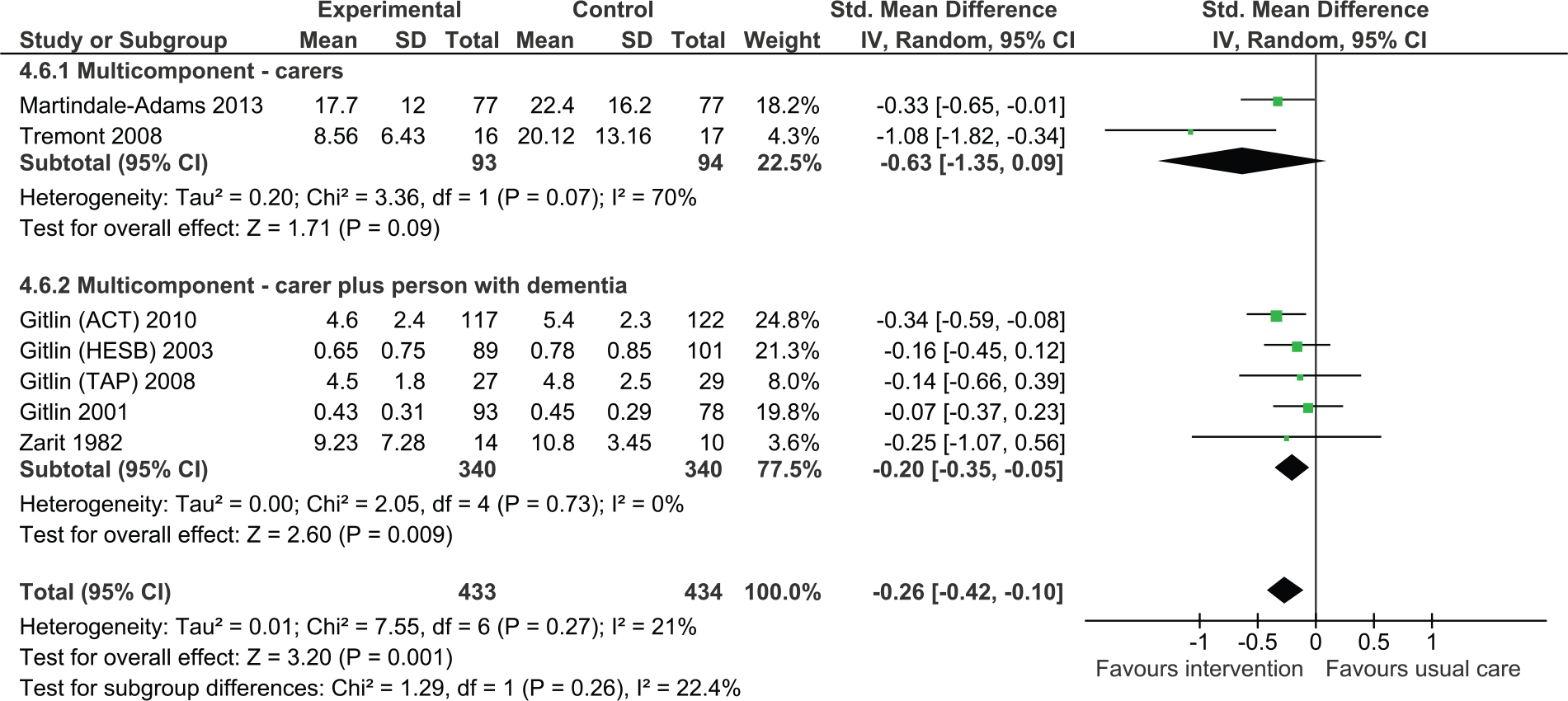
Multicomponent interventions versus usual care: Effect on caregiver upset with behavioral and psychological symptoms of dementia postintervention.
Impact on independence in ADL
Nine studies reported outcomes for ADL in the person with dementia of which eight were dyadic in nature. Overall, the effect was not significant although the direction of effect was positive (Figure 7, SMD = 0.17, 95% CI = [−0.15, 0.57], N = 1,465).
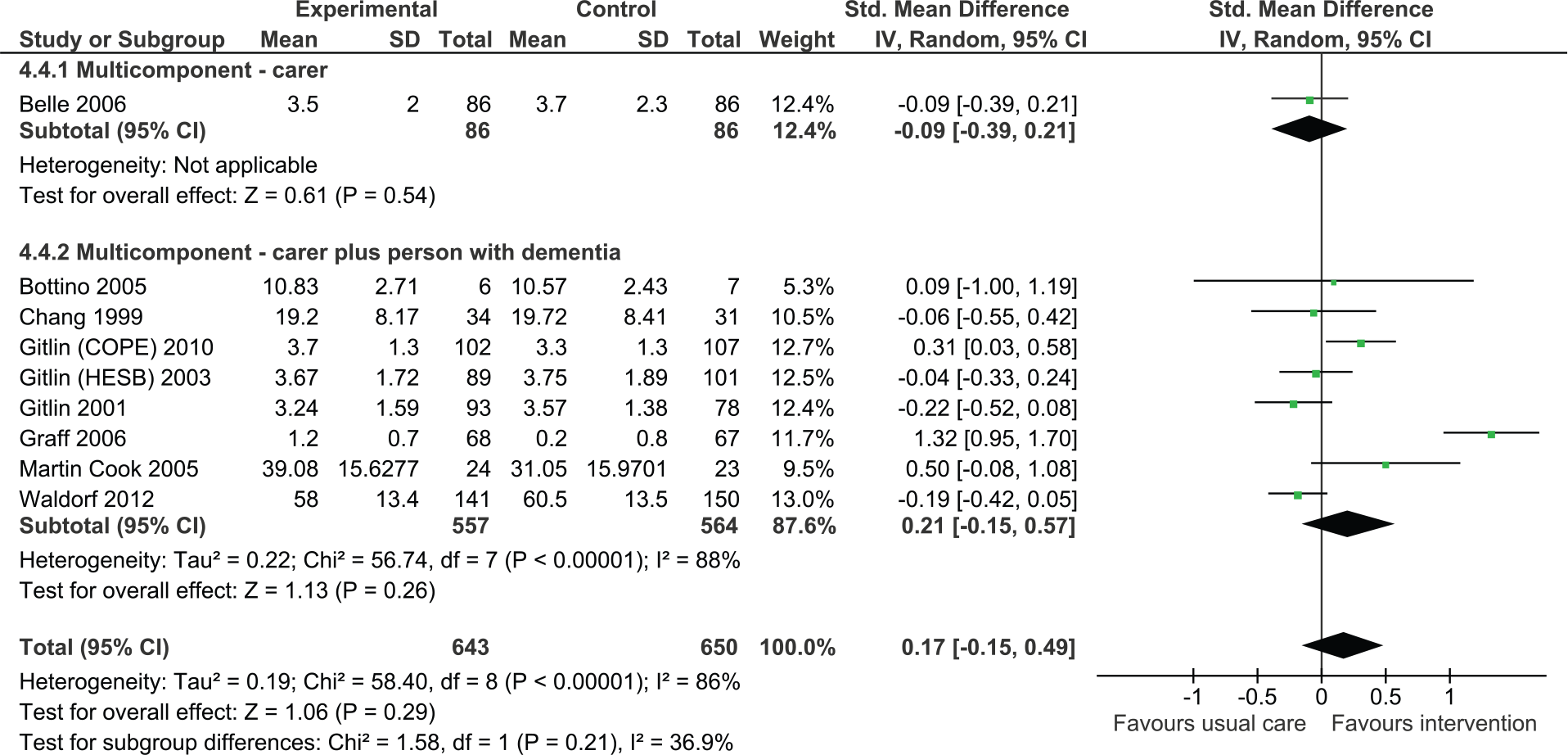
Multicomponent interventions versus usual care: Effect on activities of daily living postintervention.
Effect of interventions based on the severity of symptoms of the person with dementia
There were too few studies to further compare the effect of carer focused and dyadic interventions based on the severity of the symptoms in the person with dementia. However, we did conduct sensitivity analyses to examine whether severity of symptoms was a moderator of effect of caregiver interventions for each outcome. Results are presented in Table 2. It can be seen that studies involving people with milder severity symptoms of dementia appeared to be more effective in reducing levels of depression and burden in carers. Whereas, studies involving people with moderate to severe symptoms of dementia appeared to be more effective in improving the quality of life of the carer.
Effect of Interventions for Carers on Different Outcomes Based on the Severity of Symptoms of the PWD.
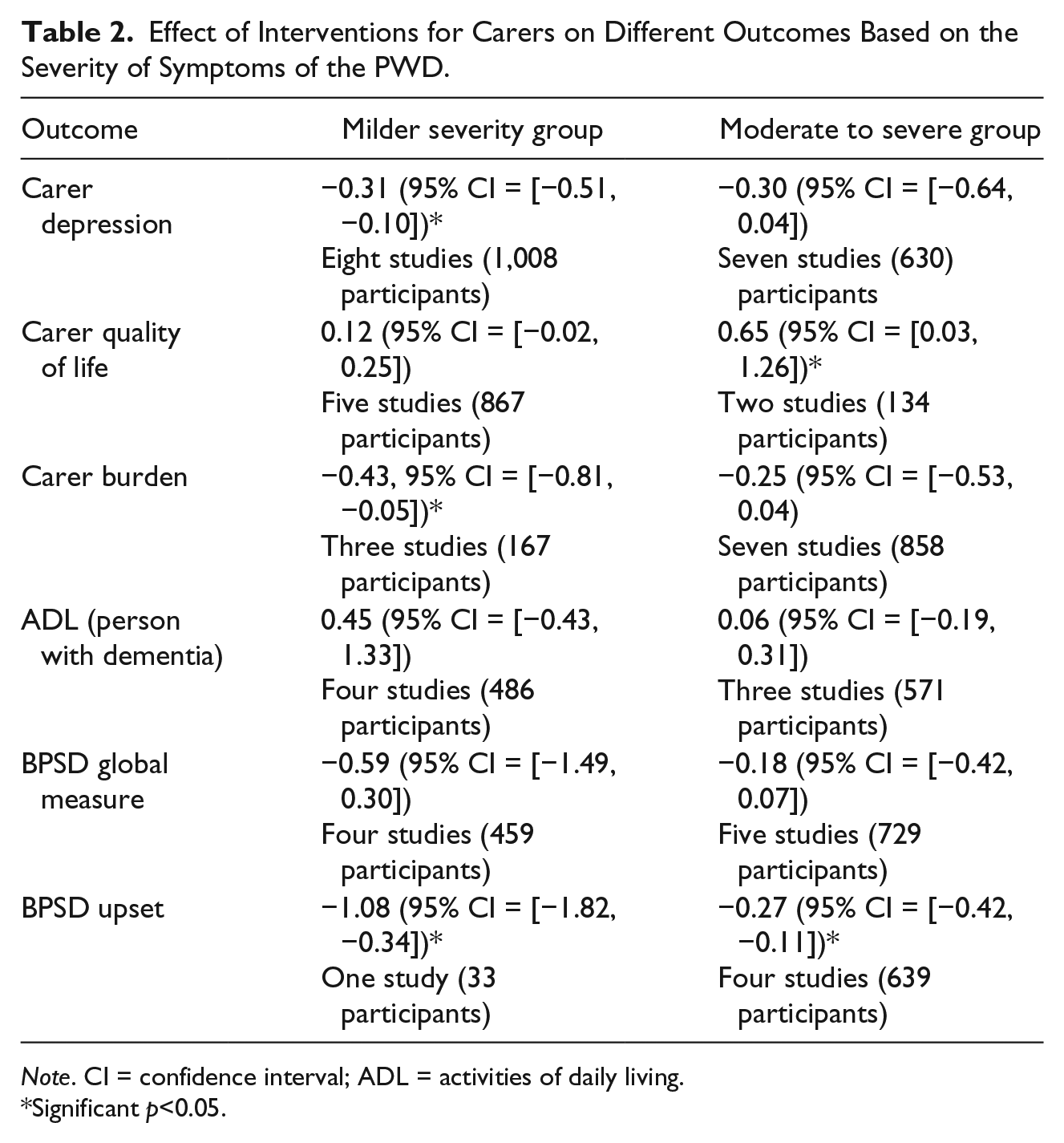
Note. CI = confidence interval; ADL = activities of daily living.
Significant p<0.05.
Discussion
Family members and friends (informal carers) play an important role in the day-to-day assistance and support of people with dementia. Informal carers typically have poorer outcomes in terms of well-being, depression, quality of life, health status, and use of health care resources (Argimon et al., 2004; Bremer et al., 2015; Spector, Orrell, Charlesworth, & Marston, 2015). This review included 40 studies evaluating multicomponent interventions for carers of people with dementia. Meta-analysis demonstrated that multicomponent interventions can reduce caregiver depressive symptoms, decrease burden, reduce caregiver’s upset with symptoms of dementia and improve the caregiver’s quality of life. Multicomponent interventions can also reduce behavioral and psychological symptoms of dementia, and our analyses suggested beneficial effects in terms of delaying functional decline although some interventions did this more effectively than others.
There were no statistically significant differences between the effects of carer focused interventions and dyadic interventions for any of the outcomes although inspection of the forest plots suggests that dyadic interventions appeared to reduce carer burden to a greater extent. Furthermore, studies evaluating carer focused interventions rarely collected outcome measures relating to the functional independence of the person with dementia, suggesting that this is not one of the aims of treatment. Qualitative research has found that the quality of the relationship between the person with dementia and the carer depends not only on the presence of depression or anxiety in the carer, but also the presence of depression, irritability, behavioral disturbances, and quality of life status of the person with dementia, emphasizing the need for interventions targeting both parties to improve mood and quality of life (Spector et al., 2015). Given the interdependent nature of the health and quality of life of people with dementia and their family members, it is plausible that providing multicomponent interventions that target the dyad, rather than just the caregiver or person with dementia themselves, would be more effective. We did not identify any studies that directly compared carer focused with dyadic interventions. Studies to compare direct differences between carer focused interventions and dyadic interventions are required.
We also examined whether effects varied based on the severity of symptoms of the people with dementia included in the population. Studies were categorized rather arbitrarily based on the average Mini-Mental State Examination score of participants, which provided an overall reflection of the study group. The analyses suggest that there is more potential to reduce depressive symptoms and carer burden when the person has milder severity dementia. Interestingly, there appeared to be more capacity to improve the carer’s quality of life when the person with dementia had moderate to severe symptoms. Quality of life is difficult to change through intervention. It may be that carer quality of life quickly deteriorates when the symptoms of dementia change from mild to moderate/severe and so there is more potential to make a difference at this point. Caution should be applied in interpreting these findings because of the relatively small number of studies involved in the analyses.
This review supports the findings of other reviews of caregiver interventions (Brodaty & Arasaratnam, 2012; Olazarán et al., 2010; Van’t Leven et al., 2013) but adds to the body of literature by examining effect on a number of outcomes, including meta-analysis and comparing different forms of multicomponent interventions. The effect sizes found for all outcomes are considered small (Cohen, 1992). However, living with dementia and providing care for someone with dementia is challenging; hence, even small improvements may be considered clinically significant. This is particularly important in dementia care where there are few effective treatments for the person with dementia.
The total worldwide cost of dementia in 2015 was US$818 billion and this is projected to rise (Prince et al., 2015). This estimate reflects direct medical costs (approx. 20% of global costs), direct social care costs (approx. 40%), and the costs of informal care (valued using an opportunity cost approach and accounting for approximately 40%; Prince et al., 2015). Governments have identified the need to invest money to identify a cure for dementia and to delay onset of dementia. In 2013, the G7 (United States, Japan, Germany, France, United Kingdom, Italy, Canada) launched the “Global Action Against Dementia.” The initiative was designed to increase research funding, promote participation in trials, and enhance collaboration and data sharing. The group declared an ambition to identify a cure, or a disease modifying therapy for dementia by 2025. However, it has been acknowledged that this is an ambitious target and that we cannot and should not delay implementation of treatment and care that has been shown to be effective in improving outcomes for people with dementia (Prince et al., 2015). Although caregiver interventions may not be disease modifying, they have been shown to improve outcomes for both the person with dementia and their carer and there is some evidence of cost-effectiveness (Knapp, Iemmi, & Romeo, 2013).
Nonpharmacological interventions for people with dementia and their carers are heterogeneous in terms of content, dose, and the person delivering the treatment. Studies also involve participants with different severities of dementia and from different cultural backgrounds though the majority of studies were conducted in the United States. Pooling studies in the presence of clinical heterogeneity can be problematic but the reality in clinical practice is that most of these interventions are not replicated “as per protocol.” Clinicians are most likely to provide their own form of multicomponent intervention based on what they have been taught, their organizational culture, and their previous clinical experiences. The benefit of the meta-analyses presented within this review is that they provide an overall indication of the magnitude and types of effect. Indeed, a number of translational studies of caregiver interventions have demonstrated differences between intervention delivery in the context of a highly structured research trial and delivery in “real world” settings (Döpp, Graff, Rikkert, Nijhuis van der Sanden, & Vernooij-Dassen, 2013; Gitlin, Jacobs, & Earland, 2010).
In this review, we did not look at effects on all outcomes (e.g., service use) and we pooled different outcome measures to calculate the SMD, which is more difficult to interpret. We also did not conduct subgroup analyses based on intervention dose, content, and different populations. Subgroup analyses can be insightful but can also be difficult when considering complex interventions as it is hard to determine clinically meaningful cutoff points. For example, how should one compare low and high dose interventions when intervention duration within the studies is consistently spread between 2 and 10 hr?
One of the limitations of this review is that we used an existing systematic review to source studies published until 2008 and then updated searches for more recent studies. Thus, there were two slightly different methods used to source studies. The existing systematic review included all nonpharmacological interventions, whereas we were only interested in caregiver intervention. Our search term was developed based on terms used by the Cochrane Dementia and Cognitive Impairment Group and the BMJ Clinical Evidence terms for study design (British Medical Journal Clinical Evidence, 2016). Furthermore, we relied on the details describing the interventions provided in the publications to categorize studies. This may have led to us categorizing studies as being “education focused” or “support focused” and thus excluded from this review when they actually involved additional content that was poorly described or omitted.
In conclusion, there is a substantial body of evidence that multicomponent interventions can improve a range of important outcomes for both the person with dementia and his or her carer. There was no evidence that the dyadic approach offered an advantage.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: These authors gratefully acknowledge funding provided by the National Health and Medical Research Council (NHMRC) Partnership Centre on Dealing with Cognitive and Related Functional Decline in Older People (Grant No. GNT9100000).