
Abstract
Introduction
The demographics of the global population show that there is a trend toward an increased proportion of older adults aged ≥65 years as a result of improvements in health care, living standards, and socioeconomic status (Beard et al., 2016). Concurrent with this population profile change is the shift to a more positive perception of older people and their ongoing potential to contribute to society (Cuthill et al., 2016; Villar & Celdrán, 2013). An increasing proportion of people aged ≥65 years are learning new skills and increasing their knowledge base so they can continue to be competent and involved in their communities (del Pilar Díaz-López et al., 2016; Narushima et al., 2018a).
The World Health Organization (WHO) Active Ageing Framework (Cybulski et al., 2016; Narushima et al., 2018a; Villar & Celdrán, 2013) promotes health, participation, and security as the three key determinants of quality of life in older adults. This active ageing framework encourages lifelong learning in older adults so that they may retain or develop psychological and cognitive functionality that persists into later life. Active ageing in late adulthood has also been identified by the European Commission as an important educational objective to cope with potential labor shortages as well as improve an individual’s inclusion in the community (Di Gessa & Grundy, 2014). However, this is often referred to as “productive ageing” and has been criticized as a means for governments to prolong labor participation (Boudiny, 2013).
Learning in late adulthood goes beyond productive or active ageing and instead promotes healthy cognitive function, self-dependency, and a sense of social belonging through participation in educational interventions (Narushima et al., 2018a). There is a growing body of literature on the effects of participating in educational or learning activities in later life adults (Botes et al., 2019; Di Gessa & Grundy, 2014; Narushima et al., 2018a, 2018b; Somrongthong et al., 2017; Villar & Celdrán, 2013). These studies show dramatic improvements in health-related quality of life (QOL) and psychological wellbeing among adult learners who have participated in formal and non-formal (i.e., leisure type courses) educational activities. However, many of these studies have been limited by small sample sizes, the specifics of the educational course, or are related to a specific geographical area. As such, insights into the impact of later life education using pooled data from relevant outcomes such as cognitive health (Creavin et al., 2016; Folstein et al., 1975; Yesavage et al., 1982) and QOL (Ware and Gandek, 1998) are currently absent (Arai et al., 2012; Botes et al., 2019; Di Gessa & Grundy, 2014; Narushima et al., 2018b; Villar & Celdrán, 2013).
The overall objective of this study was to systematically review the literature and quantify the effect of later-life formal education or learning programs on QOL, mood, and cognitive function, compared with no later-life formal education or learning, in older adults. In general, formal education is defined as education that is institutionalized, intentional and planned through public organizations and recognized private bodies, whereas a learning program is defined as a coherent set or sequence of educational activities designed and organized to achieve pre-determined learning objectives or accomplish a specific set of educational tasks over a sustained period (United Nations Educational Scientific and Cultural Organization, 2011). However, although some studies have used a narrow interpretation of formal education as encompassing only learning which takes place in a designated institution, guided by a teacher or trainer, with the aim of attaining an officially recognized qualification (Villar & Celdrán, 2013), we undertook an expanded analysis to reflect the fact that some education and learning is offered in non-institutional settings (i.e., in the community and online).
Thus, the specific objectives of this systematic review and meta-analysis were to: review the type of educational interventions explored by adults aged ≥65 years; review and quantify the impact of these interventions on outcomes of interest in adults aged ≥65 years; identify the most effective interventions for a given subpopulation of older adults (stratified by demographics, cognitive health, access/level of education, and socioeconomic background); and identify knowledge gaps surrounding the impact of formal education/learning programs on adults aged ≥65 years and the need for future studies/intervention programs.
Methods
This study was reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009) and according to the Cochrane Handbook for Systematic Reviews of Interventions (Chandler et al., 2019). The Newcastle-Ottawa scale was used to assess the methodological quality of the studies included in this review.
Eligibility Criteria
Subjects of interest were adults aged ≥65 years who had undertaken some form of formal education or learning programs. Subjects could be residing in the community, care homes, residential homes, elderly care facilities, retirement homes, assisted living facilities, or nursing homes. Owing to a paucity of quantitative data in adults aged ≥65 years, the protocol was subsequently expanded to include subjects aged ≥55 years.
Interventions comprised any non-pharmacological intervention that was initiated before the subject was 65 years of age and was ongoing, or participation had been initiated after the subject was 65 years of age. The intervention included formal education or learning programs such as those offered through colleges, universities, adult learning centers, third age universities, or online learning platforms. The level of education undertaken could include degrees, diplomas, modules, courses, evening classes, lectures, seminars, or online distance learning, either alone or as a component of a multifaceted intervention, including cognitive exercise, and combined training. The comparator group comprised adults aged ≥65 years who had not participated in a formal education or learning program.
Studies included in the systematic review had one or more of the following outcomes of interest: activities of daily living, affective and behavioral symptoms (i.e., the Geriatric Depression Scale [Long and Short Forms]) (Yesavage et al., 1986), happiness, cognitive function (i.e., MMSE score) (Folstein et al., 1975), and QOL. Included studies were published in English, had the full text available, and were randomized controlled trials, prospective clinical trials, population-based cohort studies, or observational studies. All included studies were published between the date of database (PubMed and Scopus) inception and 30th September 2019.
Studies were excluded if they involved adults aged <65 years, were published in languages other than English, had no full text available or were conference abstracts, or did not investigate active participation of adults aged ≥65 in a formal education or learning program. Studies were also excluded if they involved pharmacological intervention for outcomes of interest. For example, if medication was started as part of a trial and was likely to affect outcomes of interest, the study was excluded. Following initial hierarchal data extraction, the protocol was expanded to include subjects aged ≥55 years.
Search Strategy and Study Selection
Electronic searches of the PubMed and Scopus databases were conducted from database inception until 30th September 2019. The full details of the search terms used for each database are provided as Supplemental Material.
Two reviewers independently conducted the research, screened all studies for eligibility, extracted data, and assessed the risks of bias for each included study. Bibliographies of all included studies were screened manually to identify any additional studies that may have been missed during the electronic searches. Any disagreements between the two reviewers were resolved by consensus or by consultation with a third reviewer.
Data Collection Process
Two reviewers extracted data independently. The DistillerSR systematic review software (Evidence Partners; Ottawa, Ontario, Canada) was used for data extraction from randomized controlled trials, prospective clinical trials, population-based cohort studies, and observational studies. The following data were extracted from all eligible studies: study ID, title, year of publication, country, study setting, sample size and study duration; sociodemographic characteristics—mean age (years), sex, employment status, household income, marital status, place of birth, place of residence, race and home status; intervention—frequency, duration, intensity and level of education or learning program; comparator group; health conditions; smoking status; alcohol consumption; physical activity status; ongoing medications; and outcome measures. If data for any of these parameters were not available for a given study, the corresponding authors were contacted to try to obtain the raw data or to provide further information. Where a study was published in duplicate, or there were companion documents or multiple reports of a primary study, all available data were collated to maximize information and the most complete dataset (aggregated across all publications) was used.
Risk of Bias
The Cochrane Community RoB 2.0 tool was used to assess the risk of bias for randomized controlled trials and non-randomized observational studies. Funnel plots and Egger’s test were analyzed closely to assess the bias statistically, together with cross-validation of the results (leave1out cross-validation).
Statistical Analysis
RStudio (Boston, MA, USA), RevMan version 5.3 (Cochrane Collaboration, 2014) and IBM SPSS version 21.0 (IBM Corp.; Armonk, NY, USA) software were used for all analyses. A meta-analysis was conducted for studies where at least 80% of data were available for the abovementioned data-extraction factors (see Section “Data Collection Process”) in 10 or more studies. All eligible studies were combined to give a relative risk for each of the outcomes studied. Data were pooled using a random-effects model to give the most conservative estimate. Software was used to generate forest plots of relative risk with the corresponding 95% confidence intervals (CIs). Covariates/adjustments were specified in the tables and forest plots. Where intervention and comparison data were both available, mean difference and standard deviation (SD) for continuous variables, and frequency or median (interquartile range) for categorical variables, with corresponding p values, were provided. Standard errors (SEs) were calculated using the formula SE = SD/√n, where n was the number of participants.
Overall pooled measure effects were calculated using the random-effects model of DerSimonian and Laird (1986). The generic inverse variance method was used to calculate overall effect size. Statistical heterogeneity between the studies was assessed using the I2 metric with cut-offs of 25%, 50%, and 75% to define low, moderate, and high heterogeneity, respectively.
Non-pooled analysis was conducted using forest plots with mean difference reference points for the accompanying CIs for the WHOQOL-BREF physical scale, Difficulties in Physical Functioning Scale (DFPS), balance as a physical ability characteristic, self-motivation for physical activity, and the Cuestionario Breve de Calidad de Vida (CUBRECAVI) ratings for satisfaction with life, objective health and functional skills. Leave1out cross-validation (with the R metafor package) was performed to cross-validate the results and further assess sensitivity of the meta-analysis and the risk of bias for the individual studies. All analyses were stratified by sex and type, and frequency and duration of intervention.
Meta-regression analysis was conducted to determine whether any of the abovementioned covariates (see Data collection process) had a significant impact on the summary estimates if data were available for three or more studies. p < .05 were considered statistically significant.
Results
Study Characteristics
Following the protocol expansion to include younger subjects (≥55 years) and the additional search terms, in order to obtain a meaningful amount of quantitative data for analysis, a total of 3,934 records were reviewed. Following title and abstract screening, 104 full-text articles were retrieved and reviewed, of which 32 studies met the inclusion criteria (Figure 1).
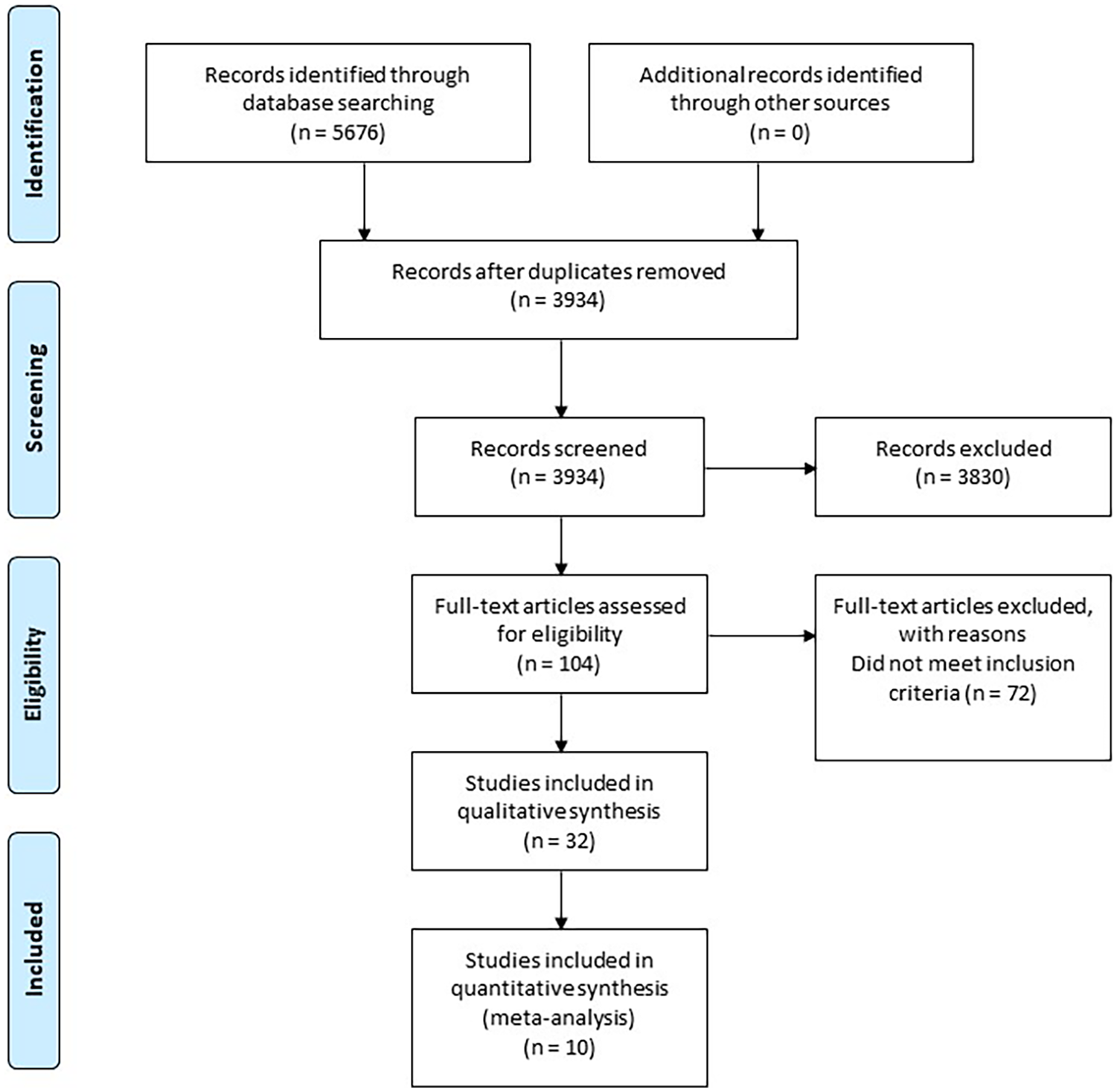
Study selection flow diagram.
Sample sizes varied greatly, ranging from 2 to 3,915 subjects (mean 234.09; SD 686.31) with an average age range of 64.30 to 83.60 years (Table 1). Sociodemographic details and other covariates of interest were reported infrequently and not uniformly: only two studies reported place of birth; four studies reported household income; nine studies reported employment status; nine studies reported race/ethnicity; 12 studies reported marital status; 15 studies reported home status; and 18 studies reported level of education (reported to varying degrees). No studies reported on a subject’s place of residence. Smoking history, alcohol consumption, physical activity, and details of ongoing medications were not reported in any study. Most studies were observational or qualitative in design (n = 15), followed by quasi-experimental design (n = 8) and randomized control (n = 8). One study used a non-experimental method that used a descriptive-correlational method through the study of surveys.
Study Design Characteristics.

Note. Sample size is the total number of subjects in the study.
The interventions studied incorporated the creative arts (n = 5), cognitive training (n = 9), computer and internet use (n = 6), health promotion and education (n = 3), and literacy (n = 1; Table 2, Supplemental Table 1). Eight studies did not report on a specific intervention but instead reported that subjects participated in various formal education courses. Eighteen studies reported a comparator group, which included no formal education/course participation, other/usual activities in place of intervention, or more specifically a group with no dementia or cognitive decline. Twenty-one studies used standard endpoints including baseline/pre-test measurement and sequential measurements at varying time points (post-test or subsequent follow up). The remaining studies used a single qualitative measurement (survey, interview or focus group) following completion of formal education. Fifty-five outcome measures were reported of which only eight were used more than once (Table 2). The most commonly used outcome measures were the MMSE (n = 11), the Geriatric Depression Scale (n = 5), the Life Satisfaction Scale (n = 4), and parameters that were measured using the Likert Scale (n = 4).
Subject and Intervention Characteristics.

Note. Outcome measures reported included: MMSE = Minimum Mental State Exam; GDS15 = Geriatric Depression Scale; LSS = Life satisfaction Scale; Likert Scale; UCLALS = UCLA Loneliness Scale; PCS = Perceived Control Scale; WHOQOL = World Health Organization-QOL; AVLT = Rey Auditory Verbal Learning Test; GDPS; SELF = Self Evaluation Life Function; NART = National Adult Reading Test; CSDD = Cornell Scale for Depression in Dementia; MOSES = Multi-Observational Scale for the Elderly; DPFS = Difficulties in Physical Functioning Scale; DACL = Depressive adjective checklist; SAS = Self-anchoring scale; RBMT = The Rivermead Behavioral Memory Test; TEA = Tests of Everyday Attention; Benton Fluency Task; Bond Lader Mood Scale; Structural Characteristics; Functional Characteristics; LGS = Loyola Generativity Scale; MIA = Memory in Adulthood Questionnaire; MCI = The Memory Controllability Inventory; CFT = Complex Figure Test; QLI = Quality of Life Index; EHQOL = EUROHIS-QOL; CUBRECAVI; Other outcome measures include, but are not limited to: CES-Depression Scale, TMT = Trail Making Test, 10word recall test (WRT), Verbal Fluency Test, general perceived self-efficacy test, Flourishing scale; Test Stroop Color; SDMT = Symbol Digit Modalities Test; Trail Making Test A; PASAT = Paced Auditory Serial Addition Test; Trail Making Test B; LNS = Letter–Number Sequencing of the WAIS-IV; Stroop color-word test; Matrix reasoning of the WAIS-IV, measures for respiratory function, time spent in group, general health questionnaire, participant observation, focus groups, interviews, questionnaires and surveys, correlations, memory performance tests, physical and cognitive functioning measures, and other models of statistical analysis.
Qualitative Analysis
Qualitative analysis revealed an increase in cognitive function across all types formal learning intervention (Dellefield & McDougall, 1996; Fu et al., 2018; Ivgi et al., 1999; Jo et al., 2018; Kinney & Rentz, 2005; Li et al., 2019; López-Higes et al., 2018; Mendoza-Ruvalcaba & Arias-Merino, 2015; Santos et al., 2014; Skrzek et al., 2015; Wang et al., 2018; Ward et al., 2018). In addition, there was an increased sense of self and life satisfaction and an increase in self-confidence or confidence with computer use. Subjects across eight studies revealed an increase in feelings of community, sociability, and pleasure following formal learning (Ellis, 2018; Kinney & Rentz, 2005; Mendoza-Ruvalcaba & Arias-Merino, 2015; Panayotoff, 1993; Richeson et al., 2007; Rusted et al., 2006; Sánchez-Nieto et al., 2019; Ullán et al., 2013). There was also a reduction in loneliness reported for three computer and internet training interventions (Blažun et al., 2012; Chilcott & Smith, 2011; White et al., 2002), while depression was reported to be reduced in four studies across various learning types (Rusted et al., 2006; Sánchez-Nieto et al., 2019; Shapira et al., 2007; White et al., 2002). Two studies reported that previous formal education, and higher education levels increased intervention success/adoption (Cutler et al., 2016; Richeson et al., 2007).
Meta-Analysis
From 32 studies, 10 studies were initially selected for meta-analysis based on MMSE scores and participation in formal education and learning programs for older adults. Measure effects were retrieved for all studies, and a pooled meta-analysis was performed on five studies (Fahmy et al., 2016; Jo et al., 2018; Li et al., 2019; López-Higes et al., 2018; Spector et al., 2003); note that two of the constituent studies (Jo et al., 2018; López-Higes et al., 2018) had two population samples, both of which were included, resulting in seven studies included in the pooled analysis.
Meta-analysis of 4,239 older adults (with or without dementia) revealed a significant pooled mean difference in MMSE score, before and after intervention with formal education and learning programs (Figure 2). The pooled mean difference for MMSE score before and after the intervention was 0.40, 95% CI = [0.12, 0.67], with a Z statistic value of 2.81 (p = .005; overall random-effects model). Heterogeneity was 99%, although study weights were not markedly different in the random-effects model. As two study subgroups were significantly larger (Jo et al., 2018), it should be noted that even though study weights were similar to those of other studies, 95% CIs were much narrower; thus, results from the Jo et al. (2018) study should be considered the most accurate in the meta-analysis.

Mean change in MMSE before and after intervention.
Risk of Bias
Funnel plot
The funnel plot (Figure 3) reveals divergent results; however, with three studies on both sides of the overall effect line and a symmetrical model, there is an indication of low publication bias. However, all studies are outside the funnel plot CI lines, which indicates a high risk of sampling bias and low statistical power for most studies. Thus, the funnel plot shows mixed results regarding two types of bias with a probable risk of a type II error present in the majority of studies.

Evaluation of publication bias.
Leave1out analysis
The overall pooled model remained statistically significant (p < .05) after exclusion of each study individually, except for the Jo et al. (2018) study (Table 3). This validates the funnel plot analysis and the assumption that the Jo et al. (2018) study is particularly relevant and is contributing the most to the overall statistically significant mean difference (p < .05). Heterogeneity in the meta-analysis is due to potential sampling bias, but also to considerable heterogeneity in educational and learning programs as interventions. Heterogeneity analysis reveals that interventions and populations, as well as study methodology, contribute to the 99% heterogeneity level. Therefore, it was justifiable to use the random effects model for estimation of the overall effect.
Leave1out Analysis.

Note. Two datasets were extracted from each of López-Higes et al. (2018) and Jo et al. (2018). CI = confidence interval; I2 = between-study heterogeneity; lb = lower bound; SE = standard error; Tau2 = tau value for heterogeneity; ub = upper bound.
Egger’s regression test
The Egger’ regression test confirmed the previous bias analysis results for the overall model. In this mixed-effects meta-regression model, the test for funnel plot asymmetry was statistically significant (z = 2.215, p = .027), thus indicating a statistically significant result for bias. Together with the original funnel plot and the large CIs in most studies, the results of the Egger’s regression test indicate sampling bias (i.e., the samples were too small). However, the overall effect is statistically significant primarily because of the Jo et al. (2018) study.
Non-pooled analysis
Four studies with multiple measure effects were selected for the non-pooled analysis (Carvalho-Loures et al., 2010; del Pilar Díaz-López et al., 2016; Mendoza-Ruvalcaba & Arias-Merino, 2015; Shapira et al., 2007). There was a general trend toward improvement in physical outcomes after educational and learning programs compared with baseline (Figure 4). For example, the WHOQOL-BREF physical scale score mean change was −0.33 (SE = 1.55) in one study (Carvalho-Loures et al., 2010), and DFPS mean score change was −3.54 (SE = 0.85) in another (Shapira et al., 2007). Other mean score changes were: 0.33 (SE = 0.53) for balance and 1.1 (SE = 0.25) for self-motivation for physical activity in one study (Mendoza-Ruvalcaba & Arias-Merino, 2015), and 0.44 (SE = 0.06), 0.22 (SE = 0.04), and 0.16 (SE = 0.07) for CUBRECAVI ratings for satisfaction with life, objective health, and functional skills, respectively, in another study (del Pilar Díaz-López et al., 2016). The particularly small CI for the CUBRECAVI score for objective health indicated a significant result.

Non-pooled analysis of education and learning interventions.
Discussion
This systematic review of the literature quantified the effect of later-life formal education and learning or learning programs on QOL, wellbeing, mood, and cognitive function, compared with no such participation. Our meta-analysis revealed a statistically significant indication that educational programs have a positive effect on MMSE scores in older adults; however, more studies are needed to confirm this finding. In addition, a non-pooled analysis showed that there were trends in the outcome measures across four studies (Carvalho-Loures et al., 2010; del Pilar Díaz-López et al., 2016; Mendoza-Ruvalcaba & Arias-Merino, 2015; Shapira et al., 2007). These studies showed that participation in formal education can have a significantly positive impact on several domains of wellbeing, including quality of life, physical functioning (including balance), life satisfaction, and objective health.
This qualitative review of the literature supports previous findings that participation in later-life learning contributed to aspects of enjoyment, learning, increased wellbeing and quality of life, and promotes healthy cognitive function, self-dependency, and a sense of belonging (Narushima et al., 2018a). Older adults are known to be at risk of loneliness and depression, due to both declining health and reduced social functioning abilities, and to changes in family life and domestic arrangements (for example, loss of a partner or relocation to a care home) (Berg-Weger & Morley, 2020; O’Rourke et al., 2018). Although estimates of loneliness prevalence vary considerably due to heterogeneous population samples and a lack of standardized measurement approaches, 20% to 30% of older adults report loneliness at least some of the time (Ong et al., 2016). In turn, loneliness/social isolation and depression are closely associated with poor health outcomes, including development of dementia (Sutin et al., 2018), increased levels of health care utilization (Stall et al., 2019), and premature mortality, particularly in older men (Holt-Lunstad et al., 2015; Holwerda et al., 2016). Many interventions have been developed to address a lack of social connectedness, with an emphasis on interpersonal contact, purposeful participation, and personal development (Freedman & Nicolle, 2020; O’Rourke et al., 2018). Undertaking education and learning is one way of addressing these needs, and our review of the literature indicated that participation in computer and internet training courses can reduce loneliness and depression (Shapira et al., 2007; Tatnall, 2014). Furthermore, we also show that education in information and communication promotes feelings of being in control and increases quality of life satisfaction more than those who were engaged in other non-computer-based activities (Shapira et al., 2007). These findings support that education in information and communication technologies can foster social relationships as well as increase leisure and entertainment opportunities (Tatnall, 2014).
Learning can also help vulnerable and older individuals maintain a quality of life despite chronic illness and functional difficulties (Narushima et al., 2018b), and this study highlights that formal educational interventions are particularly relevant to people with dementia or cognitive decline. It is generally agreed that a longer duration of formal childhood schooling and university education appears to provide some protection against cognitive decline and dementia in later years (Dekhtyar et al., 2015; Perneczky, 2019). However, recent research shows that maintaining the so-called “cognitive reserve” via intellectual occupations, engagement in leisure and social activities, and ongoing educational activities throughout adult life is also important (Peeters et al., 2020; Sauter et al., 2019). Furthermore, the promotion of cognitive reserve may be able to mitigate even genetic risk for the development of dementia (Dekhtyar et al., 2019; Mazzeo et al., 2019). Current pharmacologic treatments for dementia provide only modest symptomatic relief, and non-pharmacologic management including cognitively engaging activities may provide just as much benefit for patients (Arvanitakis et al., 2019). Specifically, following formal cognitive stimulation, the improvements in cognitive function in older adults have been found to be comparable with those obtained in trials of drugs for dementia (Spector et al., 2003). The qualitative findings from one study that used focus group interviews showed that participants had a greater understanding of their own memory and felt that it was not as bad as previously perceived (Richeson et al., 2007). In another study it was reported that healthy aging for people with dementia can be achieved or enhanced through the use of digital gaming technologies (Cutler et al., 2016), which shows that the specific nature of formal education can be varied and still yield positive results. These findings are also supported by the results of the present pooled meta-analysis.
The inadequacy and complexity of measuring quantitative outcomes at several points in time can be attributed to the independent variable of education and the dependent variable of health (often important in older populations) (Panayotoff, 1993); therefore, a qualitative approach to analysis is advised and this is reflected in the study designs and results of the reviewed literature. Similar difficulties with quantitative outcome measures have been reported, which cite complications with access, tracking participants, and the complexity of information required to capture wellbeing in a questionnaire (Hafford-Letchfield & Lavender, 2015). Such data cannot be stabilized and meaningfully interpreted, and therefore it is difficult to disentangle the respective roles of multiple factors in a qualitative study (Jenkins & Mostafa, 2012). This is reflected in the present study, where only 19% of studies that met the inclusion criteria had data suitable for a pooled meta-analysis. Despite a significant number of studies reporting pre- and post-test outcomes, these measures were often not statistically comparable between studies, except for those included in the meta-analysis. This is compounded by the observational nature of many of the studies, where results were derived from interviews, focus groups, subjective questionnaires, or Likert scales. Future studies of this nature should consider streamlining the design and employing validated outcome measures. Additional gaps in the published literature relate to the specific definitions of formal, non-formal and informal education, learning, or training intervention, and the lack of an accountable tool for measuring the outcome of those procedures. Researchers planning future evidence-based studies must ensure clarity in the methodology, and in the domain(s) in which improvement is anticipated as a result of the intervention.
Sociodemographic data were often reported non-uniformly, making it difficult to draw statistically significant conclusions on the effect of formal education with respect to covariates of interest. However, two studies in this review reported older participants who had engaged in higher education prior to joining a life-long learning program and as such reported a higher generative interest and satisfaction (Muñoz-Rodríguez et al., 2019; Wang et al., 2018). This confirms that prior attainment of education is a strong predictor of participation in any kind of learning activity.
Our adjustment to reduce the age for inclusion to ≥55 years in addition to expanding the search terms used, increased the number of studies for which quantitative data were available for meta-analysis. The reduction in inclusion age criteria is appropriate, as formal learning programs were initially catered for people over the age of 65 years, who had mostly passed the age of retirement. In contrast, those currently taking part in lifelong learning are adults who are increasingly younger (Muñoz-Rodríguez et al., 2019). Owing to the qualitative nature of most studies included, it was not possible to meet all of the original objectives of this study.
Limitations
Although there is a low risk of publication bias, there is a high risk of sampling bias and a type II error risk is rated as probable in most studies included in our analyses. This is because most of the studies are observational, the datasets have small sample sizes, and the only commonality across studies is that subjects participated in some form of formal education. However, these limitations confirm the complexities that are associated with quantifying multiple factors from qualitative studies (Jenkins & Mostafa, 2012).
Conclusions
This systematic literature review both qualifies and quantifies the positive impact of participation in formal education or learning in older people. After taking into account the caveats around study heterogeneity and statistical bias, these findings nonetheless support previous research, which suggested that participation in later-life learning contributes to increased wellbeing and quality of life, healthy cognitive function, self-dependency, and a sense of belonging. This meta-analysis also suggests that the benefits of later-life learning are likely independent of the type of intervention. Finally, while traditionally older learners are ≥65 years, participants in lifelong learning are increasingly becoming younger.
Supplemental Material
sj-pdf-1-ggm-10.1177_2333721420986027 – Supplemental material for How Does Participation in Formal Education or Learning for Older People Affect Wellbeing and Cognition? A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-pdf-1-ggm-10.1177_2333721420986027 for How Does Participation in Formal Education or Learning for Older People Affect Wellbeing and Cognition? A Systematic Literature Review and Meta-Analysis by Cory Noble, Darko Medin, Zara Quail, Charles Young and Mark Carter in Gerontology and Geriatric Medicine
Supplemental Material
sj-pdf-2-ggm-10.1177_2333721420986027 – Supplemental material for How Does Participation in Formal Education or Learning for Older People Affect Wellbeing and Cognition?: A Systematic Literature Review and Meta-Analysis
Supplemental material, sj-pdf-2-ggm-10.1177_2333721420986027 for How Does Participation in Formal Education or Learning for Older People Affect Wellbeing and Cognition?: A Systematic Literature Review and Meta-Analysis by Cory Noble, Darko Medin, Zara Quail, Charles Young and Mark Carter in Gerontology and Geriatric Medicine
Footnotes
Acknowledgements
The authors would like to acknowledge Gill Livingston and Anne Laybourne for their peer review and feedback on the initial systematic review protocol.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Zara Quail, Charles Young, and Mark Carter are employees of Care Visions Limited. Cory Noble and Darko Medin are employees of Edanz Group Japan Inc, who were engaged by Care Visions Limited to assist with the systematic review, the meta-analysis, and writing of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was funded internally by Care Visions Limited as part of their research program.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.